- Dydrogesterone versus micronized progesterone

Содержание
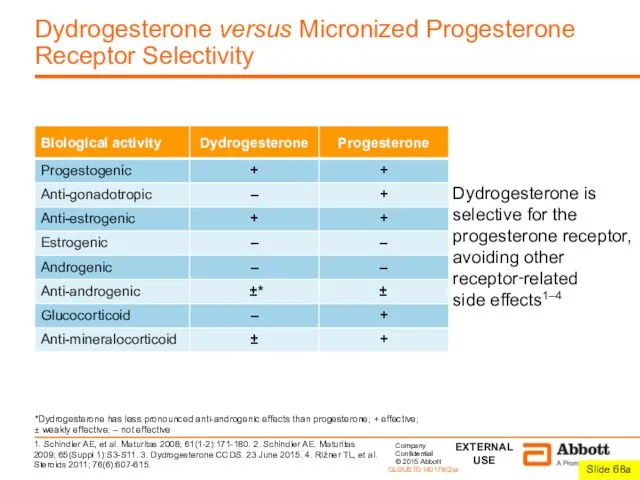
- 2. Dydrogesterone versus Micronized Progesterone Receptor Selectivity Dydrogesterone is selective for the progesterone receptor, avoiding other receptor‑related
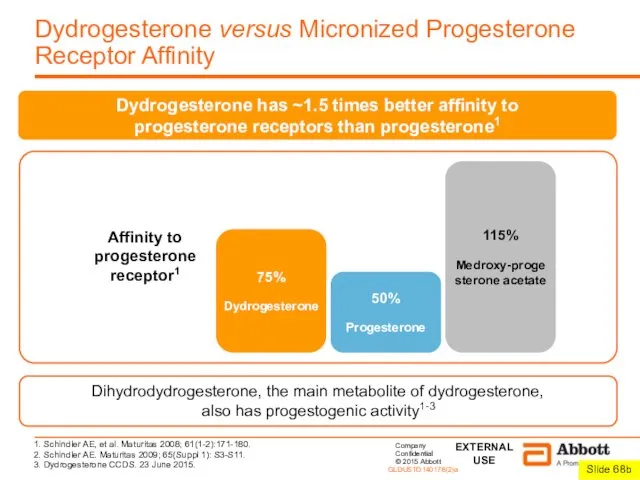
- 3. Dydrogesterone versus Micronized Progesterone Receptor Affinity 115% Medroxy-progesterone acetate 75% Dydrogesterone 50% Progesterone Affinity to progesterone
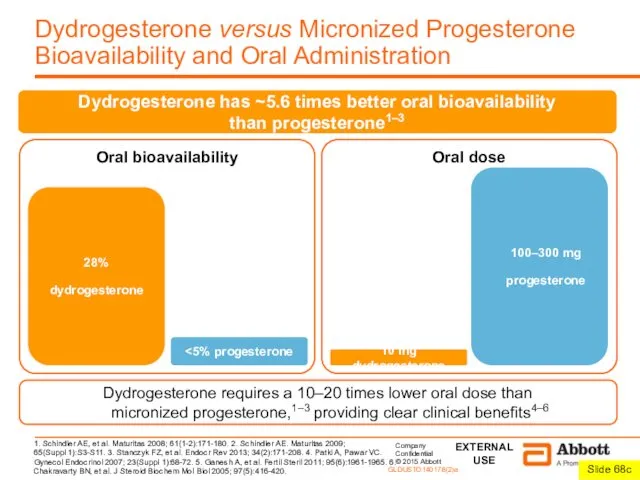
- 4. Dydrogesterone versus Micronized Progesterone Bioavailability and Oral Administration 1. Schindler AE, et al. Maturitas 2008; 61(1-2):171-180.
- 5. 1. Dydrogesterone CCDS. 23 June 2015. 2. Bulletti C, et al. Hum Reprod 1997; 12(5):1073-1079. Dydrogesterone
- 6. Dydrogesterone versus Vaginal Micronized Progesterone Safety and Tolerability Both oral and vaginal micronized progesterone are metabolized
- 7. Dydrogesterone versus Vaginal Micronized Progesterone Preference and Acceptability In studies that compared oral versus vaginal formulations
- 8. Conclusions Dydrogesterone Is produced from a natural source1 like other progestogens Is very similar to progesterone,
- 10. Скачать презентацию
Dydrogesterone versus Micronized Progesterone
Receptor Selectivity
Dydrogesterone is selective for the progesterone receptor,
Dydrogesterone versus Micronized Progesterone
Receptor Selectivity
Dydrogesterone is selective for the progesterone receptor,
Dydrogesterone versus Micronized Progesterone
Receptor Affinity
115%
Medroxy-progesterone acetate
75%
Dydrogesterone
50%
Progesterone
Affinity to progesterone receptor1
1. Schindler
Dydrogesterone versus Micronized Progesterone
Receptor Affinity
115%
Medroxy-progesterone acetate
75%
Dydrogesterone
50%
Progesterone
Affinity to progesterone receptor1
1. Schindler
Dydrogesterone versus Micronized Progesterone
Bioavailability and Oral Administration
1. Schindler AE, et al.
Dydrogesterone versus Micronized Progesterone
Bioavailability and Oral Administration
1. Schindler AE, et al.
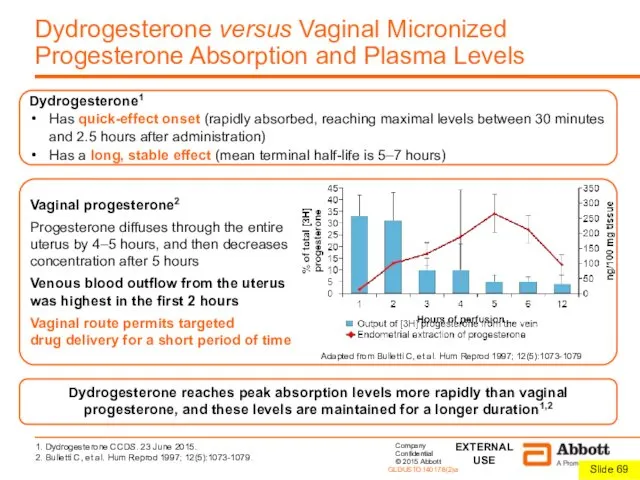
1. Dydrogesterone CCDS. 23 June 2015.
2. Bulletti C, et al. Hum
1. Dydrogesterone CCDS. 23 June 2015.
2. Bulletti C, et al. Hum
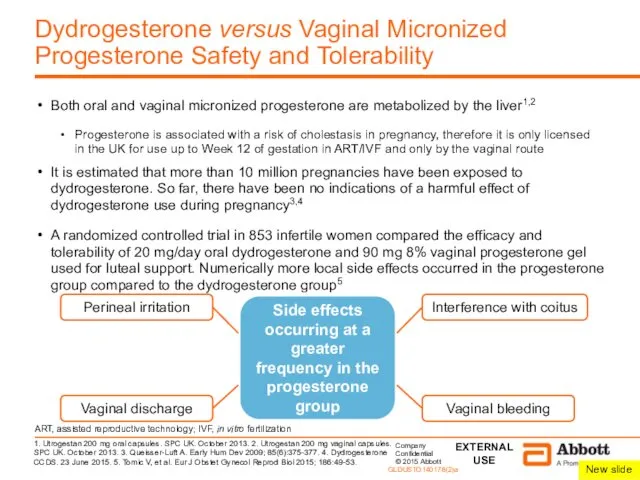
Dydrogesterone versus Vaginal Micronized Progesterone Safety and Tolerability
Both oral and vaginal
Dydrogesterone versus Vaginal Micronized Progesterone Safety and Tolerability
Both oral and vaginal
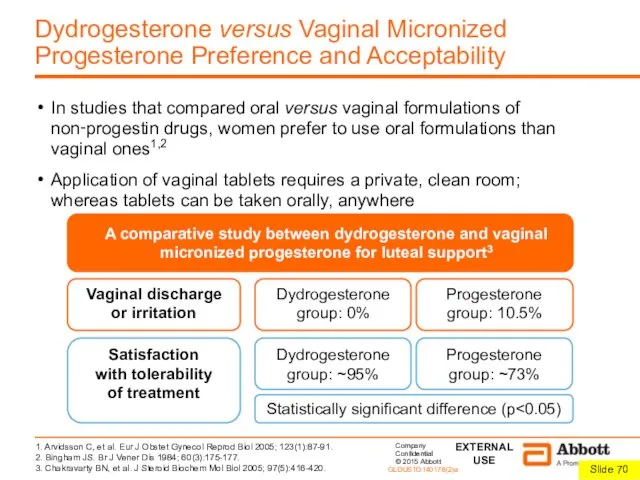
Dydrogesterone versus Vaginal Micronized Progesterone Preference and Acceptability
In studies that compared
Dydrogesterone versus Vaginal Micronized Progesterone Preference and Acceptability
In studies that compared
Conclusions
Dydrogesterone
Is produced from a natural source1 like other progestogens
Is very similar
Conclusions
Dydrogesterone
Is produced from a natural source1 like other progestogens
Is very similar
 Промежуточный мозг
Промежуточный мозг Желудочно-кишечный тракт. Пищеварительная система
Желудочно-кишечный тракт. Пищеварительная система Анатомия ствола мозга и промежуточного мозга
Анатомия ствола мозга и промежуточного мозга Плесень - вред или польза?
Плесень - вред или польза? Дыхательная система. Органы дыхания
Дыхательная система. Органы дыхания Физиология наружнего и среднего уха
Физиология наружнего и среднего уха Игра В мире животных
Игра В мире животных Химический состав клетки. Тема: Углеводы, липиды
Химический состав клетки. Тема: Углеводы, липиды Среды жизни планеты Земля. 5 класс
Среды жизни планеты Земля. 5 класс Отряд насекомоядные
Отряд насекомоядные Индивидуальное развитие организмов
Индивидуальное развитие организмов Дыхание. Газообмен между клетками и внешней средой
Дыхание. Газообмен между клетками и внешней средой Class lomotion system
Class lomotion system Anthocerotopsida (Отдел Антоцеротовые)
Anthocerotopsida (Отдел Антоцеротовые) Контрольно-обобщающий урок по теме Моллюски, или Мягкотелые
Контрольно-обобщающий урок по теме Моллюски, или Мягкотелые Индивидуальные пути обмена аминокислот. Часть 2. Лекция №14
Индивидуальные пути обмена аминокислот. Часть 2. Лекция №14 Алгоритмы биоинформатики
Алгоритмы биоинформатики Адаптации организмов
Адаптации организмов Основы селекции организмов
Основы селекции организмов Биохимия крови. Функции крови
Биохимия крови. Функции крови Вкусовой анализатор
Вкусовой анализатор Презентация Мой инновационный опыт
Презентация Мой инновационный опыт Физиология растений
Физиология растений Методическая разработка к уроку по теме Насекомые
Методическая разработка к уроку по теме Насекомые Семейство Лилейные
Семейство Лилейные Аквариумные рыбки
Аквариумные рыбки Методическая разработка - презентация к уроку в 8 классе Осанка человека и плоскостопие
Методическая разработка - презентация к уроку в 8 классе Осанка человека и плоскостопие Зоологія – наука про тварин
Зоологія – наука про тварин