- Tuberculosis of the kidney and ureter

Содержание
- 2. Plans: Introduction: What is the tuberculosis of the kidney and ureter? Main part: Etiology Pathogenesis Pathology
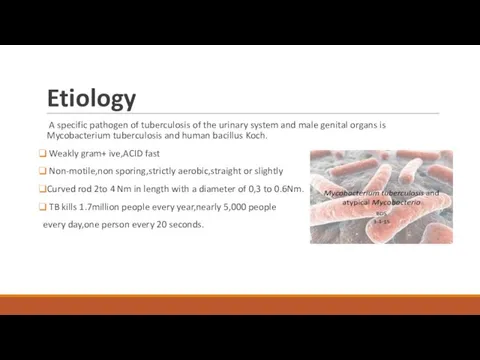
- 3. Etiology A specific pathogen of tuberculosis of the urinary system and male genital organs is Mycobacterium
- 4. Pathogenesis Primary pulmonary infection Imflammotory reaction Little resistance/ Multiplication Spread Limphatic then blood Immune response within
- 5. Pathogenesis: The small silent renal granulomas resulting from ilent hematogenous dissemination are typically founf bilaterally in
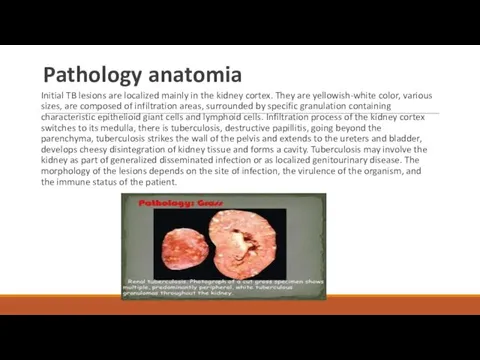
- 6. Pathology anatomia Initial TB lesions are localized mainly in the kidney cortex. They are yellowish-white color,
- 7. CLASSIFICATION: We distinguish following clinical forms nephrotuberculosis: I STAGE- NONdestructive. Tuberculosis of renal parenchyma.(minimal,primary form) II
- 8. Symptoms: The clinical picture of the disease depends on the amount of destruction and process steps.
- 9. Approximately 75% of patients present with symptoms suggesting urinary tract inflammation. DYSURIA MILD OR MODERATELY SEVERE
- 10. DIAGNOSIS:
- 11. Laboratory analyses A microbiologic diagnosis of tuberculosis usually is made by isolation of the causative organism
- 12. Differential diagnosis: Chronic nonspecific pyelonephrititis Necrotizing granulomas:1)Wegener’s granulomatosis; 2)fungal infections. Non-caseating granulomas:1)sarcoidosis; 2)leprosy; 3)brucellosis Foreign body
- 13. TREATMENT: Modern short-course antituberculosis drug regimens are effective in all forms of tuberculosis. They are based
- 14. Prognosis In tuberculosis of the kidneys and urinary tract prognosis depends on the stage of the
- 16. Скачать презентацию

Plans:
Introduction:
What is the tuberculosis of the kidney and
Plans:
Introduction:
What is the tuberculosis of the kidney and
Etiology
A specific pathogen of tuberculosis of the urinary system and
Etiology
A specific pathogen of tuberculosis of the urinary system and
Pathogenesis
Primary pulmonary infection
Imflammotory reaction
Little resistance/ Multiplication
Spread Limphatic then
Pathogenesis
Primary pulmonary infection
Imflammotory reaction
Little resistance/ Multiplication
Spread Limphatic then
Pathogenesis:
The small silent renal granulomas resulting from ilent hematogenous
Pathogenesis:
The small silent renal granulomas resulting from ilent hematogenous
Pathology anatomia
Initial TB lesions are localized mainly in the kidney cortex.
Pathology anatomia
Initial TB lesions are localized mainly in the kidney cortex.

CLASSIFICATION:
We distinguish following clinical forms nephrotuberculosis:
I STAGE- NONdestructive.
CLASSIFICATION:
We distinguish following clinical forms nephrotuberculosis:
I STAGE- NONdestructive.
Symptoms:
The clinical picture of the disease depends on the amount of
Symptoms:
The clinical picture of the disease depends on the amount of
Approximately 75% of patients present with symptoms suggesting urinary tract inflammation.
Approximately 75% of patients present with symptoms suggesting urinary tract inflammation.

DIAGNOSIS:
DIAGNOSIS:

Laboratory analyses
A microbiologic diagnosis of tuberculosis usually is made by isolation
Laboratory analyses
A microbiologic diagnosis of tuberculosis usually is made by isolation

Differential diagnosis:
Chronic nonspecific pyelonephrititis
Necrotizing granulomas:1)Wegener’s granulomatosis; 2)fungal infections.
Non-caseating granulomas:1)sarcoidosis;
Differential diagnosis:
Chronic nonspecific pyelonephrititis
Necrotizing granulomas:1)Wegener’s granulomatosis; 2)fungal infections.
Non-caseating granulomas:1)sarcoidosis;
TREATMENT:
Modern short-course antituberculosis drug regimens are effective in all forms of
TREATMENT:
Modern short-course antituberculosis drug regimens are effective in all forms of

Prognosis
In tuberculosis of the kidneys and urinary tract prognosis depends on
Prognosis
In tuberculosis of the kidneys and urinary tract prognosis depends on
 Бронхиальная астма у детей
Бронхиальная астма у детей Противовоспалительные лекарственные средства (ПВЛС)
Противовоспалительные лекарственные средства (ПВЛС) Мүгедектік
Мүгедектік Түбір өзектерді көлікті өңдеу әдістері
Түбір өзектерді көлікті өңдеу әдістері Малярия, токсоплазма, лямблии
Малярия, токсоплазма, лямблии Сүйек сыну. Буын шығу соғып алу. Сіңір созылу
Сүйек сыну. Буын шығу соғып алу. Сіңір созылу Бронхиальная астма
Бронхиальная астма Сифилитический увеит
Сифилитический увеит Қыз баланың, бойжеткеннің және әйелдің жеке бас гигиенасы
Қыз баланың, бойжеткеннің және әйелдің жеке бас гигиенасы Тамыр ішіндегі шашыранды қан ұю (ТШҚҰ) синдромы
Тамыр ішіндегі шашыранды қан ұю (ТШҚҰ) синдромы Кожно – кинестетический анализатор. Сенсорные кожно-кинестетические расстройства. Исследование тактильного гнозиса
Кожно – кинестетический анализатор. Сенсорные кожно-кинестетические расстройства. Исследование тактильного гнозиса Помощь при отравлениях
Помощь при отравлениях Группы крови. Гемостаз
Группы крови. Гемостаз Эпидемиологическая характеристика инфекционных заболеваний с аэрозольным механизмом передачи инфекции
Эпидемиологическая характеристика инфекционных заболеваний с аэрозольным механизмом передачи инфекции Ожоги лица. Клиника, диагностика, лечение
Ожоги лица. Клиника, диагностика, лечение Визначення туберкульозу як наукової і практичної проблеми. Історія фтизіатрії. Епідеміологія туберкульозу
Визначення туберкульозу як наукової і практичної проблеми. Історія фтизіатрії. Епідеміологія туберкульозу Glomerulonefrit, endokardit, kolit
Glomerulonefrit, endokardit, kolit Болезнь Вильсона-Коновалова. Дифференциальный диагноз с хроническими гепатитами
Болезнь Вильсона-Коновалова. Дифференциальный диагноз с хроническими гепатитами Сердце в традиционной китайской медицине
Сердце в традиционной китайской медицине Эндовидеохирургия. Выполняемые операции
Эндовидеохирургия. Выполняемые операции СРС на тему: Холодовая цепь
СРС на тему: Холодовая цепь Терминальные состояние: стадии, клиника, диагностика, критерии оценки тяжести состояния больного
Терминальные состояние: стадии, клиника, диагностика, критерии оценки тяжести состояния больного Бронхоэктатическая болезнь
Бронхоэктатическая болезнь Мышцы верхней конечности
Мышцы верхней конечности Общие тенденции развития медицинской реабилитации в Краснодарском крае
Общие тенденции развития медицинской реабилитации в Краснодарском крае Лікарські рослини, їх значення. Ароматерапія
Лікарські рослини, їх значення. Ароматерапія Предменструальный, климактерический синдром, посткастрационный синдром
Предменструальный, климактерический синдром, посткастрационный синдром Харчові отруєння
Харчові отруєння