- Pericardial diseases

Содержание
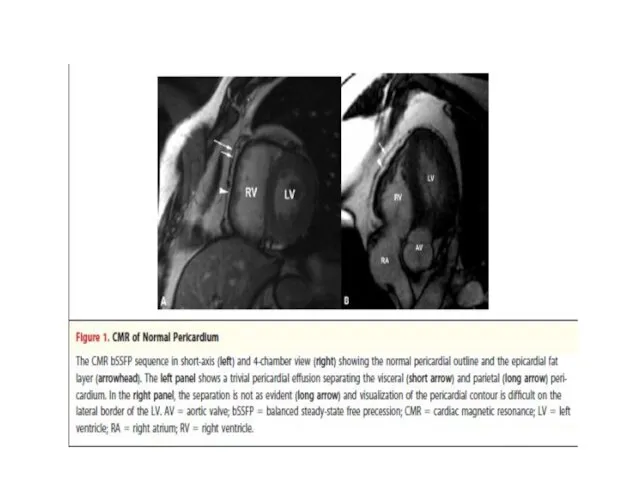
- 2. Pericard : anatomical and physyological considerations Outer layer - fibrous pericardium Inner layer - serous or
- 3. Pericardial fluid In normal hearts there is a small amount of pericardial fluid (25-50 ml) Produced
- 4. Most common forms of pericardial syndromes Acute and recurrent pericarditis Pericardial effusion Cardiac tamponade Constrictive pericarditis
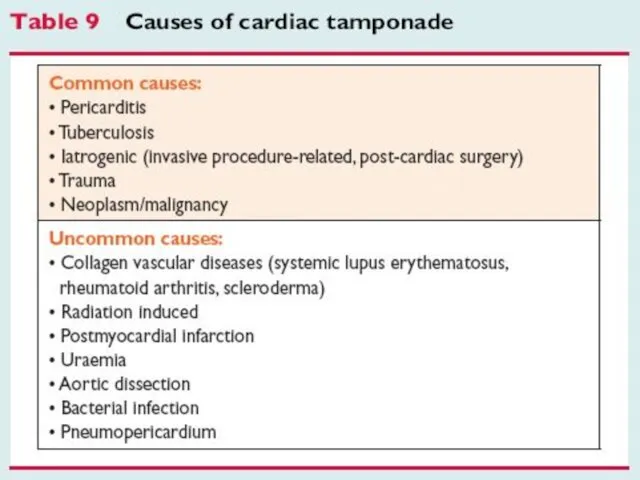
- 6. Etiology
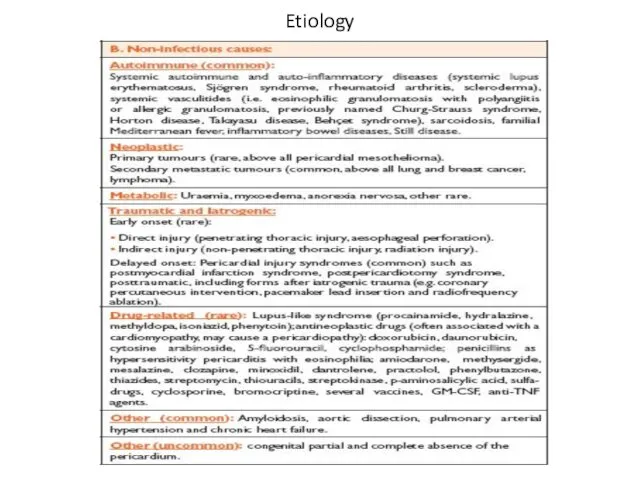
- 7. Etiology
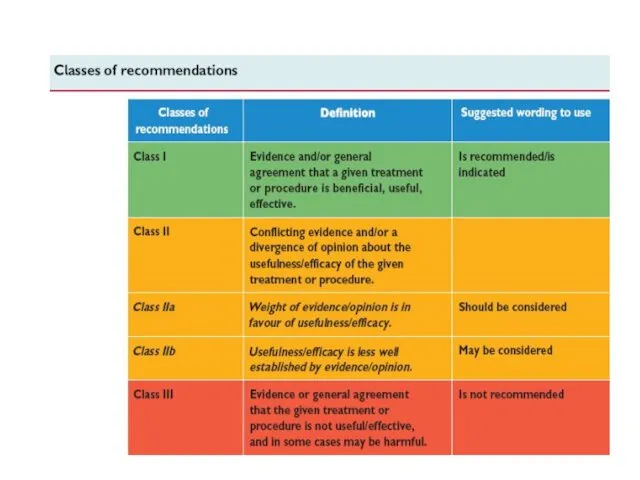
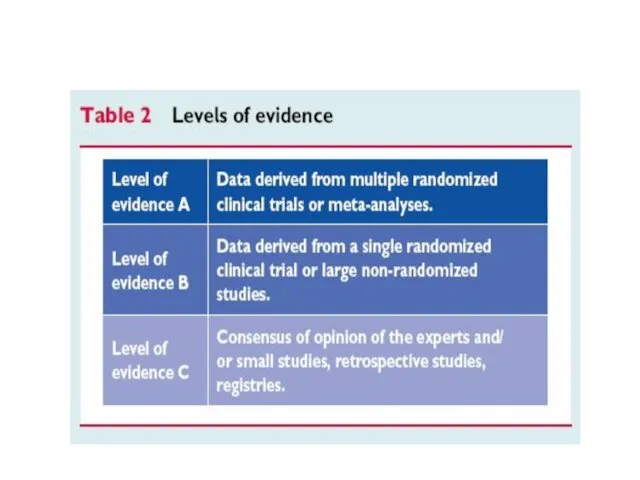
- 8. ESC guidelines 2004
- 12. Acute pericarditis
- 14. Acute pericarditis Most common form of pericardial disease ~5% of presentations to ED for non-ischemic chest
- 15. Acute pericarditis: etiology 80-95% of cases - idiopathic ( in Western Europe and in North America
- 16. Acute pericarditis: etiology (cont’d) Developed countries: emerging cases of pericarditis – iatrogenic posttraumatic, following cardiac surgery,
- 17. Acute pericarditis: etiology (cont’d) Developing countries: high prevalence of tuberculosis-related pericarditis (70-80%) in Sub-Saharian Africa, in
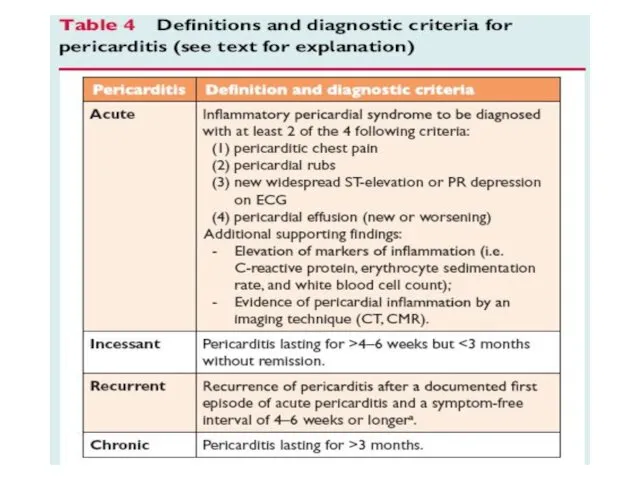
- 18. Acute pericarditis: diagnosis Typical chest pain (pleuritic CP) Pericarial friction rub Widespread ST-segment elevation and PR
- 19. Acute pericarditis: diagnosis Basic diagnostic evaluation Physical examination – auscultation ECG Trans-thoracic echocardiography (TTE) Chest x-ray
- 20. ECG in acute pericarditis
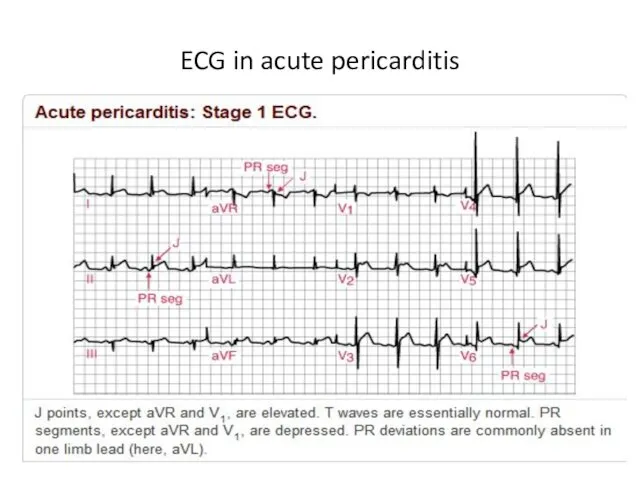
- 21. ECG in acute pericarditis
- 22. ECG in acute pericarditis
- 23. Acute pericarditis: diagnosis Basic diagnostic evaluation The need for routine etiology search in all cases of
- 24. Indications for pericardiocentesis Cardiac tamponade Large or symptomatic pericardial effusion despite medical therapy Highly suspected tuberculous,
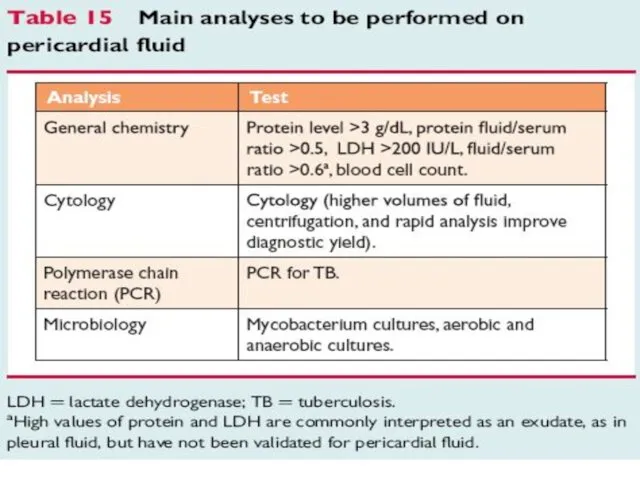
- 25. Acute pericarditis: diagnostic studies of pericardial fluid Protein LDH Glucose Cell count Less useful for diagnosis
- 26. Acute pericarditis: diagnostic studies of pericardial fluid Adenosin deaminase measurement for TB Tumor marker measurement (
- 27. Acute pericarditis: other diagnostic modalities Pericardial biopsy (during surgical drainage) - if cardiac tamponade relapsed after
- 28. Management of pericarditis
- 29. Acute pericarditis: risk stratification
- 30. Acute pericarditis: risk stratification At least one predictor of poor prognosis is sufficient to identify a
- 31. Acute pericarditis: therapy Targets toward specific etiology if known Empirical therapy for most cases (idiopathic or
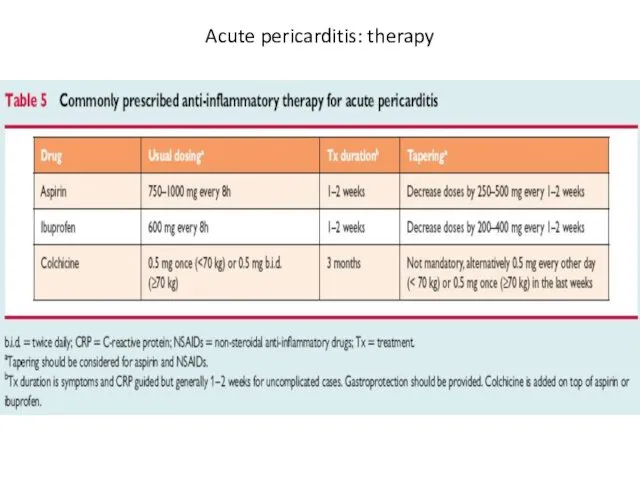
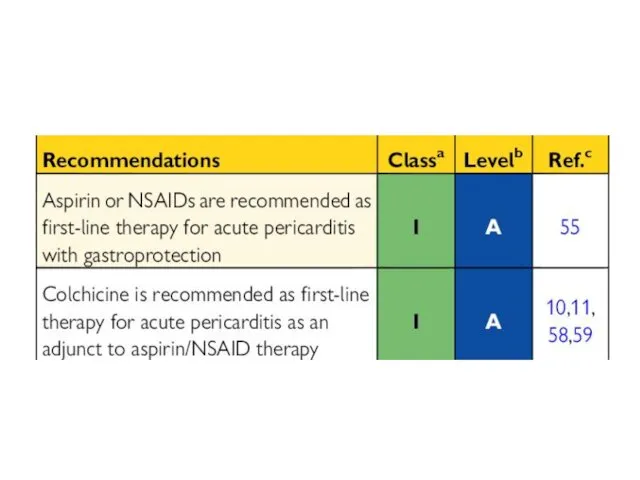
- 32. Acute pericarditis: therapy
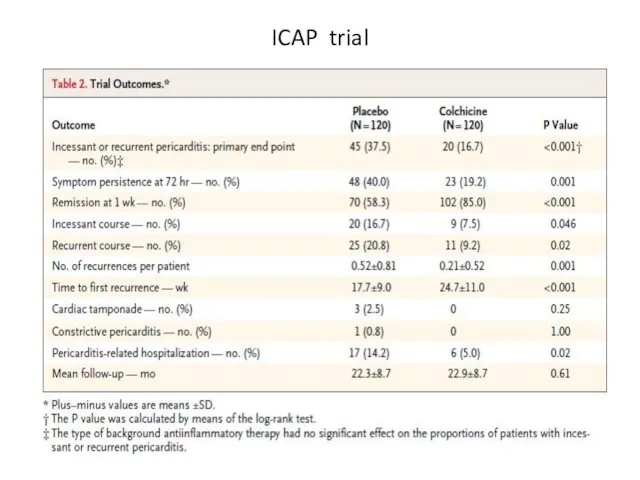
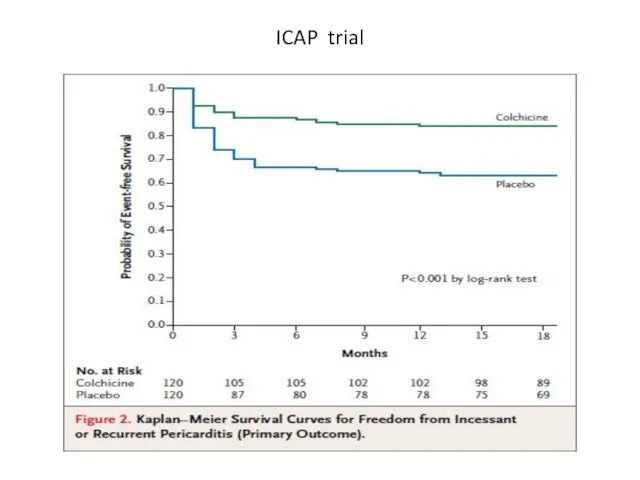
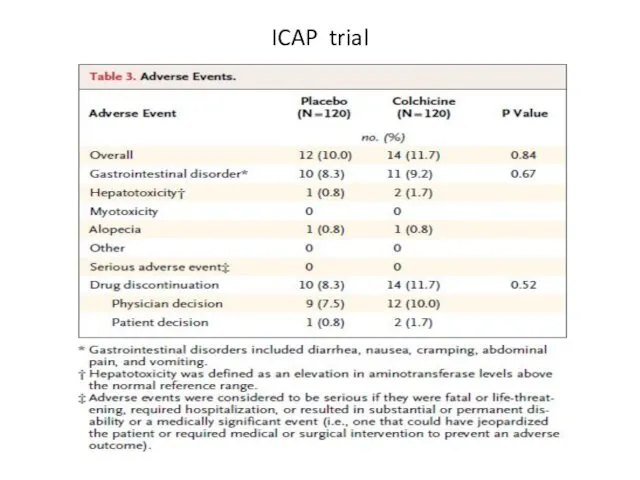
- 34. NEJM 2013, Sep 1
- 35. ICAP trial Colchicine 0.5 mg x 2/d for 3 months (for patients In addition to conventional
- 36. ICAP trial
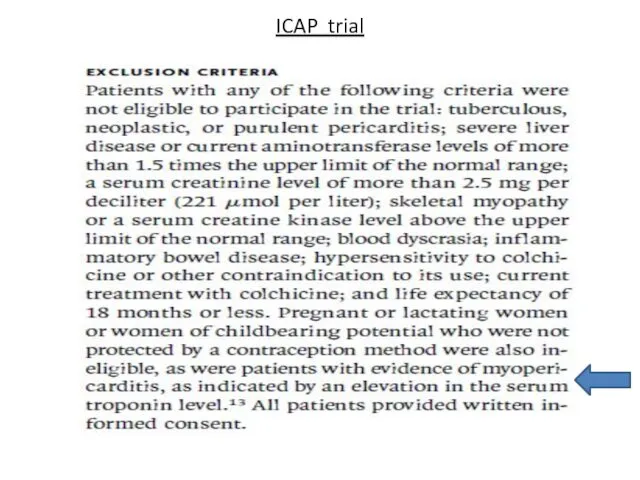
- 37. ICAP trial
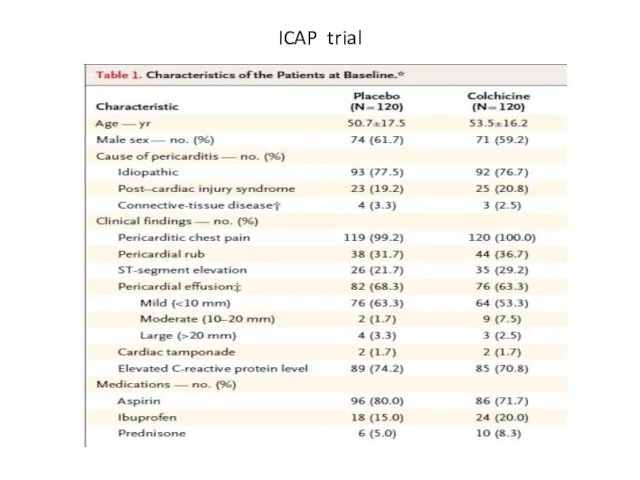
- 38. ICAP trial
- 39. ICAP trial
- 40. ICAP trial
- 42. Acute pericarditis: therapy Corticosteroids increase risk of pericaditis recurrence Indications: - contraindication for aspirin and NSAID
- 43. Acute pericarditis: therapy
- 44. Acute pericarditis: therapy
- 45. Acute pericarditis: therapy (cont’d) Rest and avoidance of physical activity are useful adjunctive measures until active
- 46. Acute pericarditis: therapy (cont’d) Athlets. Return to competitive sports only if: asymptomatic achieve normalization of ECG
- 47. Acute pericarditis: prognosis Recurrence is most common complication Incidence ~30% Autoimmune pathogenetic mechanism is most probable
- 48. Recurrent pericarditis
- 49. Recurrent pericarditis
- 50. Recurrent pericarditis: therapy
- 51. Pericardial effusion
- 52. Echo (4-chamber view) in pt with large pericardial effusion and cardiac tamponade PE PE
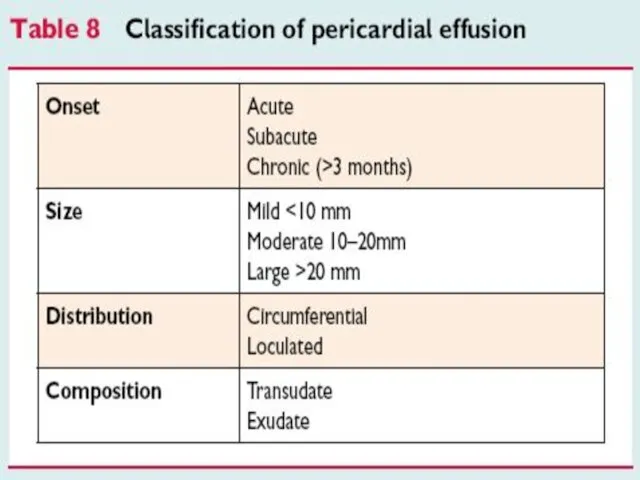
- 54. Pericardial effusion Large idiopatic chronic pericardial effusion defined as collection of pericardial fluid that persists for
- 55. Pericardial effusion Pericardiectomy is recommended in a case of large effusion after pericardiocentesis No medical therapy
- 56. Pericardial effusion: etiology Pericardial effusion without evidence of inflammation and pericarditis is often a clinical dilema
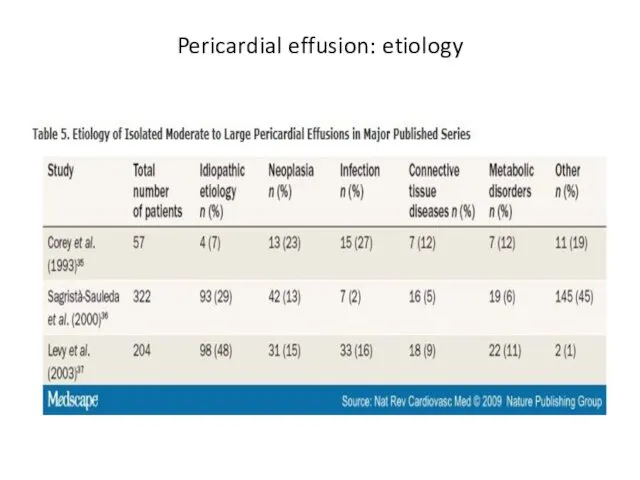
- 57. Pericardial effusion: etiology
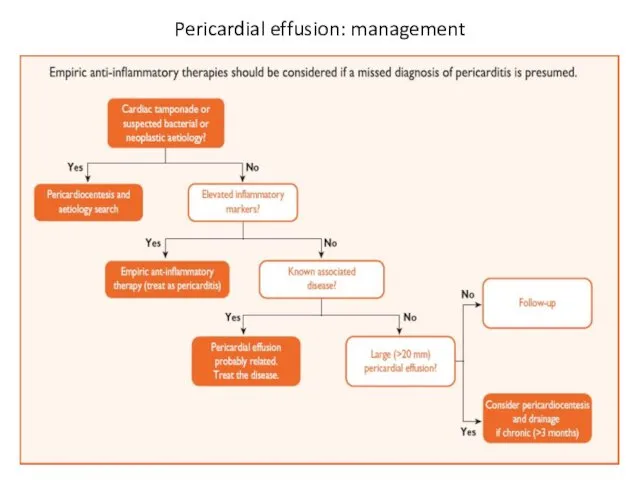
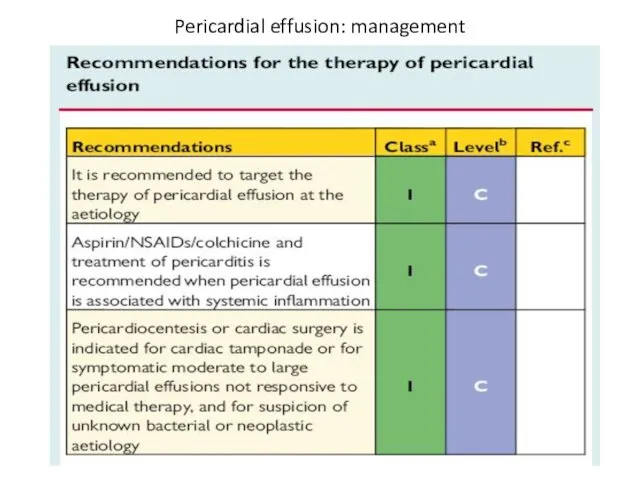
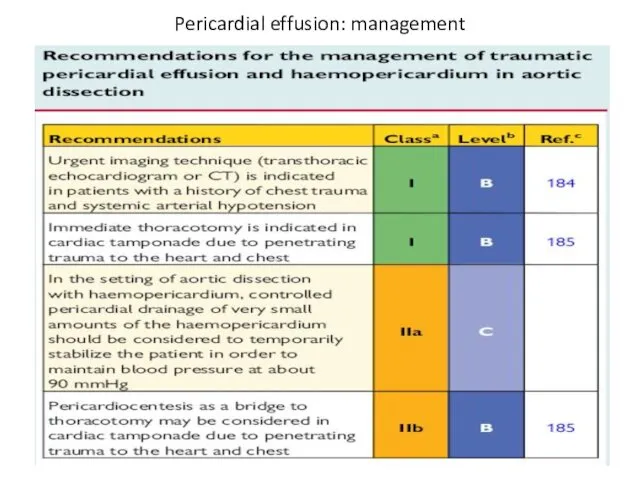
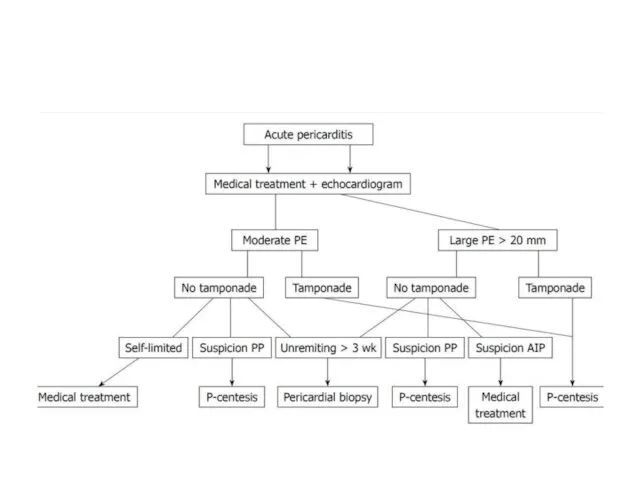
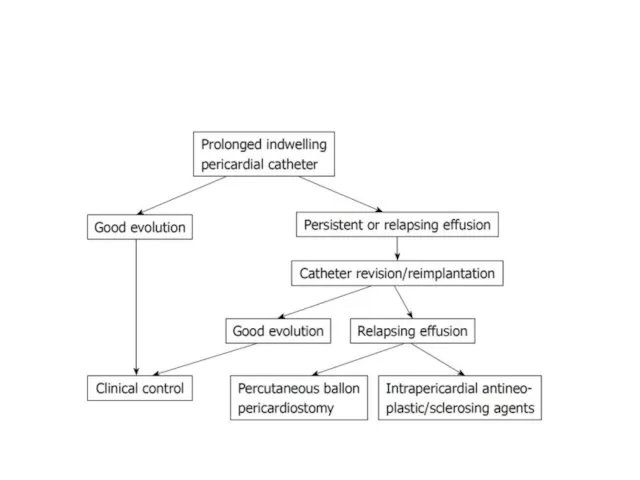
- 58. Pericardial effusion: management
- 59. Pericardial effusion: management
- 60. Pericardial effusion: management
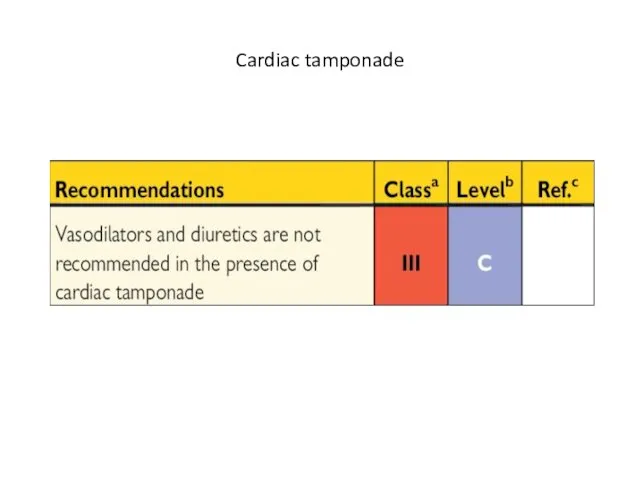
- 61. Cardiac tamponade
- 63. Cardiac tamponade Clinical signs Beck’s triad: hypotension, muffled heart sounds, elevated jugular venous pressure pulsus paradoxus
- 64. Cardiac tamponade Electrocardiographic signs - reduced voltage - electrical alternance Echocardiographic signs - large peicardial effusion
- 66. Cardiac tamponade
- 67. Approaches for pericardiocentesis parasternal apical subxyphoid / subcostal
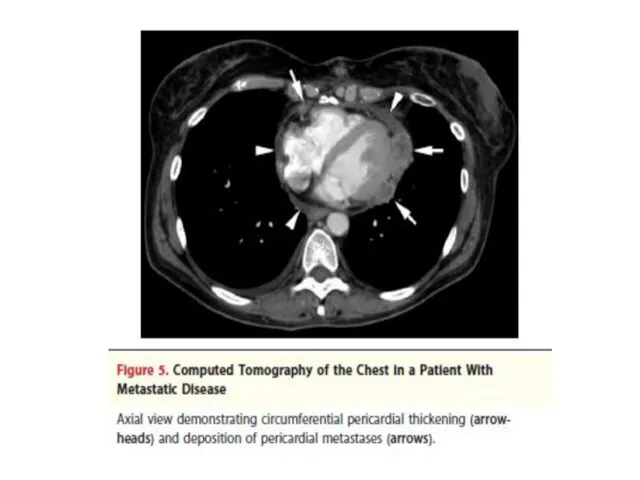
- 69. Recommendations for management of neoplastic involvement of the pericardium
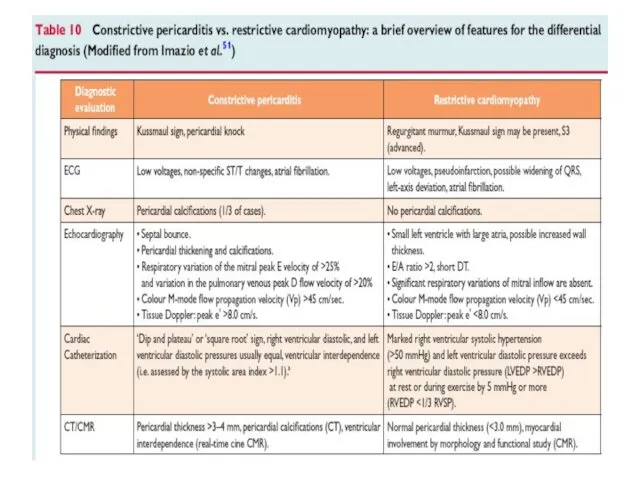
- 70. Constrictive pericarditis
- 71. Constrictive pericarditis
- 73. Constrictive pericarditis Fibrotic pericardium impedes normal diastolic filling because of loss of elasticity Usually pericardium is
- 74. Constrictive pericarditis: etiology Idiopathic or viral - 42-49% Cardiac surgery - 11-37% Radiation Rx - 9-31%
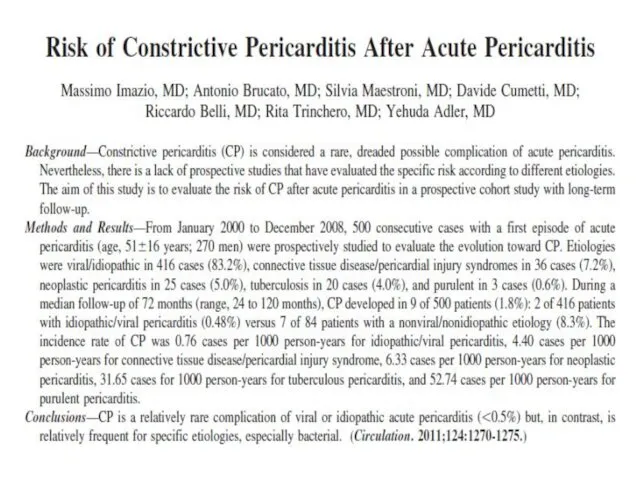
- 76. 500 patients Mean FU – 72 months Constrictive pericarditis – 1.8% Idiopathic/Viral (2 of 416 pts)
- 77. Circulation 2011; 124: 1270
- 78. Constrictive pericarditis: symptoms Right heart failure: range from periferal edema to anasarca No pulmonary congestion Usually
- 79. Constrictive pericarditis Pericardial constriction should be considered in any patient with unexplained elevation of jugular venous
- 81. Transient constrictive pericarditis 10-20% of cases during resolution of pericardial inflammation Patients with newly diagnosed constrictive
- 82. Effusive constrictive pericarditis In 8% of patients with cardiac tamponade who underwent pericardiocentesis and cardiac catheterization
- 83. Constrictive pericarditis: treatment
- 84. Thank you for attention
- 85. Backup slides
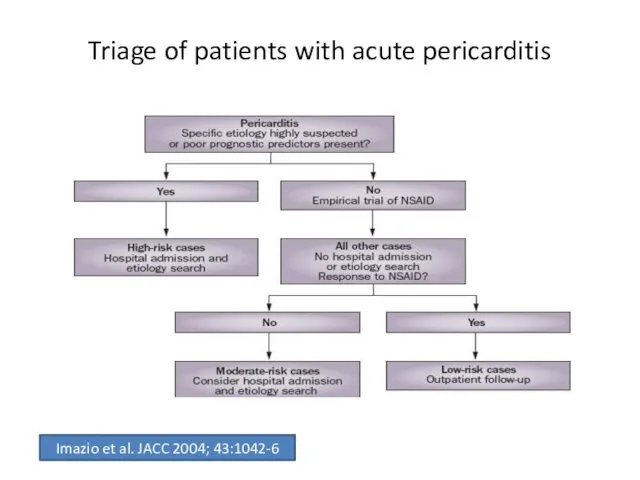
- 94. Triage of patients with acute pericarditis Imazio et al. JACC 2004; 43:1042-6
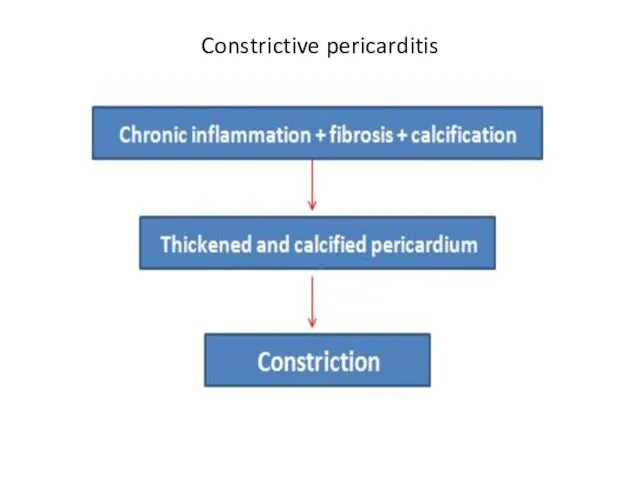
- 95. Causes of pericardial effusion Inflammation Infection Noninfectious etiology ------------------------------------------------------------------------- Chronic inflammation + fibrosis + calcification Thickened
- 96. Etiology of pericarditis Infectious pericarditis Pericarditis in systemic autoimmune diseases Type 2 (auto)immune process Pericarditis and
- 97. Acute pericarditis: therapy (cont’d)
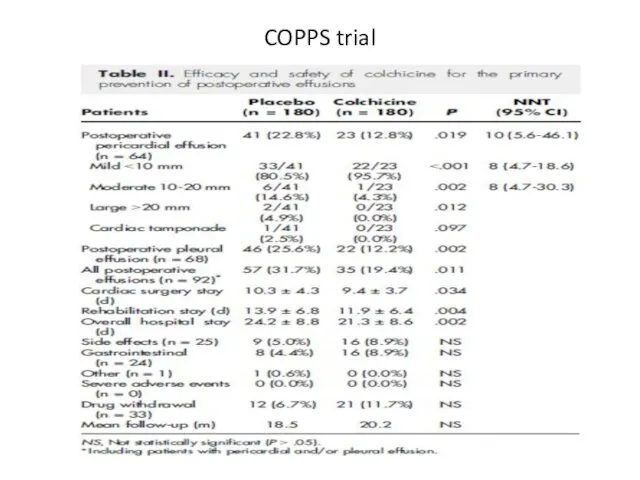
- 98. COPPS trial Am Heart J 2011; 62:527-32
- 99. COPPS trial
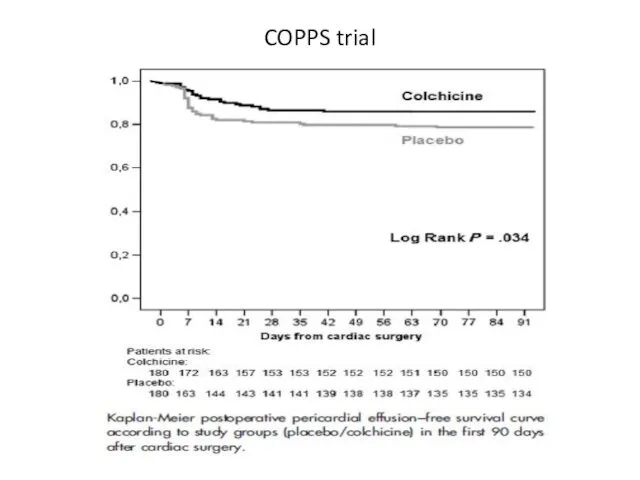
- 100. COPPS trial
- 101. COPPS trial
- 102. Rx of acute pericarditis in children
- 104. Скачать презентацию
Pericard : anatomical and physyological considerations
Outer layer - fibrous pericardium
Pericard : anatomical and physyological considerations
Outer layer - fibrous pericardium
Pericardial fluid
In normal hearts there is a small amount of pericardial
Pericardial fluid
In normal hearts there is a small amount of pericardial
Most common forms of pericardial syndromes
Acute and recurrent pericarditis
Pericardial effusion
Cardiac tamponade
Constrictive
Most common forms of pericardial syndromes
Acute and recurrent pericarditis
Pericardial effusion
Cardiac tamponade
Constrictive
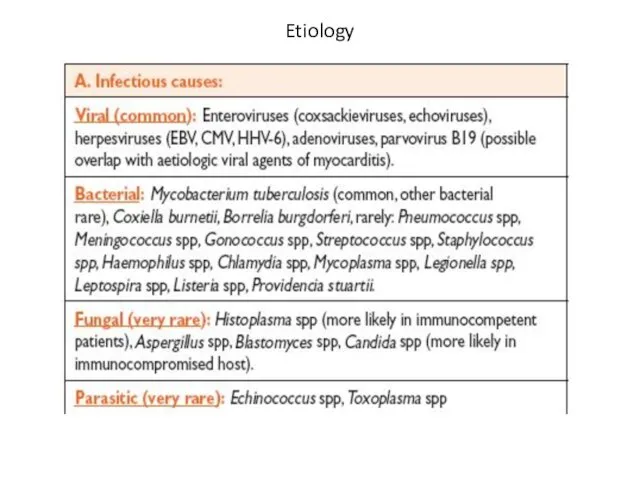
Etiology
Etiology
Etiology
Etiology
ESC guidelines 2004
ESC guidelines 2004
Acute pericarditis
Acute pericarditis
Most common form of pericardial disease
~5% of presentations to ED
Acute pericarditis
Most common form of pericardial disease
~5% of presentations to ED
Acute pericarditis: etiology
80-95% of cases - idiopathic ( in Western Europe
Acute pericarditis: etiology
80-95% of cases - idiopathic ( in Western Europe
Acute pericarditis: etiology (cont’d)
Developed countries:
emerging cases of pericarditis – iatrogenic
Acute pericarditis: etiology (cont’d)
Developed countries:
emerging cases of pericarditis – iatrogenic
Acute pericarditis: etiology (cont’d)
Developing countries:
high prevalence of tuberculosis-related pericarditis
(70-80%)
Acute pericarditis: etiology (cont’d)
Developing countries:
high prevalence of tuberculosis-related pericarditis
(70-80%)
Acute pericarditis: diagnosis
Typical chest pain (pleuritic CP)
Pericarial friction rub
Widespread ST-segment elevation
Acute pericarditis: diagnosis
Typical chest pain (pleuritic CP)
Pericarial friction rub
Widespread ST-segment elevation
Acute pericarditis: diagnosis
Basic diagnostic evaluation
Physical examination – auscultation
ECG
Trans-thoracic echocardiography (TTE)
Chest
Acute pericarditis: diagnosis
Basic diagnostic evaluation
Physical examination – auscultation
ECG
Trans-thoracic echocardiography (TTE)
Chest
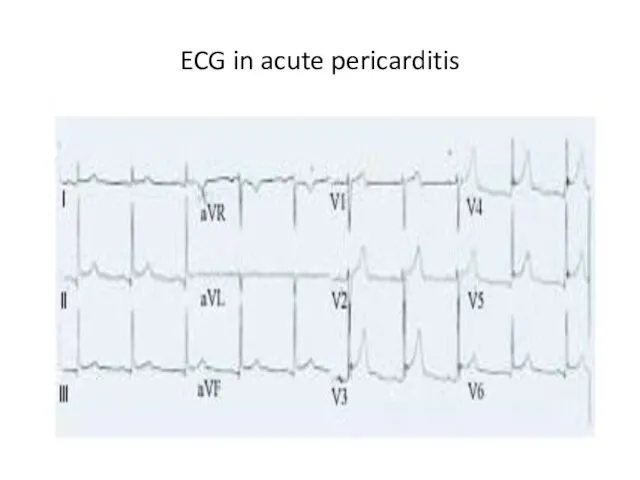
ECG in acute pericarditis
ECG in acute pericarditis
ECG in acute pericarditis
ECG in acute pericarditis
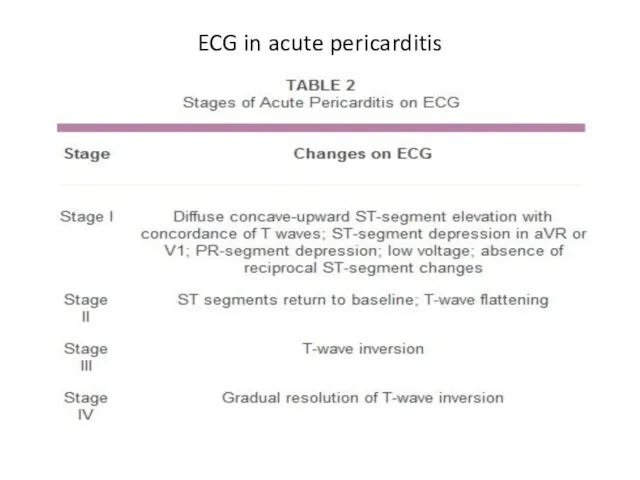
ECG in acute pericarditis
ECG in acute pericarditis
Acute pericarditis: diagnosis
Basic diagnostic evaluation
The need for routine etiology search in
Acute pericarditis: diagnosis
Basic diagnostic evaluation
The need for routine etiology search in
Indications for pericardiocentesis
Cardiac tamponade
Large or symptomatic pericardial effusion despite medical therapy
Highly
Indications for pericardiocentesis
Cardiac tamponade
Large or symptomatic pericardial effusion despite medical therapy
Highly
Acute pericarditis: diagnostic studies of pericardial fluid
Protein
LDH
Glucose
Cell count
Less useful for diagnosis
Acute pericarditis: diagnostic studies of pericardial fluid
Protein
LDH
Glucose
Cell count
Less useful for diagnosis
Acute pericarditis: diagnostic studies of pericardial fluid
Adenosin deaminase measurement for TB
Tumor
Acute pericarditis: diagnostic studies of pericardial fluid
Adenosin deaminase measurement for TB
Tumor
Acute pericarditis: other diagnostic
modalities
Pericardial biopsy (during surgical drainage)
- if cardiac
Acute pericarditis: other diagnostic
modalities
Pericardial biopsy (during surgical drainage)
- if cardiac
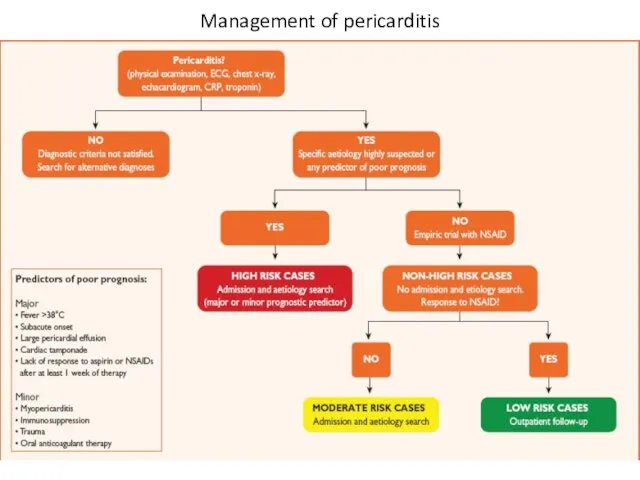
Management of pericarditis
Management of pericarditis
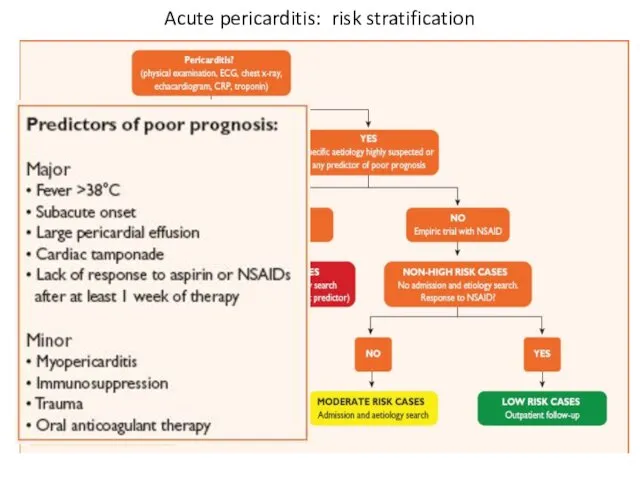
Acute pericarditis: risk stratification
Acute pericarditis: risk stratification
Acute pericarditis: risk stratification
At least one predictor of poor prognosis is
Acute pericarditis: risk stratification
At least one predictor of poor prognosis is
Acute pericarditis: therapy
Targets toward specific etiology if known
Empirical therapy for most
Acute pericarditis: therapy
Targets toward specific etiology if known
Empirical therapy for most
Acute pericarditis: therapy
Acute pericarditis: therapy
NEJM 2013, Sep 1
NEJM 2013, Sep 1
ICAP trial
Colchicine 0.5 mg x 2/d for 3 months
ICAP trial
Colchicine 0.5 mg x 2/d for 3 months
ICAP trial
ICAP trial
ICAP trial
ICAP trial
ICAP trial
ICAP trial
ICAP trial
ICAP trial
ICAP trial
ICAP trial
Acute pericarditis: therapy
Corticosteroids increase risk of pericaditis recurrence
Indications:
- contraindication for
Acute pericarditis: therapy
Corticosteroids increase risk of pericaditis recurrence
Indications:
- contraindication for
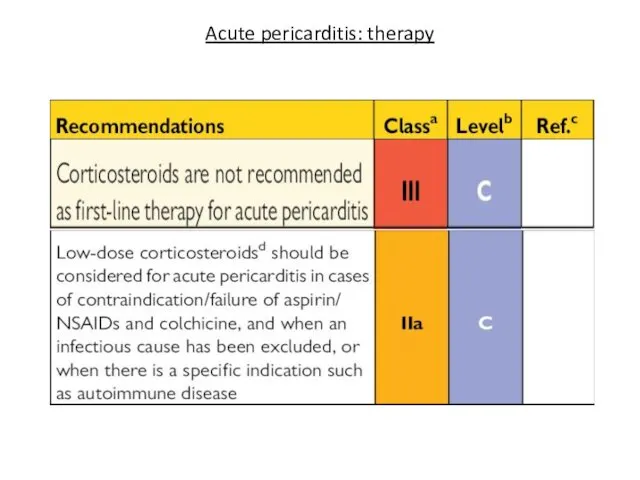
Acute pericarditis: therapy
Acute pericarditis: therapy
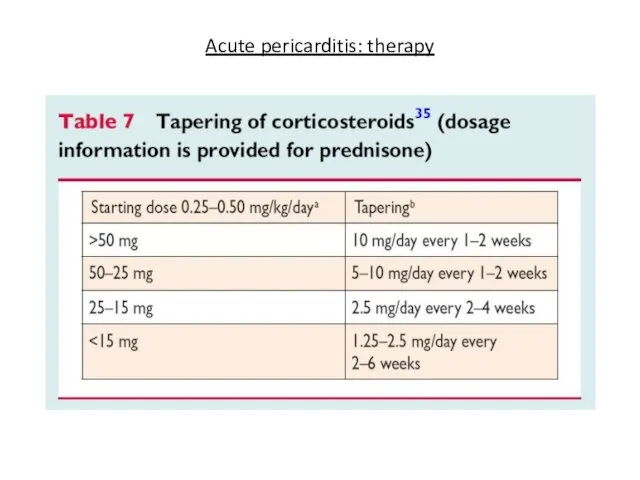
Acute pericarditis: therapy
Acute pericarditis: therapy
Acute pericarditis: therapy (cont’d)
Rest and avoidance of physical activity are useful
Acute pericarditis: therapy (cont’d)
Rest and avoidance of physical activity are useful
Acute pericarditis: therapy (cont’d)
Athlets. Return to competitive sports only if:
asymptomatic
achieve
Acute pericarditis: therapy (cont’d)
Athlets. Return to competitive sports only if:
asymptomatic
achieve
Acute pericarditis: prognosis
Recurrence is most common complication
Incidence ~30%
Autoimmune pathogenetic mechanism is
Acute pericarditis: prognosis
Recurrence is most common complication
Incidence ~30%
Autoimmune pathogenetic mechanism is
Recurrent pericarditis
Recurrent pericarditis
Recurrent pericarditis
Recurrent pericarditis
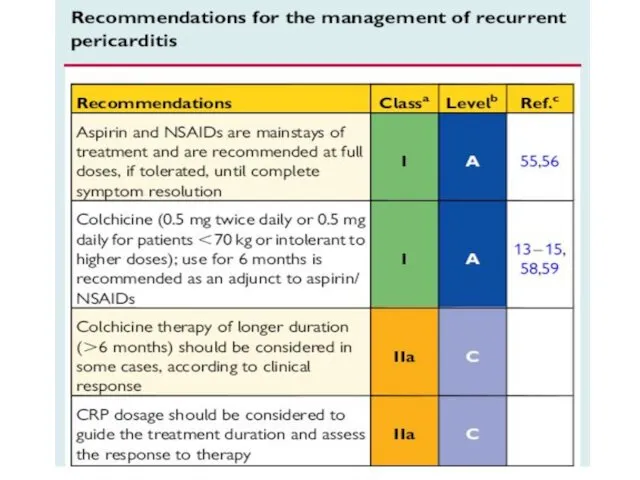
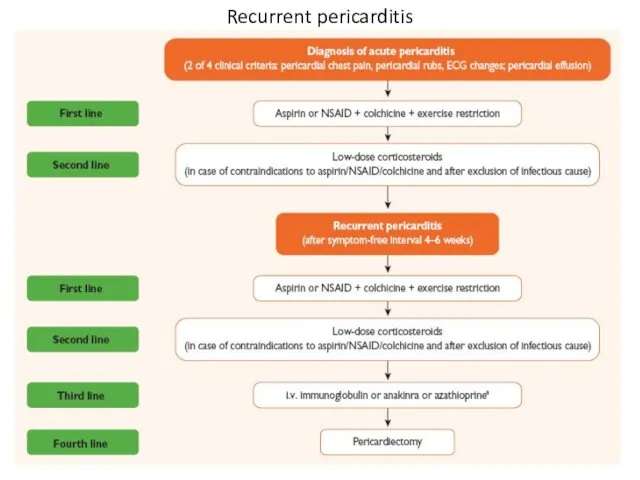
Recurrent pericarditis: therapy
Recurrent pericarditis: therapy
Pericardial effusion
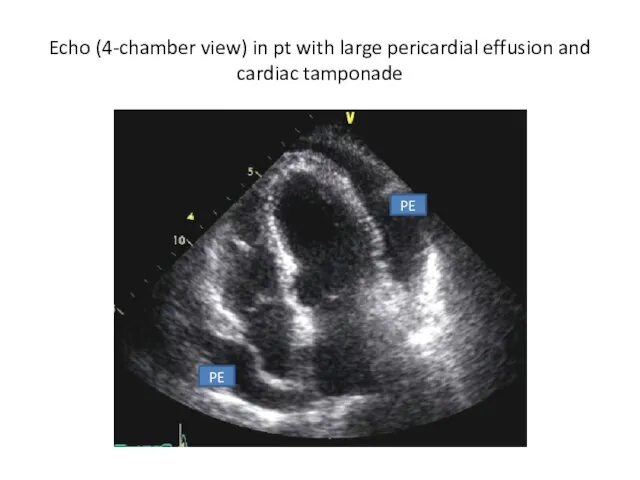
Echo (4-chamber view) in pt with large pericardial effusion and cardiac
Echo (4-chamber view) in pt with large pericardial effusion and cardiac
Pericardial effusion
Large idiopatic chronic pericardial effusion defined as collection of pericardial
Pericardial effusion
Large idiopatic chronic pericardial effusion defined as collection of pericardial
Pericardial effusion
Pericardiectomy is recommended in a case of large effusion after
Pericardial effusion
Pericardiectomy is recommended in a case of large effusion after
Pericardial effusion: etiology
Pericardial effusion without evidence of inflammation and pericarditis is
Pericardial effusion: etiology
Pericardial effusion without evidence of inflammation and pericarditis is
Pericardial effusion: etiology
Pericardial effusion: etiology
Pericardial effusion: management
Pericardial effusion: management
Pericardial effusion: management
Pericardial effusion: management
Pericardial effusion: management
Pericardial effusion: management
Cardiac tamponade
Cardiac tamponade
Clinical signs
Beck’s triad: hypotension, muffled heart sounds,
elevated jugular venous
Cardiac tamponade
Clinical signs
Beck’s triad: hypotension, muffled heart sounds,
elevated jugular venous
Cardiac tamponade
Electrocardiographic signs
- reduced voltage
- electrical alternance
Echocardiographic signs
-
Cardiac tamponade
Electrocardiographic signs
- reduced voltage
- electrical alternance
Echocardiographic signs
-
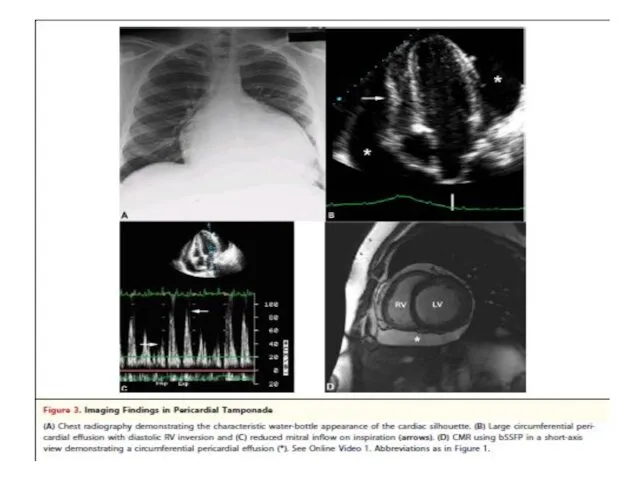
Cardiac tamponade
Cardiac tamponade
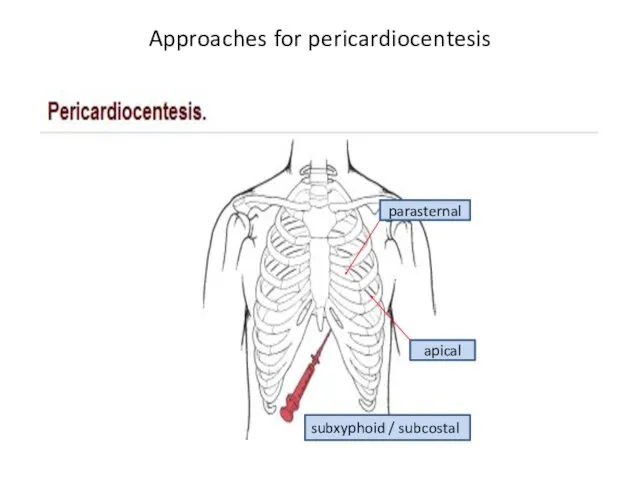
Approaches for pericardiocentesis
parasternal
apical
subxyphoid / subcostal
Approaches for pericardiocentesis
parasternal
apical
subxyphoid / subcostal
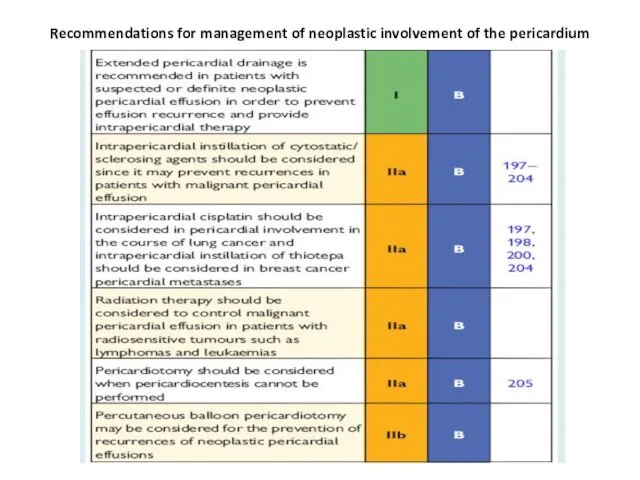
Recommendations for management of neoplastic involvement of the pericardium
Recommendations for management of neoplastic involvement of the pericardium
Constrictive pericarditis
Constrictive pericarditis
Constrictive pericarditis

Constrictive pericarditis
Fibrotic pericardium impedes normal diastolic filling because of loss of
Constrictive pericarditis
Fibrotic pericardium impedes normal diastolic filling because of loss of
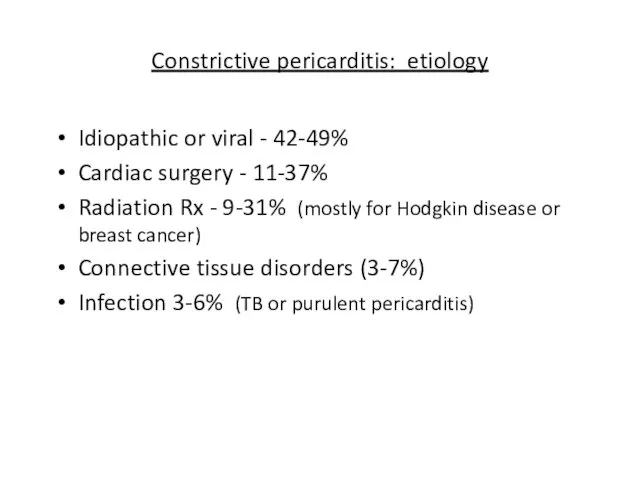
Constrictive pericarditis: etiology
Idiopathic or viral - 42-49%
Cardiac surgery - 11-37%
Radiation Rx
Constrictive pericarditis: etiology
Idiopathic or viral - 42-49%
Cardiac surgery - 11-37%
Radiation Rx
500 patients
Mean FU – 72 months
Constrictive pericarditis – 1.8%
Idiopathic/Viral (2 of
500 patients
Mean FU – 72 months
Constrictive pericarditis – 1.8%
Idiopathic/Viral (2 of
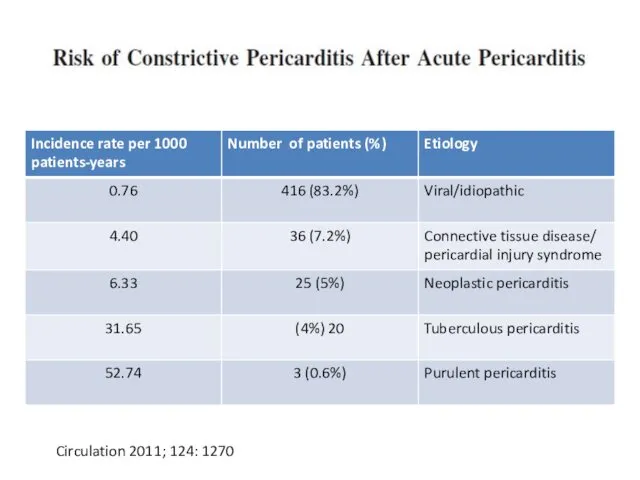
Circulation 2011; 124: 1270
Circulation 2011; 124: 1270
Constrictive pericarditis: symptoms
Right heart failure: range from periferal edema to anasarca
Constrictive pericarditis: symptoms
Right heart failure: range from periferal edema to anasarca
Constrictive pericarditis
Pericardial constriction should be considered in any patient with
Constrictive pericarditis
Pericardial constriction should be considered in any patient with
Transient constrictive pericarditis
10-20% of cases during resolution of pericardial inflammation
Patients with
Transient constrictive pericarditis
10-20% of cases during resolution of pericardial inflammation
Patients with
Effusive constrictive pericarditis
In 8% of patients with cardiac tamponade who underwent
Effusive constrictive pericarditis
In 8% of patients with cardiac tamponade who underwent
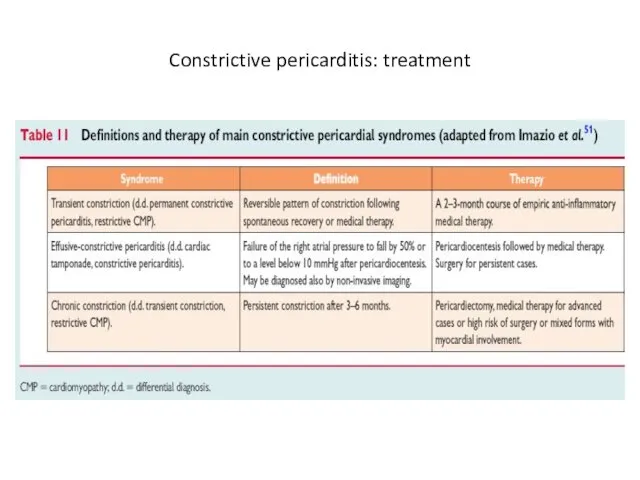
Constrictive pericarditis: treatment
Constrictive pericarditis: treatment
Thank you for attention
Backup slides

Triage of patients with acute pericarditis
Imazio et al. JACC 2004; 43:1042-6
Triage of patients with acute pericarditis
Imazio et al. JACC 2004; 43:1042-6
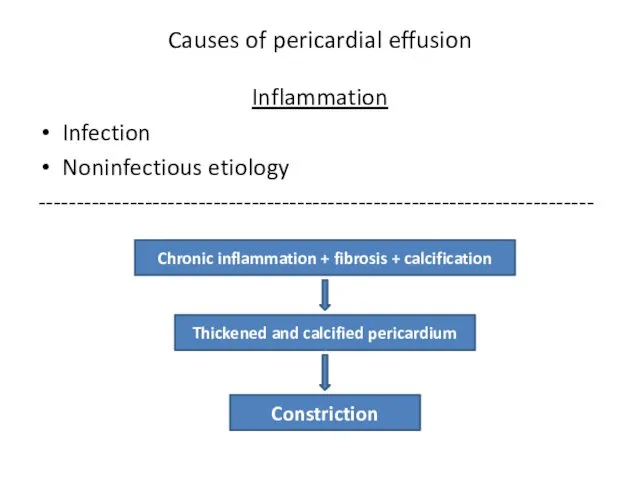
Causes of pericardial effusion
Inflammation
Infection
Noninfectious etiology
-------------------------------------------------------------------------
Chronic inflammation + fibrosis + calcification
Thickened and
Causes of pericardial effusion
Inflammation
Infection
Noninfectious etiology
-------------------------------------------------------------------------
Chronic inflammation + fibrosis + calcification
Thickened and
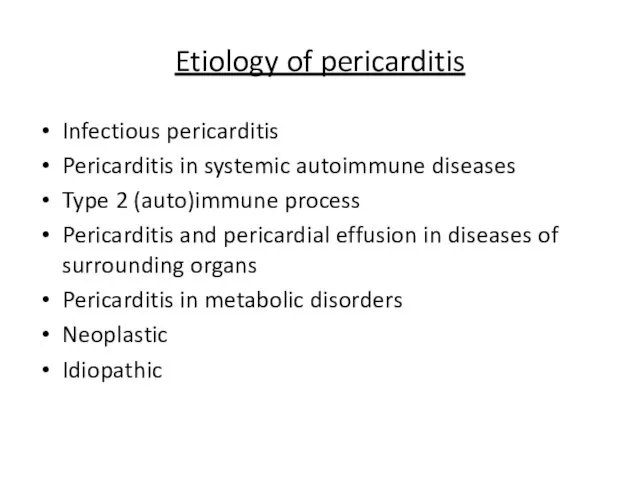
Etiology of pericarditis
Infectious pericarditis
Pericarditis in systemic autoimmune diseases
Type 2 (auto)immune process
Pericarditis
Etiology of pericarditis
Infectious pericarditis
Pericarditis in systemic autoimmune diseases
Type 2 (auto)immune process
Pericarditis
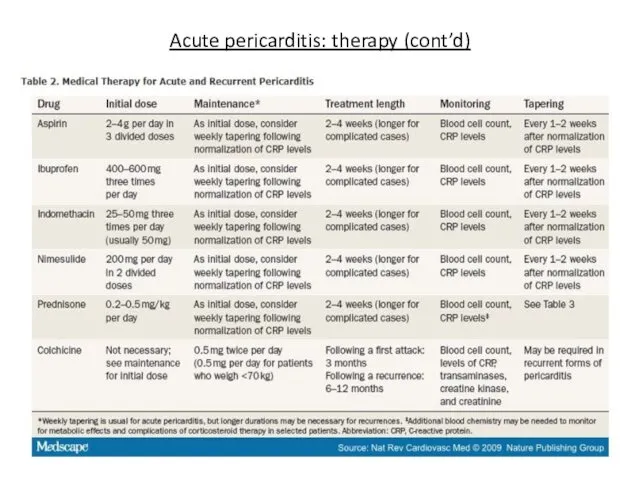
Acute pericarditis: therapy (cont’d)
Acute pericarditis: therapy (cont’d)
COPPS trial
Am Heart J 2011; 62:527-32
COPPS trial
Am Heart J 2011; 62:527-32
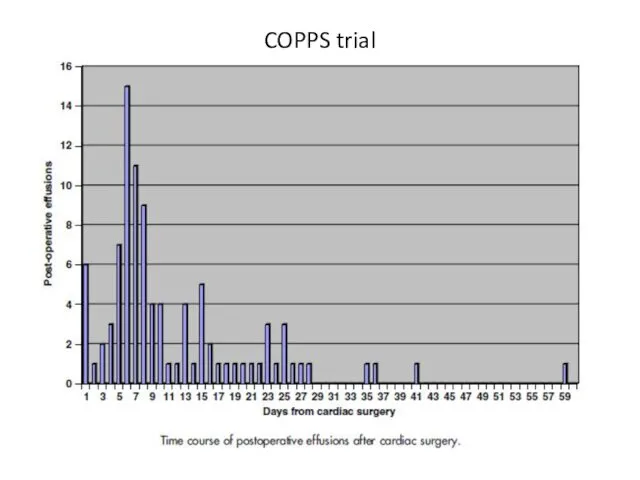
COPPS trial
COPPS trial
COPPS trial
COPPS trial
COPPS trial
COPPS trial
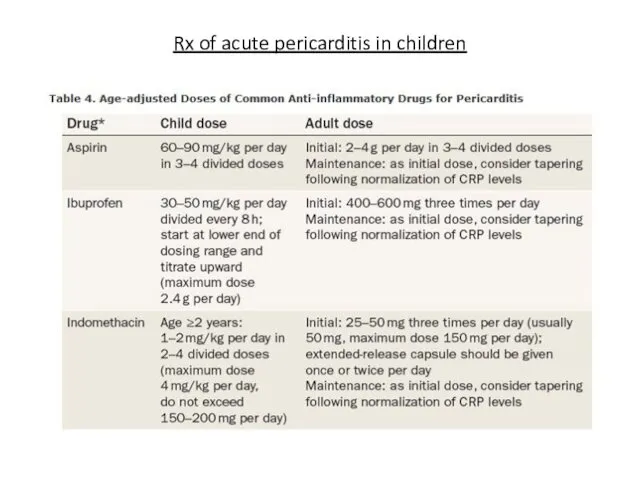
Rx of acute pericarditis in children
Rx of acute pericarditis in children
 Необратимое повреждение – некроз
Необратимое повреждение – некроз Кадровая политика в здравоохранении. Критерии оценки и совершенствование
Кадровая политика в здравоохранении. Критерии оценки и совершенствование Жедел аппендицит
Жедел аппендицит узи
узи Понятие об иммунитете. Строение иммунной системы. Антигены
Понятие об иммунитете. Строение иммунной системы. Антигены Наркотики. Їх види та вплив
Наркотики. Їх види та вплив Жедел ішек инфекциялары
Жедел ішек инфекциялары Гормональные лекарственные средства
Гормональные лекарственные средства Анатомия и физиология полости рта. Анатомия зубов. Гистология твердых тканей зуба. Рентгенанатомия зубов
Анатомия и физиология полости рта. Анатомия зубов. Гистология твердых тканей зуба. Рентгенанатомия зубов Цирроз печени
Цирроз печени Морфологические группы лекарственного растительного сырья и их особенности
Морфологические группы лекарственного растительного сырья и их особенности Кеуде қуысының жарақаты. Қабырға, омыртқа сынуы
Кеуде қуысының жарақаты. Қабырға, омыртқа сынуы ОРВИ и грипп
ОРВИ и грипп Диета №9: лечебное питание при сахарном диабете
Диета №9: лечебное питание при сахарном диабете Противосудорожные препараты
Противосудорожные препараты Опухоль. Доброкачественные и злокачественные опухоли
Опухоль. Доброкачественные и злокачественные опухоли Принципы Рационального Питания
Принципы Рационального Питания Ауыл тұрғындарына алғашқы медико – санитарлық көмекті ұйымдастыру
Ауыл тұрғындарына алғашқы медико – санитарлық көмекті ұйымдастыру Bronchial asthma in children (treatment)
Bronchial asthma in children (treatment) Субмукозная миома матки
Субмукозная миома матки Болезни гипофиза: МСЭ и реабилитация
Болезни гипофиза: МСЭ и реабилитация Системная красная волчанка
Системная красная волчанка Клиническая психология
Клиническая психология Улану кезіндегі шұғыл көмек
Улану кезіндегі шұғыл көмек Миокардиты у детей
Миокардиты у детей Патогенез гнойно-воспалительных заболеваний
Патогенез гнойно-воспалительных заболеваний Создание единого цифрового контура в здравоохранении
Создание единого цифрового контура в здравоохранении Первая медицинская помощь при массовых поражениях
Первая медицинская помощь при массовых поражениях