- Vaginal discharge + pruritis

Содержание
- 2. Vaginal Discharge Vaginal discharge may be blood stained white cream, yellow, or greenish discharge and wrongly
- 3. PHYSIOLOGY OF THE VAGINA The vagina is lined by non-keratinized stratified squamous epithelial influenced by estrogen
- 4. Lactobacilli (Duoderline Bacilli) Convert glycogen to lactic acid pH of the vagina is 3.5-4.5
- 5. Vaginal Ecosystem Dynamic equilibrium between microflora and metabollic by products of the microflora, host estrogen and
- 6. Factors affecting the vaginal Ecosystem Antibiotics Hormones or lack of hormones Contraceptive preparations Douches Vaginal Medication
- 7. Vaginal Desquamated Tissue Reproductive age – superfacial cells (est) Luteal phase- Intermediate cells (prog) Postmenopausal women-
- 8. Differential Diagnosis Pediatrics + Peripubertal Physiological leukorrhea – high estrogen Eczema Psoriasis Pinworm- rectum itchy Foreign
- 9. Investigation: Swab for culture PR Examination EUA X-RAY pelvic Exclude sexual abuse Management: Hygiene Antibiotics Steroids
- 10. Post Menopausal Exclude malignancy
- 11. 3. Reproductive Age: 1. Physiological : Increased in pregnancy and mid cycle. Consists of cervical mucous
- 12. 2. Infection: Trichomonas vaginalis Candida vaginitis Bacterial vaginosis( non specific vaginitis) Sexual transmitted disease Neisseria gonorrhea,
- 13. 3. Urinary and faeculent discharge – vvv 4. Foreign body: IUCD, neglected pessay, vaginal diaphragm 5.
- 14. DIAGNOSIS History: Age Type of discharge Amount Onset (relation to antibiotics medication relation to menstruation) Use
- 15. 2. General Examination:(Anemia, Cachaxia) Inspection of vulva Speculum examination Amount, consistency, characteristic, odor Bimanual examination
- 16. Investigation 3 Specimens a. Wet mount smear (ad saline) b. Swab for culture and sensitivity c.
- 17. Treatment: According to the Cause Foreign body – remove Leukorrhoea a. Reassurance b. Hygience c. Minimize
- 18. Vaginal Infection Trichomonas vaginitis: STD: 70% of males contract the disease after single exposure Symptoms: 25%
- 19. Signs: Thin Frothy Pale Green or gray discharge pH 5-6.5 The organism ferment carbohydrates – Produce
- 20. Investigation Identify the organism in wet mount smear The organism is pear-shaped and motile with a
- 21. Management Oral Metronidazole (flagyl) Single dose 2 gm 500 mg P.O twice for 1 week :
- 22. Causes of Treatment Failure: Compliance Partner as a reservoir Treatment: Vaginal Route Note: Treatment during pregnancy
- 23. Candida Vaginitis: Moniliasis Causative organisms: Candida albicans Is not STD CAUSES: Hormonal factor ( O.C.P) Depress
- 24. Symptoms: 20% asymptomatic Pruritus Vulvar burning External dysuria Dyspareunia Vaginal discharge ( white, highly viscous, granular,
- 25. Signs Erythema Oedema Excoriation Pustules Speculum: cottage cheese type of discharge Adherent thrush patches attached to
- 26. Investigation 1.Clinical 2. pH of the vagina norma 3. Fungal element either budding yeast form or
- 27. Management Standard Topically applied azole ( nystatin) - 80% - 90% relief 3. Oral antifungal (Fluconazole)
- 28. RECURRENT DISEASE Definition: More than 3 episodes of infection in one year. Causes: Poor compliance Exclude
- 29. Treatment Clotrimazol single supp. 500 mg Postmenstrual for 6 months Oral antifungal: Daily until symptoms disapppear
- 30. BACTERIAL VAGINOSIS STD: Causative organism: Past Haemophilus or Corynebacterium vaginale Now: Gardnella vaginalis Gram Negative Bacilli
- 31. SIGNS AND SYMPTOMS Symptoms: 30-40% asymptomatic Unpleasant vaginal odour (musty or fishy odor) Vaginal discharge: thin,
- 32. Diagnosis: pH: 5-6.5 Positive odor test- mix discharge with 10% KOH – fishy odor(metabollic by product
- 33. Complication Increase risk of pelvic inflammatory disease Post operative cuff infection after hysterectomy In pregnancy, it
- 34. Management Metronidazole 500 mg twice daily for 7 days Cure is 85% it fall to 50%
- 35. Recurrent Causes: Causes: Partner STD Treatment During Pregnancy:?? The organism may predispose to PRM
- 36. PRURITUS VULVAE Definition: Means sensation of itching. It is a term used to describe a sensation
- 37. CAUSES: Pruritus: associated with vaginal discharge e.g. candida and trichomonas vaginalis. Other discharge which is purulent
- 38. Urinary condition: Incontinence: glycosuria Allergy and drug sensitivity : soaps, deodorant, antiseptic contains phenol, nylon underwear
- 39. 1. Investigation 1. History The onset, site, duration Presence or absence of vaginal discharge History of
- 40. 2. Examination General – anemia, jaundice Local examination Urine for sugar and bile Blood sugar and
- 42. Скачать презентацию
Vaginal Discharge
Vaginal discharge may be blood stained white cream, yellow, or
Vaginal Discharge
Vaginal discharge may be blood stained white cream, yellow, or
PHYSIOLOGY OF THE VAGINA
The vagina is lined by non-keratinized stratified squamous
PHYSIOLOGY OF THE VAGINA
The vagina is lined by non-keratinized stratified squamous
Lactobacilli (Duoderline Bacilli)
Convert glycogen to lactic acid
pH of the vagina
Lactobacilli (Duoderline Bacilli)
Convert glycogen to lactic acid
pH of the vagina
Vaginal Ecosystem
Dynamic equilibrium between microflora and metabollic by products of the
Vaginal Ecosystem
Dynamic equilibrium between microflora and metabollic by products of the
Factors affecting the vaginal Ecosystem
Antibiotics
Hormones or lack of hormones
Contraceptive preparations
Douches
Vaginal Medication
Sexual
Factors affecting the vaginal Ecosystem
Antibiotics
Hormones or lack of hormones
Contraceptive preparations
Douches
Vaginal Medication
Sexual
Vaginal Desquamated Tissue
Reproductive age – superfacial cells (est)
Luteal phase- Intermediate cells
Vaginal Desquamated Tissue
Reproductive age – superfacial cells (est)
Luteal phase- Intermediate cells
Differential Diagnosis
Pediatrics + Peripubertal
Physiological leukorrhea – high estrogen
Eczema
Psoriasis
Pinworm- rectum itchy
Foreign body
Differential Diagnosis
Pediatrics + Peripubertal
Physiological leukorrhea – high estrogen
Eczema
Psoriasis
Pinworm- rectum itchy
Foreign body
Investigation:
Swab for culture
PR Examination
EUA
X-RAY pelvic
Exclude sexual abuse
Management:
Hygiene
Antibiotics
Steroids
Investigation:
Swab for culture
PR Examination
EUA
X-RAY pelvic
Exclude sexual abuse
Management:
Hygiene
Antibiotics
Steroids
Post Menopausal
Exclude malignancy
Post Menopausal
Exclude malignancy
3. Reproductive Age:
1. Physiological :
Increased in pregnancy and mid cycle.
Consists
3. Reproductive Age:
1. Physiological :
Increased in pregnancy and mid cycle.
Consists
2. Infection:
Trichomonas vaginalis
Candida vaginitis
Bacterial vaginosis( non specific vaginitis)
Sexual transmitted disease
Neisseria gonorrhea,
2. Infection:
Trichomonas vaginalis
Candida vaginitis
Bacterial vaginosis( non specific vaginitis)
Sexual transmitted disease
Neisseria gonorrhea,
3. Urinary and faeculent discharge – vvv
4. Foreign body: IUCD, neglected
3. Urinary and faeculent discharge – vvv
4. Foreign body: IUCD, neglected
DIAGNOSIS
History:
Age
Type of discharge
Amount
Onset (relation to antibiotics medication relation to menstruation)
Use of
DIAGNOSIS
History:
Age
Type of discharge
Amount
Onset (relation to antibiotics medication relation to menstruation)
Use of
2. General Examination:(Anemia, Cachaxia)
Inspection of vulva
Speculum examination
Amount, consistency, characteristic, odor
Bimanual examination
2. General Examination:(Anemia, Cachaxia)
Inspection of vulva
Speculum examination
Amount, consistency, characteristic, odor
Bimanual examination
Investigation
3 Specimens
a. Wet mount smear (ad saline)
b. Swab for culture and
Investigation
3 Specimens
a. Wet mount smear (ad saline)
b. Swab for culture and
Treatment: According to the Cause
Foreign body – remove
Leukorrhoea
a. Reassurance
b.
Treatment: According to the Cause
Foreign body – remove
Leukorrhoea
a. Reassurance
b.
Vaginal Infection
Trichomonas vaginitis:
STD: 70% of males contract the disease after single
Vaginal Infection
Trichomonas vaginitis:
STD: 70% of males contract the disease after single
Signs:
Thin
Frothy
Pale
Green or gray discharge
pH 5-6.5
The organism ferment carbohydrates – Produce gas
Signs:
Thin
Frothy
Pale
Green or gray discharge
pH 5-6.5
The organism ferment carbohydrates – Produce gas
Investigation
Identify the organism in wet mount smear
The organism is pear-shaped and
Investigation
Identify the organism in wet mount smear
The organism is pear-shaped and
Management
Oral Metronidazole (flagyl)
Single dose 2 gm
500 mg P.O twice for 1
Management
Oral Metronidazole (flagyl)
Single dose 2 gm
500 mg P.O twice for 1
Causes of Treatment Failure:
Compliance
Partner as a reservoir
Treatment:
Vaginal Route
Note: Treatment
Causes of Treatment Failure:
Compliance
Partner as a reservoir
Treatment:
Vaginal Route
Note: Treatment
Candida Vaginitis: Moniliasis
Causative organisms: Candida albicans
Is not STD
CAUSES:
Hormonal factor ( O.C.P)
Depress
Candida Vaginitis: Moniliasis
Causative organisms: Candida albicans
Is not STD
CAUSES:
Hormonal factor ( O.C.P)
Depress
Symptoms: 20% asymptomatic
Pruritus
Vulvar burning
External dysuria
Dyspareunia
Vaginal discharge ( white, highly viscous, granular,
Symptoms: 20% asymptomatic
Pruritus
Vulvar burning
External dysuria
Dyspareunia
Vaginal discharge ( white, highly viscous, granular,
Signs
Erythema
Oedema
Excoriation
Pustules
Speculum: cottage cheese type of discharge
Adherent thrush patches attached to the
Signs
Erythema
Oedema
Excoriation
Pustules
Speculum: cottage cheese type of discharge
Adherent thrush patches attached to the
Investigation
1.Clinical
2. pH of the vagina norma < 4.5
3. Fungal element
Investigation
1.Clinical
2. pH of the vagina norma < 4.5
3. Fungal element
Management
Standard
Topically applied azole ( nystatin)
- 80% - 90% relief
3. Oral antifungal
Management
Standard
Topically applied azole ( nystatin)
- 80% - 90% relief
3. Oral antifungal

RECURRENT DISEASE
Definition: More than 3 episodes of infection in one year.
Causes:
Poor
RECURRENT DISEASE
Definition: More than 3 episodes of infection in one year.
Causes:
Poor
Treatment
Clotrimazol single supp. 500 mg Postmenstrual for 6 months
Oral antifungal: Daily
Treatment
Clotrimazol single supp. 500 mg Postmenstrual for 6 months
Oral antifungal: Daily
BACTERIAL VAGINOSIS
STD:
Causative organism: Past Haemophilus or Corynebacterium vaginale
Now: Gardnella vaginalis
Gram Negative
BACTERIAL VAGINOSIS
STD:
Causative organism: Past Haemophilus or Corynebacterium vaginale
Now: Gardnella vaginalis
Gram Negative
SIGNS AND SYMPTOMS
Symptoms:
30-40% asymptomatic
Unpleasant vaginal odour (musty or fishy odor)
Vaginal discharge:
SIGNS AND SYMPTOMS
Symptoms:
30-40% asymptomatic
Unpleasant vaginal odour (musty or fishy odor)
Vaginal discharge:
Diagnosis:
pH: 5-6.5
Positive odor test- mix discharge with 10% KOH – fishy
Diagnosis:
pH: 5-6.5
Positive odor test- mix discharge with 10% KOH – fishy
Complication
Increase risk of pelvic inflammatory disease
Post operative cuff infection after hysterectomy
In
Complication
Increase risk of pelvic inflammatory disease
Post operative cuff infection after hysterectomy
In
Management
Metronidazole 500 mg twice daily for 7 days
Cure is 85% it
Management
Metronidazole 500 mg twice daily for 7 days
Cure is 85% it
Recurrent Causes:
Causes:
Partner
STD
Treatment During Pregnancy:?? The organism may predispose to PRM
Recurrent Causes:
Causes:
Partner
STD
Treatment During Pregnancy:?? The organism may predispose to PRM
PRURITUS VULVAE
Definition:
Means sensation of itching. It is a term used to
PRURITUS VULVAE
Definition:
Means sensation of itching. It is a term used to

CAUSES:
Pruritus: associated with vaginal discharge e.g. candida and trichomonas vaginalis. Other
CAUSES:
Pruritus: associated with vaginal discharge e.g. candida and trichomonas vaginalis. Other
Urinary condition: Incontinence: glycosuria
Allergy and drug sensitivity : soaps, deodorant, antiseptic
Urinary condition: Incontinence: glycosuria
Allergy and drug sensitivity : soaps, deodorant, antiseptic
1. Investigation
1. History
The onset, site, duration
Presence or absence of vaginal discharge
History
1. Investigation
1. History
The onset, site, duration
Presence or absence of vaginal discharge
History
2. Examination
General – anemia, jaundice
Local examination
Urine for sugar and bile
Blood sugar
2. Examination
General – anemia, jaundice
Local examination
Urine for sugar and bile
Blood sugar
 Патологиялық анатомия
Патологиялық анатомия Оба қоздырғышы
Оба қоздырғышы Microscopic colitis
Microscopic colitis Сосудистые анастомозы РУС
Сосудистые анастомозы РУС Нарушение половых функций. Климакс
Нарушение половых функций. Климакс Мeningeal a syndrome in clinic of infectious diseases
Мeningeal a syndrome in clinic of infectious diseases Медсестринський процес – історичний нарис. Професійні організації медичних сестер
Медсестринський процес – історичний нарис. Професійні організації медичних сестер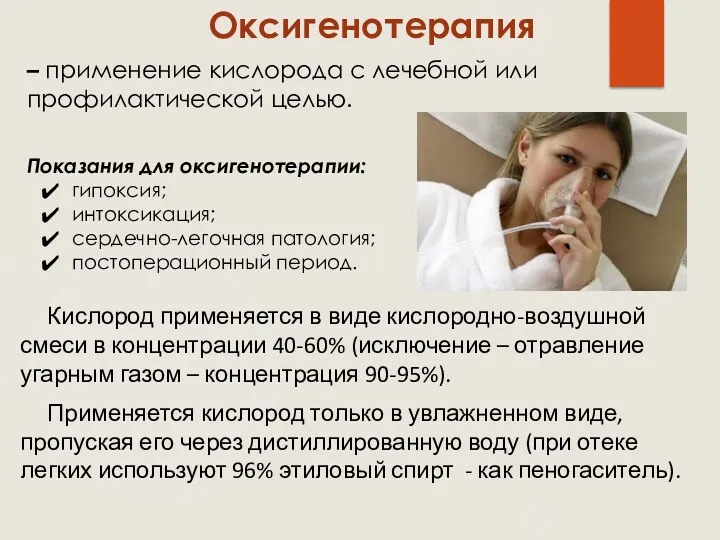 Оксигенотерапия. Виды оксигенотерапии
Оксигенотерапия. Виды оксигенотерапии Потребность в нормальном дыхании
Потребность в нормальном дыхании Cardiovascular system
Cardiovascular system Первая помощь детям при травмах и несчастных случаях. Общие советы для детей и взрослых
Первая помощь детям при травмах и несчастных случаях. Общие советы для детей и взрослых Медикаментозды остеопороз: алдын алудағы және түзетуге негізгі ұстанымдар
Медикаментозды остеопороз: алдын алудағы және түзетуге негізгі ұстанымдар Первая помощь при отморожении, общем охлаждении организма
Первая помощь при отморожении, общем охлаждении организма Обследование зубных рядов, зубов и периодонта в детском возрасте
Обследование зубных рядов, зубов и периодонта в детском возрасте Терапиялық стоматология клиникасындағы ауру сезімі және жансыздандыру
Терапиялық стоматология клиникасындағы ауру сезімі және жансыздандыру Общие вопросы лучевой диагностики. Ультразвуковое исследование
Общие вопросы лучевой диагностики. Ультразвуковое исследование Концепция обеспечения качества лекарственных средств
Концепция обеспечения качества лекарственных средств Клиническая симптоматология рака и абсцесса легких. Синдром полости в легком. (Тема 21)
Клиническая симптоматология рака и абсцесса легких. Синдром полости в легком. (Тема 21) Острая почечная и острая печеночная недостаточность
Острая почечная и острая печеночная недостаточность Ранний детский аутизм
Ранний детский аутизм Технические регламенты и национальные стандарты оказания оздоровительных услуг гостиничными организациями. (Лекция 6.1)
Технические регламенты и национальные стандарты оказания оздоровительных услуг гостиничными организациями. (Лекция 6.1) Уход за больными хирургического профиля
Уход за больными хирургического профиля Требования к организации и проведению профилактической дератизации и дезинсекции
Требования к организации и проведению профилактической дератизации и дезинсекции Периферические венозные катетеры
Периферические венозные катетеры Ортаңғы және ішкі құлақ аурулары. Саңыраулық және мылқаулық орта кұлактың жедел және созылмалы кабынуы мастоидит
Ортаңғы және ішкі құлақ аурулары. Саңыраулық және мылқаулық орта кұлактың жедел және созылмалы кабынуы мастоидит Нейропротезирование. История нейропротезирования
Нейропротезирование. История нейропротезирования Синдромы при заболеваниях дыхательной системы
Синдромы при заболеваниях дыхательной системы Первая медицинская помощь
Первая медицинская помощь