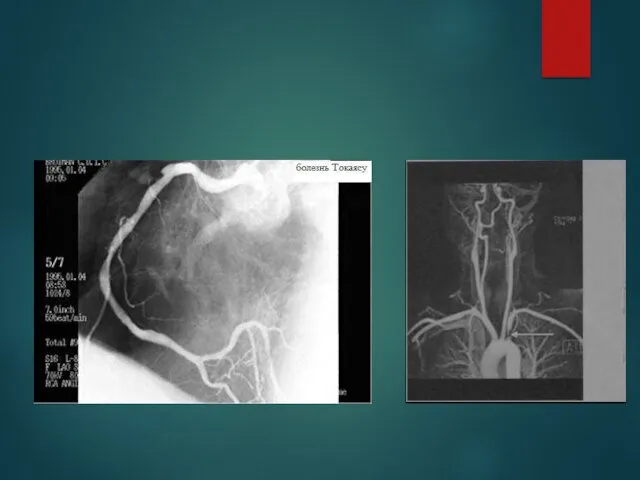
- Takayasu’s arteritis

Содержание
- 2. EPIDEMIOLOGY More case reports from Japan ,India, South-east Asia, Mexico No geographic restriction No race –
- 3. Age Mc-2nd & 3rd decade May range from infancy to middle age Indian studies-age 3- 50
- 4. Genetics Japan - HLA-B52 and B39 Mexican and Colombian patients - HLA-DRB1*1301 and HLA-DRB1*1602 India- HLA-
- 5. Histopathology Idiopathic c/c infla arteritis of elastic arteries resulting in occlusive &/ ectatic changes Large vessels,
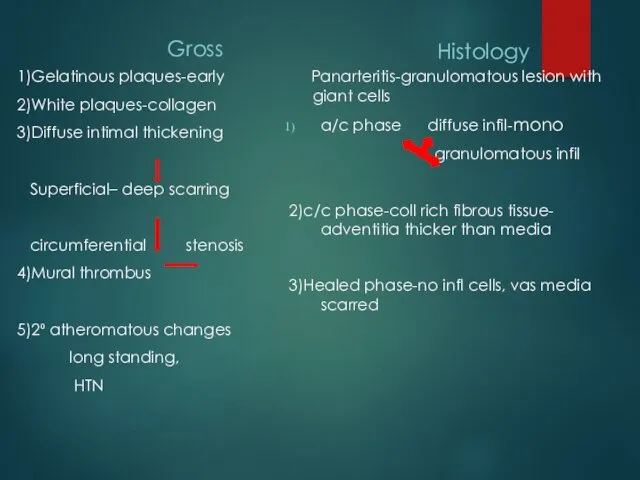
- 7. Gross 1)Gelatinous plaques-early 2)White plaques-collagen 3)Diffuse intimal thickening Superficial– deep scarring circumferential stenosis 4)Mural thrombus 5)2⁰
- 8. Wall thickening, Fibrosis, Stenosis, & Thrombus formation →end organ ischaemia More a/c inflammation → destroys arterial
- 9. Associated pathology-TB (LN)-55% Erthema multiforme Bazins disease(eryt induratum) churg strauss synd reteroperitoneal fib PAN,UC,CD etc
- 10. Clinical features Early pre pulseless/gen manif Fever,weight loss,headache, fatigue,malaise,night sweats, arthralgia +/_ splenomegaly/ cervical, axillary lymphadenopathy
- 12. Coronary involvement in TA Occurs in 10~30% Often fatal Classified into 3 types Type1:stenosis or occlu
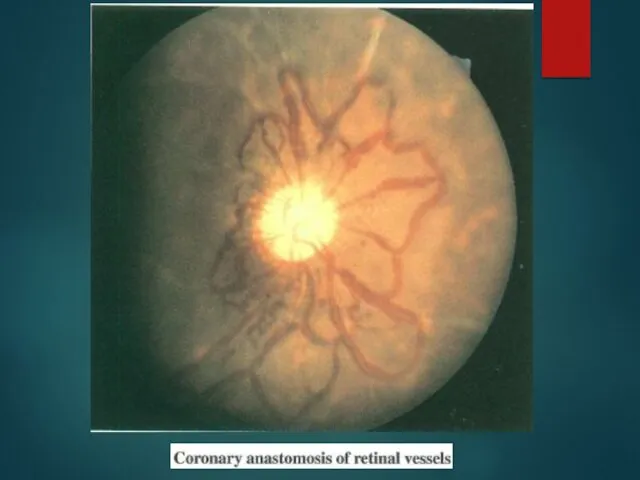
- 13. Occular involvement-Amaurosis fugax, pain behind eye, no real visual loss Hypertensive retinopathy Commonest Arteriosclerotic –art narrowing,
- 15. HTN is the most characteristic manifestation in Indian patients,suggesting a high frequency of lesions in the
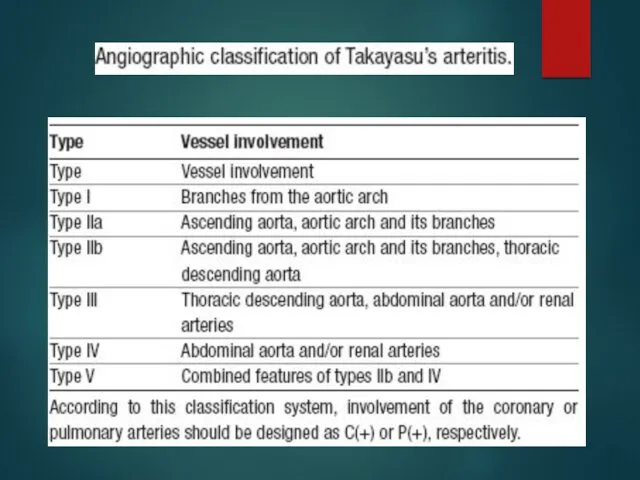
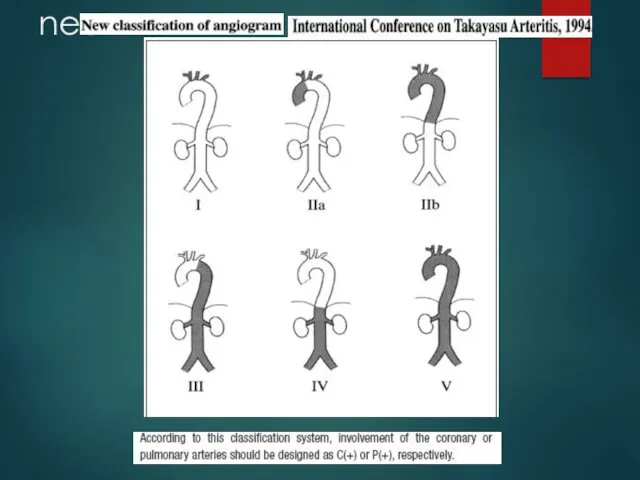
- 16. Ishikawa clinical classification of Takayasu arteritis 1978 4 Complications Retinopathy, Secondary HTN, AR, & Aneurysm
- 18. Cumulative survival 5years -91% (event free survival -74.9%) 10 years -84% (event free survival -64%) Single
- 19. 1990
- 20. 1995
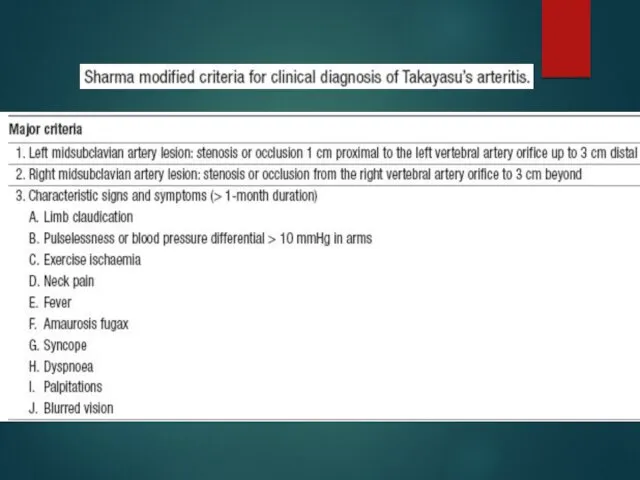
- 21. Sharma BK, Jain S, Suri S, Numano F. Diagnostic criteria for Takayasu arteritis. Int J Cardiol
- 23. nee
- 24. a/c phase-Axial T1-weighted image wall thickening of As aorta and PA Axial T1-weighted image- improvement of
- 25. Findings of TA on MRI mural thrombi signal alterations within and surrounding inflamed vessels vascular dilation
- 26. [18F]fluorodeoxyglucose PET for diagnosing Takayasu’s arteritis common [18F]FDG uptake pattern TA early phase - linear and
- 27. remission after treatment
- 28. Treatment of TA ・ Steroids immunosuppressants: Cyclosporine,Cyclophosphamide, Mtx,Mycophenolate mofetil Anti-platelet therapy(low-dose Aspirin) angioplasty/surgery If uncontrolled Control
- 29. Medical treatment 0.7-1 mg/kg/day –prednisolone for 1-3 months common tapering regimen once remission ↓ pred by
- 30. Steroids → 50% response Methotrexate →further 50% respond 25% with active disease will not respond to
- 31. Critical issue is in trying to determine whether or not disease is active During Rx- regular
- 32. chronic phase- persistent inflammation steroids should be continued –
- 33. Surgical treatment HTN with critical RAS Extremity claudication limiting daily activities Cerebrovascular ischaemia or critical stenoses
- 34. Surgical techniques Carry high morbidity & mortality Steno /aneurysm -anastomotic points Progressive nature of TA Diffuse
- 35. Renal artery involvement Best treated by PTA Stent placement following PTA Ostial lesions Long segment lesions
- 36. ostial stenosis of the right renal artery after deployment of a stent
- 37. Renal PTA - 33 stenoses (20 pts) Indi-sev HTN,angio 70% stenosis with pr grad 20mm, nl-ESR
- 38. Aortoarteritic lesions Balloon dilation safe & reasonably effective Can be performed repeatedly without any added risks
- 39. Left subclavian angiograms- 95% stenosis with extensive collaterals Post angioplasty and stenting.
- 40. Joseph s et al, SCT J Vasc Interv Radiol 1994;5:573–580 PTA- Scl A in TA 24
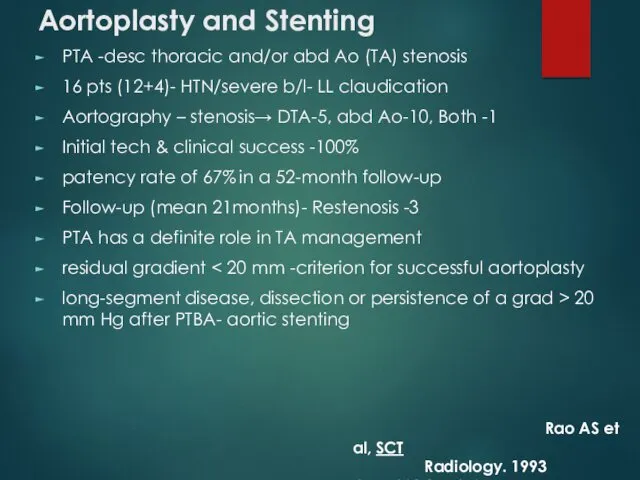
- 41. Aortoplasty and Stenting PTA -desc thoracic and/or abd Ao (TA) stenosis 16 pts (12+4)- HTN/severe b/l-
- 42. long-segment diffuse stenotic involvement of the DTA after deployment of stents.
- 43. Treatment for cor A occulusion in TA Surgery (CABG)- often not indicated ・IMA can’t be used
- 45. Скачать презентацию
EPIDEMIOLOGY
More case reports from Japan ,India, South-east Asia, Mexico
No geographic restriction
No
EPIDEMIOLOGY
More case reports from Japan ,India, South-east Asia, Mexico
No geographic restriction
No
Age
Mc-2nd & 3rd decade
May range from infancy to middle
Age
Mc-2nd & 3rd decade
May range from infancy to middle
Genetics
Japan - HLA-B52 and B39
Mexican and Colombian patients
Genetics
Japan - HLA-B52 and B39
Mexican and Colombian patients
Histopathology
Idiopathic c/c infla arteritis of elastic arteries resulting in occlusive &/
Histopathology
Idiopathic c/c infla arteritis of elastic arteries resulting in occlusive &/
Gross
1)Gelatinous plaques-early
2)White plaques-collagen
3)Diffuse intimal thickening
Superficial– deep scarring
circumferential stenosis
4)Mural
Gross
1)Gelatinous plaques-early
2)White plaques-collagen
3)Diffuse intimal thickening
Superficial– deep scarring
circumferential stenosis
4)Mural
Wall thickening, Fibrosis, Stenosis, & Thrombus formation →end organ ischaemia
More a/c
More a/c
Associated pathology-TB (LN)-55%
Erthema multiforme
Bazins disease(eryt induratum)
churg strauss synd
Associated pathology-TB (LN)-55%
Erthema multiforme
Bazins disease(eryt induratum)
churg strauss synd
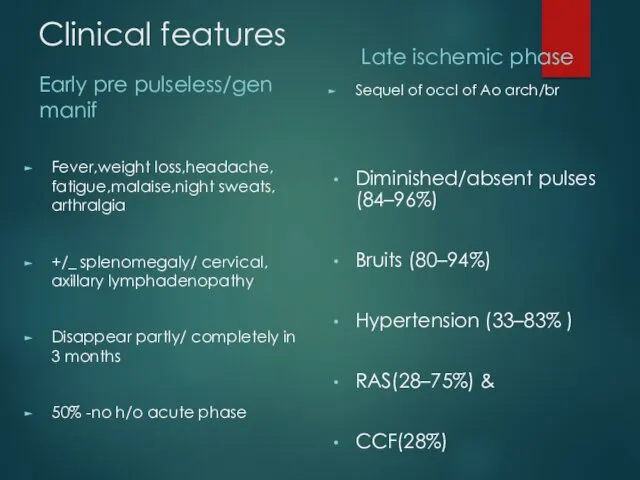
Clinical features
Early pre pulseless/gen manif
Fever,weight loss,headache, fatigue,malaise,night sweats, arthralgia
+/_ splenomegaly/ cervical,
Clinical features
Early pre pulseless/gen manif
Fever,weight loss,headache, fatigue,malaise,night sweats, arthralgia
+/_ splenomegaly/ cervical,
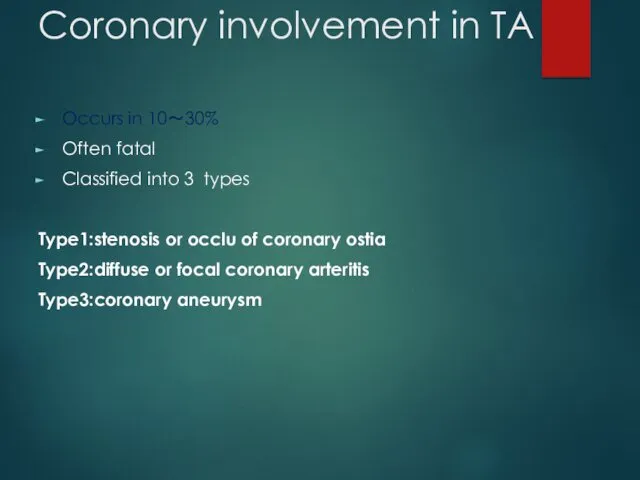
Coronary involvement in TA
Occurs in 10~30%
Often fatal
Classified into 3 types
Type1:stenosis or
Coronary involvement in TA
Occurs in 10~30%
Often fatal
Classified into 3 types
Type1:stenosis or
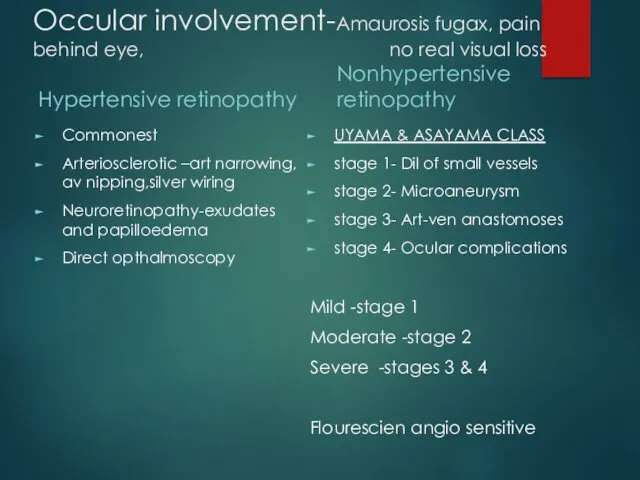
Occular involvement-Amaurosis fugax, pain behind eye, no real visual loss
Hypertensive retinopathy
Commonest
Arteriosclerotic
Occular involvement-Amaurosis fugax, pain behind eye, no real visual loss
Hypertensive retinopathy
Commonest
Arteriosclerotic
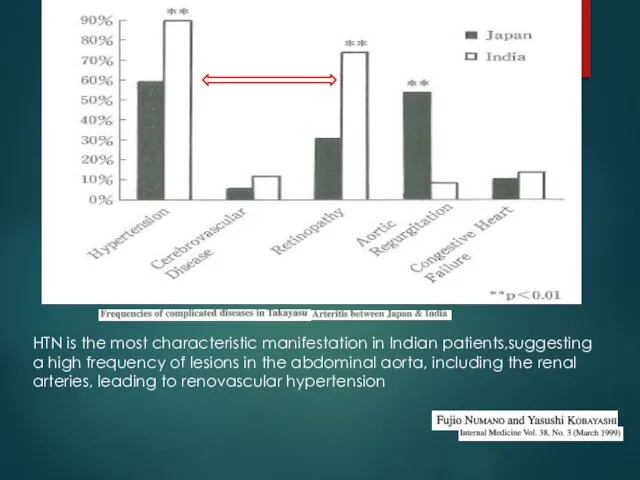
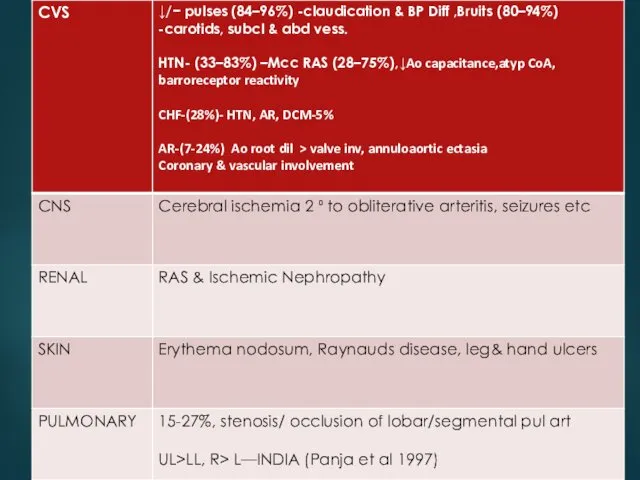
HTN is the most characteristic manifestation in Indian patients,suggesting a high
HTN is the most characteristic manifestation in Indian patients,suggesting a high
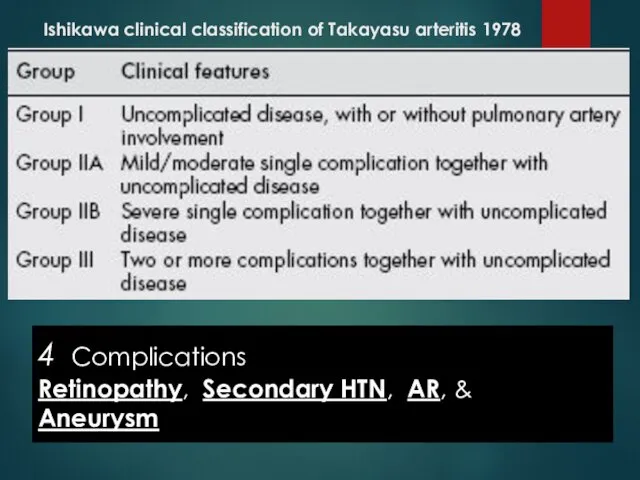
Ishikawa clinical classification of Takayasu arteritis 1978
4 Complications
Retinopathy, Secondary HTN,
Ishikawa clinical classification of Takayasu arteritis 1978
4 Complications
Retinopathy, Secondary HTN,
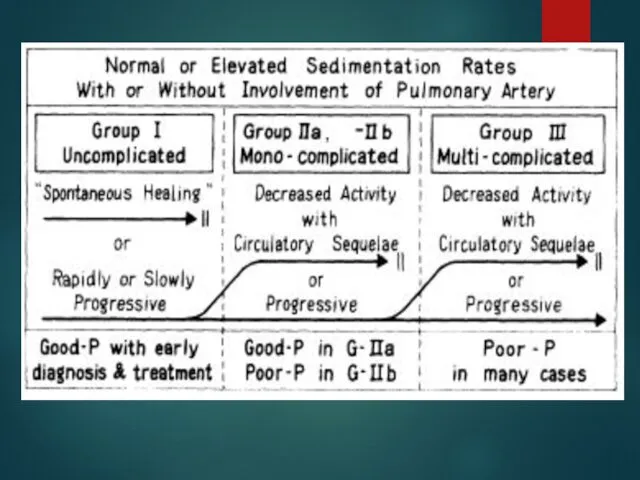
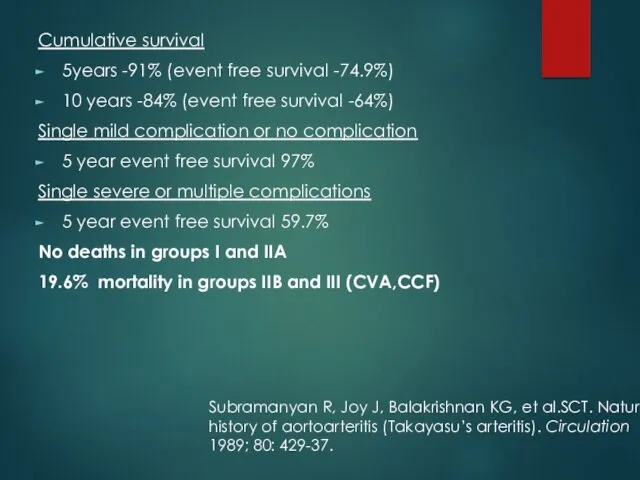
Cumulative survival
5years -91% (event free survival -74.9%)
10 years -84% (event
Cumulative survival
5years -91% (event free survival -74.9%)
10 years -84% (event
1990
1990
1995
1995
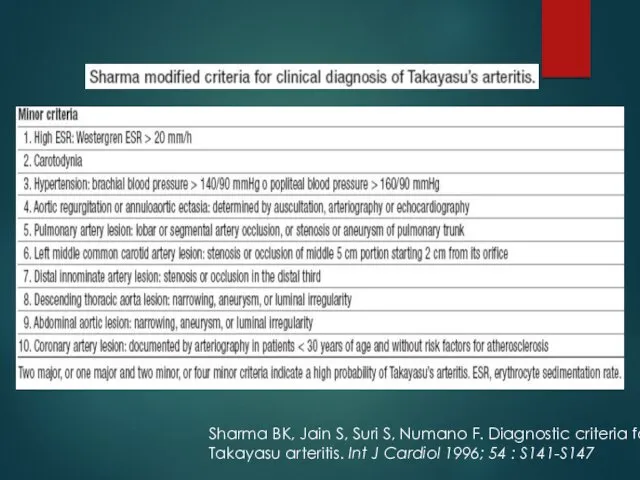
Sharma BK, Jain S, Suri S, Numano F. Diagnostic criteria for
Takayasu
Sharma BK, Jain S, Suri S, Numano F. Diagnostic criteria for
Takayasu
nee
nee
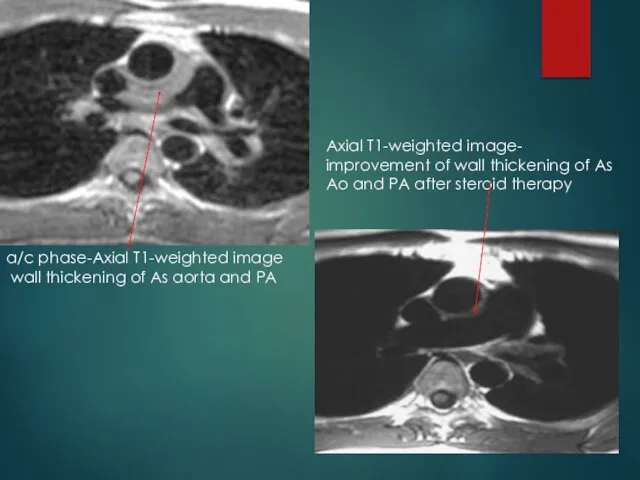
a/c phase-Axial T1-weighted image
wall thickening of As aorta and
a/c phase-Axial T1-weighted image
wall thickening of As aorta and
Findings of TA on MRI
mural thrombi
signal alterations within
Findings of TA on MRI
mural thrombi
signal alterations within
![[18F]fluorodeoxyglucose PET for diagnosing Takayasu’s arteritis common [18F]FDG uptake pattern](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/19592/slide-25.jpg)
[18F]fluorodeoxyglucose PET for diagnosing
Takayasu’s arteritis
common [18F]FDG uptake pattern TA
early phase
[18F]fluorodeoxyglucose PET for diagnosing
Takayasu’s arteritis
common [18F]FDG uptake pattern TA
early phase

remission after treatment
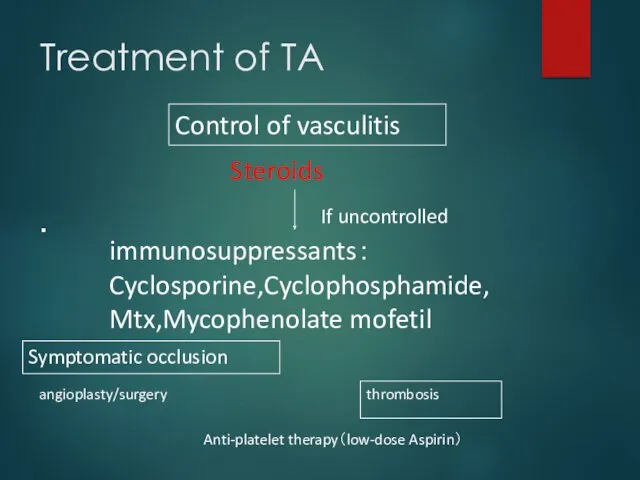
Treatment of TA
・
Steroids
immunosuppressants:
Cyclosporine,Cyclophosphamide,
Mtx,Mycophenolate mofetil
Anti-platelet therapy(low-dose Aspirin)
angioplasty/surgery
If uncontrolled
Control of vasculitis
Symptomatic occlusion
thrombosis
Treatment of TA
・
Steroids
immunosuppressants:
Cyclosporine,Cyclophosphamide,
Mtx,Mycophenolate mofetil
Anti-platelet therapy(low-dose Aspirin)
angioplasty/surgery
If uncontrolled
Control of vasculitis
Symptomatic occlusion
thrombosis
Medical treatment
0.7-1 mg/kg/day –prednisolone for 1-3 months
common tapering regimen once
Medical treatment
0.7-1 mg/kg/day –prednisolone for 1-3 months
common tapering regimen once
Steroids → 50% response
Methotrexate →further 50% respond
25% with active disease will
Steroids → 50% response
Methotrexate →further 50% respond
25% with active disease will
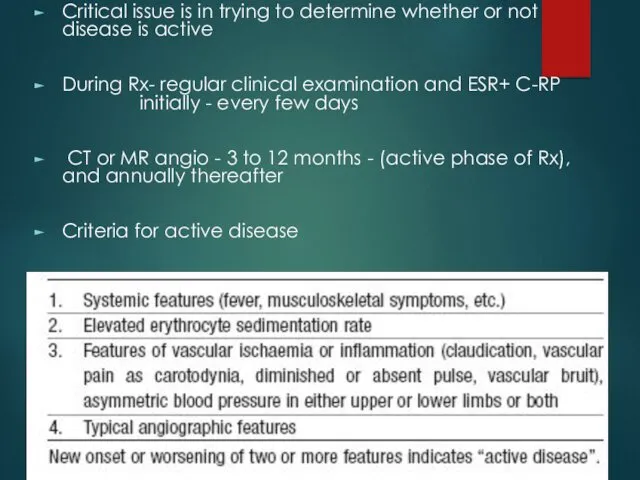
Critical issue is in trying to determine whether or not disease
Critical issue is in trying to determine whether or not disease
chronic phase- persistent inflammation
steroids should be continued –
chronic phase- persistent inflammation
steroids should be continued –
Surgical treatment
HTN with critical RAS
Extremity claudication limiting daily activities
Cerebrovascular ischaemia or
Surgical treatment
HTN with critical RAS
Extremity claudication limiting daily activities
Cerebrovascular ischaemia or
Surgical techniques
Carry high morbidity & mortality
Steno /aneurysm -anastomotic points
Progressive nature
Surgical techniques
Carry high morbidity & mortality
Steno /aneurysm -anastomotic points
Progressive nature
Renal artery involvement
Best treated by PTA
Stent placement following PTA
Ostial lesions
Long segment
Renal artery involvement
Best treated by PTA
Stent placement following PTA
Ostial lesions
Long segment

ostial stenosis of the right renal artery
after deployment of a stent
ostial stenosis of the right renal artery
after deployment of a stent
Renal PTA - 33 stenoses (20 pts)
Indi-sev HTN,angio 70% stenosis
Renal PTA - 33 stenoses (20 pts)
Indi-sev HTN,angio 70% stenosis
Aortoarteritic lesions
Balloon dilation
safe & reasonably effective
Can be performed repeatedly without
Aortoarteritic lesions
Balloon dilation
safe & reasonably effective
Can be performed repeatedly without
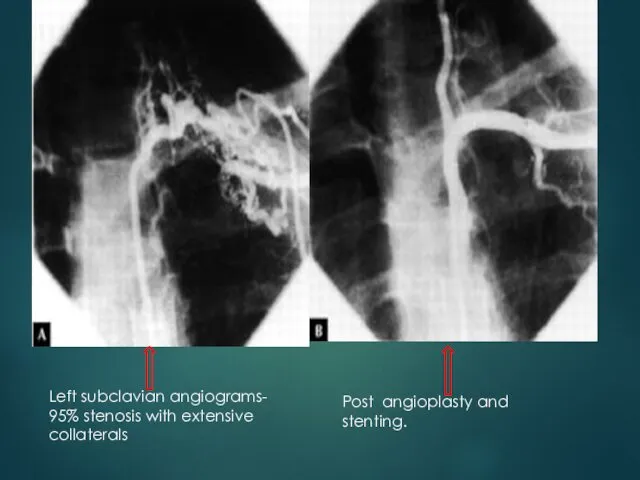
Left subclavian angiograms- 95% stenosis with extensive collaterals
Post angioplasty and
Left subclavian angiograms- 95% stenosis with extensive collaterals
Post angioplasty and
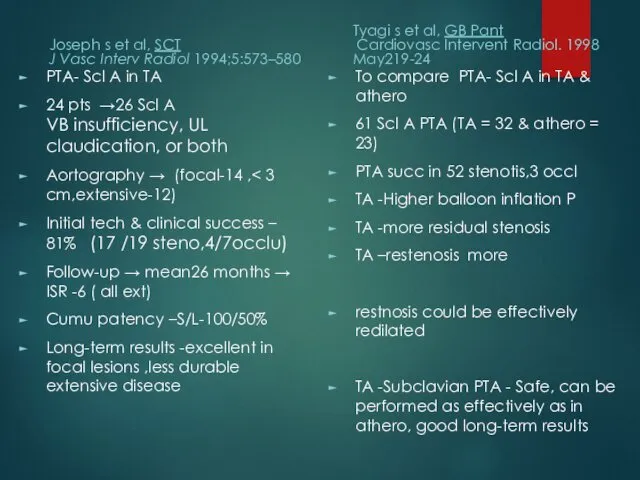
Joseph s et al, SCT
J Vasc Interv Radiol 1994;5:573–580
PTA- Scl A
Joseph s et al, SCT
J Vasc Interv Radiol 1994;5:573–580
PTA- Scl A
Aortoplasty and Stenting
PTA -desc thoracic and/or abd Ao (TA) stenosis
16 pts
Aortoplasty and Stenting
PTA -desc thoracic and/or abd Ao (TA) stenosis
16 pts
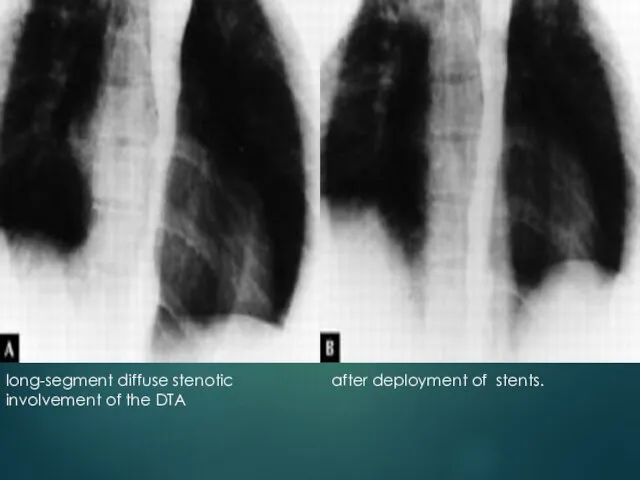
long-segment diffuse stenotic involvement of the DTA
after deployment of stents.
long-segment diffuse stenotic involvement of the DTA
after deployment of stents.
Treatment for cor A occulusion in TA
Surgery (CABG)- often not indicated
・IMA
Treatment for cor A occulusion in TA
Surgery (CABG)- often not indicated
・IMA
 Флавоноидтар
Флавоноидтар Феохромоцитома
Феохромоцитома Организация здравоохранения в зарубежных странах. Страховая, бюджетная и частная системы здравоохранения
Организация здравоохранения в зарубежных странах. Страховая, бюджетная и частная системы здравоохранения Стенокардия. Причины сердечных приступов
Стенокардия. Причины сердечных приступов Косметикалық кабинеттердің құрылымына және жұмысына қойылатын гигиеналық талаптары
Косметикалық кабинеттердің құрылымына және жұмысына қойылатын гигиеналық талаптары Воспаление. Ответ острой фазы
Воспаление. Ответ острой фазы Hemorrhagic syndromes of newborns
Hemorrhagic syndromes of newborns Вторичный метаболизм высших растений. Сапонины и минорные вторичные метаболиты
Вторичный метаболизм высших растений. Сапонины и минорные вторичные метаболиты Семиотика поражения органов кровообращения у детей
Семиотика поражения органов кровообращения у детей Клещевой энцефалит
Клещевой энцефалит Что такое отек. Виды и причины отеков, методы лечения
Что такое отек. Виды и причины отеков, методы лечения Жыныстық ажыратылу физиологиясы және жыныс бездері функциясының жас ерекшелігіне қатысты өзгерістері
Жыныстық ажыратылу физиологиясы және жыныс бездері функциясының жас ерекшелігіне қатысты өзгерістері Рецептура. Тема № 10
Рецептура. Тема № 10 Диполь. Электрическое поле диполя. Понятие об ЭКГ, теория отведений Эйнтховена для электрокардиографии. Лекция 5
Диполь. Электрическое поле диполя. Понятие об ЭКГ, теория отведений Эйнтховена для электрокардиографии. Лекция 5 Физические принципы действия диагностики УЗИ
Физические принципы действия диагностики УЗИ Наследственно – дегенеративные заболевания нервной и нервно-мышечной систем
Наследственно – дегенеративные заболевания нервной и нервно-мышечной систем ВОП планирование семьи и репродуктивное сохранение здоровья. Пренатальная генетическая оценка и рекомендации
ВОП планирование семьи и репродуктивное сохранение здоровья. Пренатальная генетическая оценка и рекомендации Превентивная фитотерапия инфекционных заболеваний
Превентивная фитотерапия инфекционных заболеваний Зоонози
Зоонози Актуализация формулярной системы в гериатрическом стационаре
Актуализация формулярной системы в гериатрическом стационаре Транспозиция сухожилий (реконструкция при повреждениях периферических нервов)
Транспозиция сухожилий (реконструкция при повреждениях периферических нервов) Травматические повреждения женских половых органов
Травматические повреждения женских половых органов Туберкулез лимфатических узлов
Туберкулез лимфатических узлов Общая этиология и общий патогенез эндокринопатий
Общая этиология и общий патогенез эндокринопатий Патофизиология сердечной недостаточности
Патофизиология сердечной недостаточности Болезнь Берже
Болезнь Берже Неотложные состояния в неврологии
Неотложные состояния в неврологии Лимфедема конечностей
Лимфедема конечностей