- Acute myocardial infarction

Содержание
- 2. Answer: Acute myocardial infarction is the most likely diagnosis. Based on this history alone, electrocardiographic monitoring
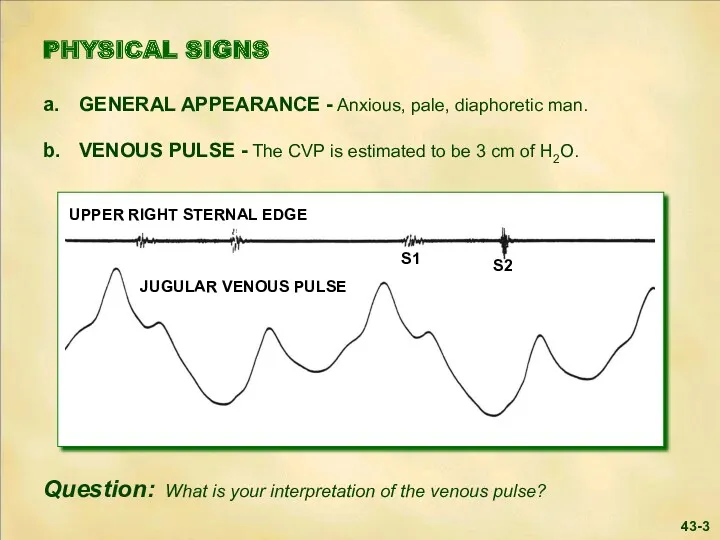
- 3. 43-3
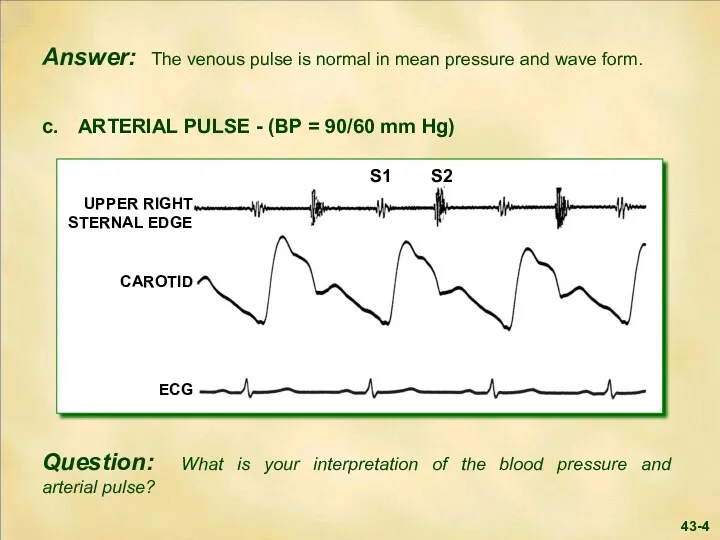
- 4. 43-4
- 5. Answer: The blood pressure is mildly decreased, while the arterial pulse contour is normal. Parasympathetic overactivity
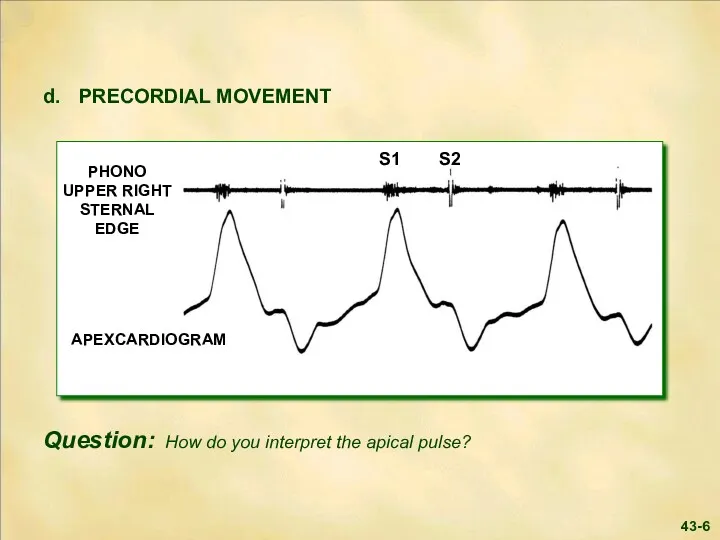
- 6. 43-6 S1 S2
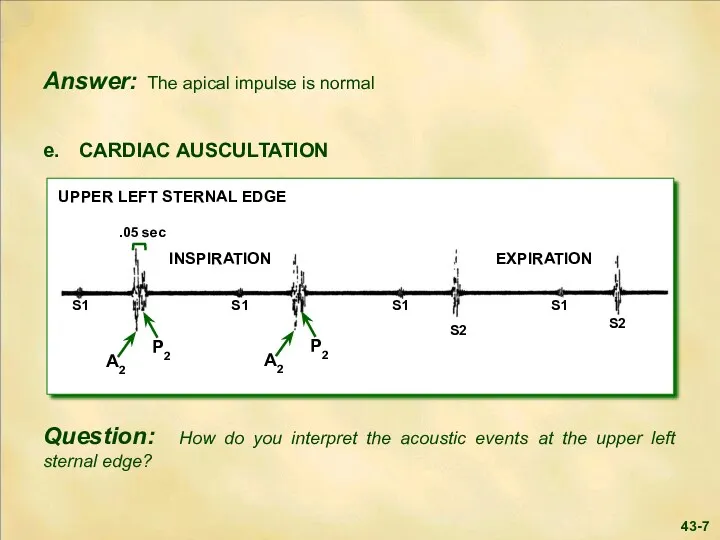
- 7. 43-7
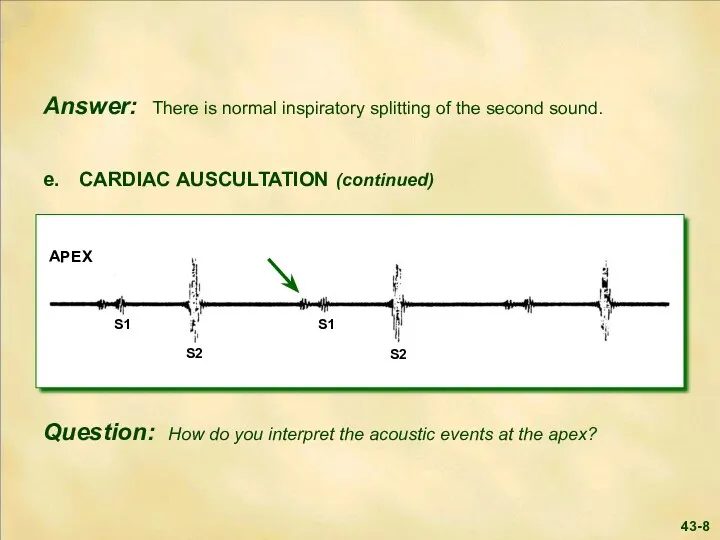
- 8. 43-8
- 9. Answer: The first heart sound at the apex is diminished in intensity. In this clinical setting,
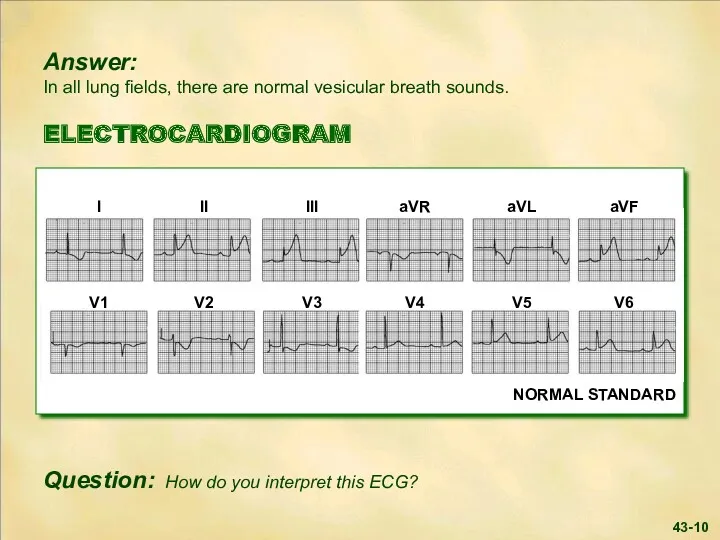
- 10. 43-10
- 11. Answer: The ECG shows marked ST segment elevation in the inferior leads with lesser elevation in
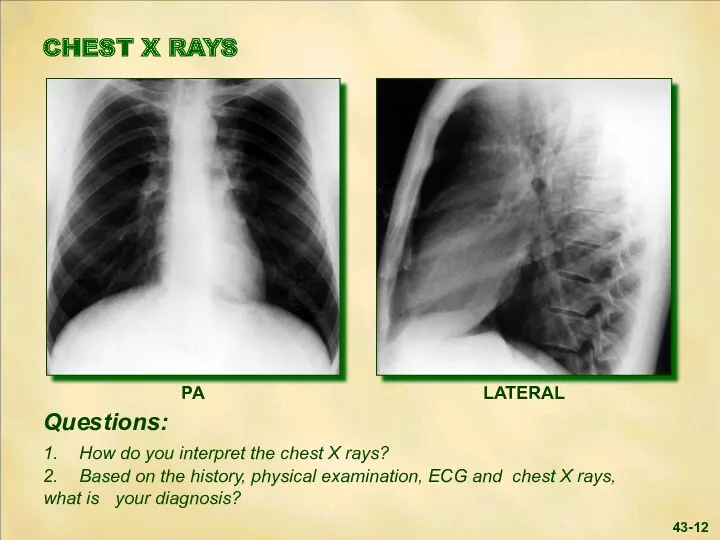
- 12. 43-12
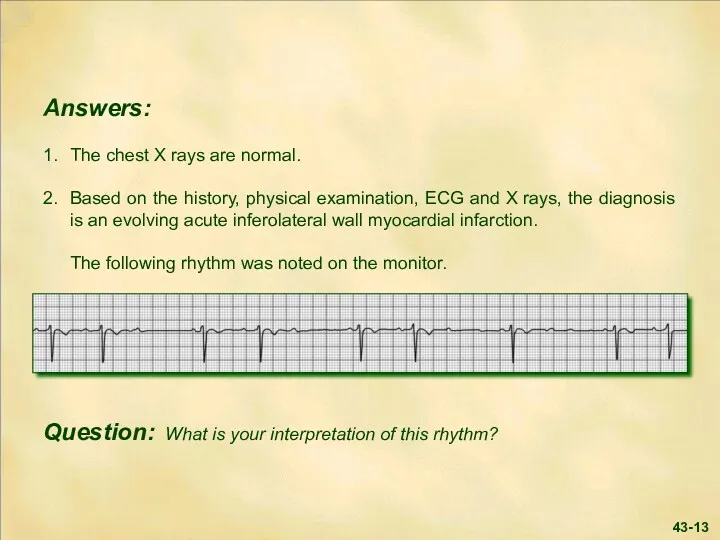
- 13. 43-13
- 14. Answer: The rhythm strip shows sinus rhythm with Mobitz Type I second degree A-V block (
- 15. Answer: Thrombosis plays an important role in ST-elevation myocardial infarction. Timely reperfusion of the occluded coronary
- 16. 43-16 Answer (continued): If full catheterization facilities are available, urgent study and percutaneous intervention is most
- 17. LABORATORY Myocardial biomarkers ordered on admission confirmed the diagnosis of infarction. Necrosis of myocardial tissue results
- 18. The patient was placed at bed rest in the CCU. Ninety minutes following thrombolytic therapy, the
- 19. 43-19
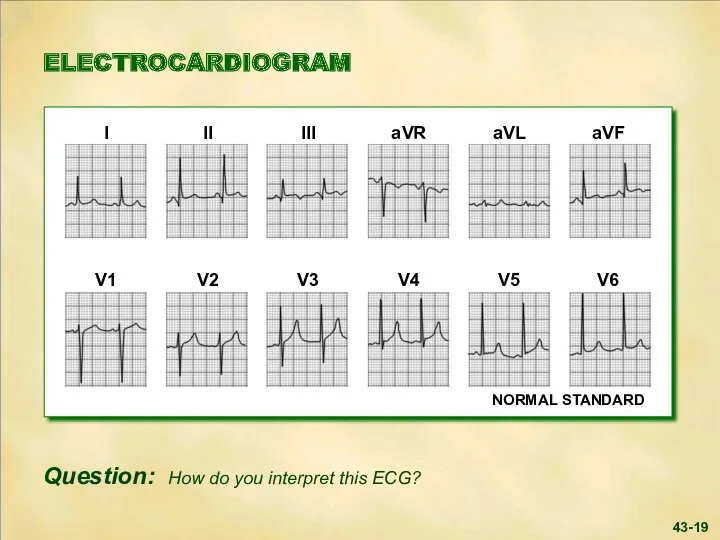
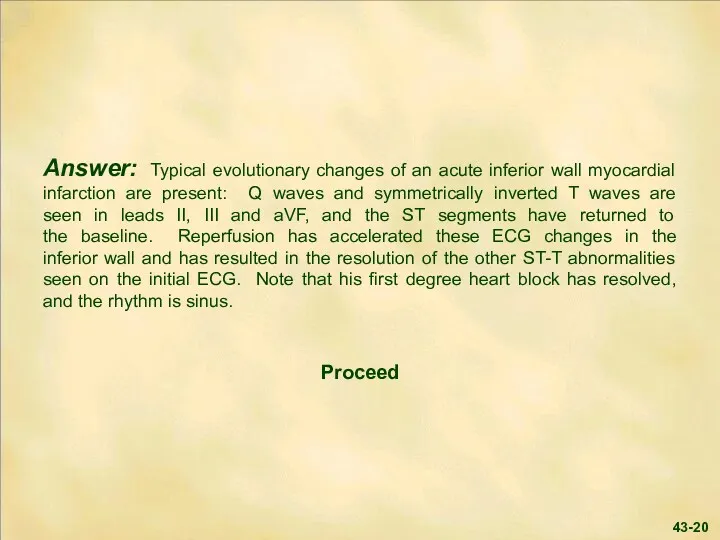
- 20. Answer: Typical evolutionary changes of an acute inferior wall myocardial infarction are present: Q waves and
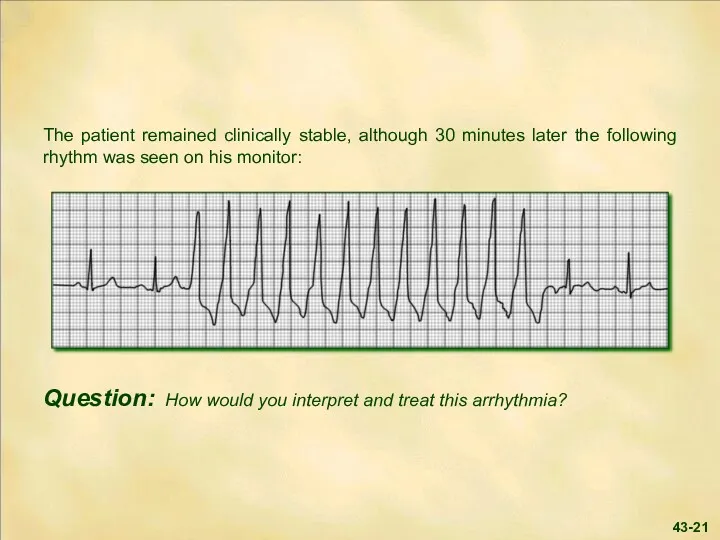
- 21. 43-21
- 22. Answer: There is a run of non-sustained ventricular tachycardia, i.e., three or more ventricular beats in
- 23. Two hours later the patient became cool and clammy, and his blood pressure dropped to 85/50
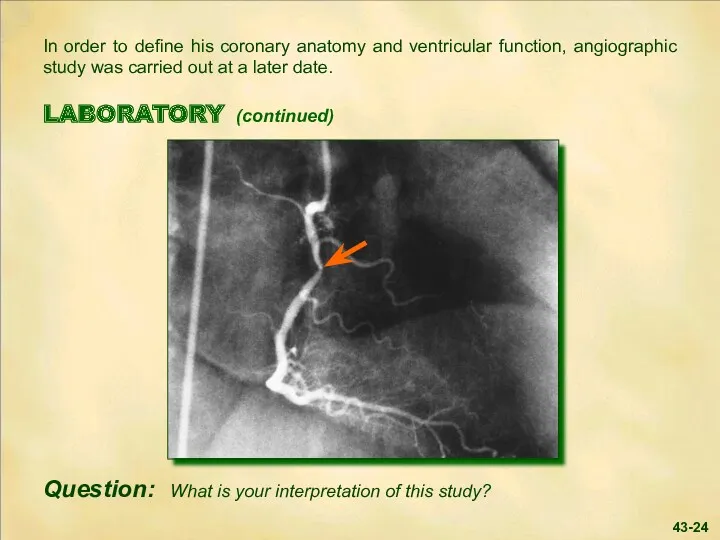
- 24. In order to define his coronary anatomy and ventricular function, angiographic study was carried out at
- 25. Answer: The right coronary angiogram shows an isolated non-critical stenosis (arrow) in the proximal right coronary
- 26. SUMMARY Coronary artery lesions range from the stable atheroma to complex lesions with thrombotic occlusion. The
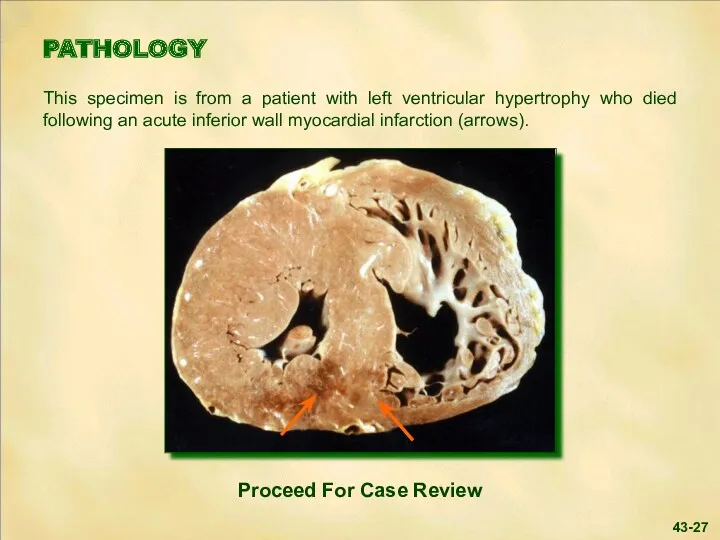
- 27. PATHOLOGY This specimen is from a patient with left ventricular hypertrophy who died following an acute
- 28. 43-28
- 29. 43-29
- 31. Скачать презентацию
Answer: Acute myocardial infarction is the most likely diagnosis.
Based on this
Answer: Acute myocardial infarction is the most likely diagnosis.
Based on this
43-3
43-3
43-4
43-4
Answer: The blood pressure is mildly decreased, while the arterial pulse
Answer: The blood pressure is mildly decreased, while the arterial pulse
43-6
S1
S2
43-6
S1
S2
43-7
43-7
43-8
43-8
Answer: The first heart sound at the apex is diminished in
Answer: The first heart sound at the apex is diminished in
43-10
43-10
Answer: The ECG shows marked ST segment elevation in the inferior
Answer: The ECG shows marked ST segment elevation in the inferior
43-12
43-12
43-13
43-13
Answer: The rhythm strip shows sinus rhythm with Mobitz Type I
Answer: The rhythm strip shows sinus rhythm with Mobitz Type I
Answer: Thrombosis plays an important role in ST-elevation myocardial infarction. Timely
Answer: Thrombosis plays an important role in ST-elevation myocardial infarction. Timely
43-16
Answer (continued): If full catheterization facilities are available, urgent study and
43-16
Answer (continued): If full catheterization facilities are available, urgent study and
LABORATORY
Myocardial biomarkers ordered on admission confirmed the diagnosis of infarction.
LABORATORY
Myocardial biomarkers ordered on admission confirmed the diagnosis of infarction.
The patient was placed at bed rest in the CCU.
Ninety minutes
The patient was placed at bed rest in the CCU.
Ninety minutes
43-19
43-19
Answer: Typical evolutionary changes of an acute inferior wall myocardial infarction
Answer: Typical evolutionary changes of an acute inferior wall myocardial infarction
43-21
43-21
Answer: There is a run of non-sustained ventricular tachycardia, i.e., three
Answer: There is a run of non-sustained ventricular tachycardia, i.e., three
Two hours later the patient became cool and clammy, and his
Two hours later the patient became cool and clammy, and his
In order to define his coronary anatomy and ventricular function, angiographic
In order to define his coronary anatomy and ventricular function, angiographic
Answer: The right coronary angiogram shows an isolated non-critical stenosis (arrow)
Answer: The right coronary angiogram shows an isolated non-critical stenosis (arrow)
SUMMARY
Coronary artery lesions range from the stable atheroma to complex lesions
SUMMARY
Coronary artery lesions range from the stable atheroma to complex lesions
PATHOLOGY
This specimen is from a patient with left ventricular hypertrophy who
PATHOLOGY
This specimen is from a patient with left ventricular hypertrophy who
43-28
43-28
43-29
43-29
 Артериальная гипертензия у беременных
Артериальная гипертензия у беременных Проблема качества жизни в контексте современной трансплантологии
Проблема качества жизни в контексте современной трансплантологии Les inlays-onlays esthétiques Procédures d’assemblage
Les inlays-onlays esthétiques Procédures d’assemblage ВКР: Сравнительная характеристика различных видов коронок и мостовидных протезов
ВКР: Сравнительная характеристика различных видов коронок и мостовидных протезов Hemolytic anemia
Hemolytic anemia Эндоскопические методы диагностики онкологических больных
Эндоскопические методы диагностики онкологических больных Leishmaniasis. Department of Infectious Diseases Leishmaniasis
Leishmaniasis. Department of Infectious Diseases Leishmaniasis ВКР: Деятельность медицинской сестры по уходу и наблюдению за пациентами при ОРВИ
ВКР: Деятельность медицинской сестры по уходу и наблюдению за пациентами при ОРВИ Острые нейроинфекции. Менингиты
Острые нейроинфекции. Менингиты Репродуктивне здоров’я молоді
Репродуктивне здоров’я молоді Оснащение формирований службы медицины катастроф по оказанию медицинской помощи в чрезвычайных ситуациях
Оснащение формирований службы медицины катастроф по оказанию медицинской помощи в чрезвычайных ситуациях Masaje al tejido conectivo
Masaje al tejido conectivo Синдром острой и хронической печеночной недостаточности
Синдром острой и хронической печеночной недостаточности Долікарська допомога
Долікарська допомога Эпилепсия
Эпилепсия Мимические мышцы лица
Мимические мышцы лица Вирусы, друзья и враги
Вирусы, друзья и враги Сестринский уход при различных заболеваниях и состояниях раздел Сестринская помощь в хирургии
Сестринский уход при различных заболеваниях и состояниях раздел Сестринская помощь в хирургии Методы обследования пациентов с патологией органов сердечно-сосудистой системы: пальпация, перкуссия, аускультация
Методы обследования пациентов с патологией органов сердечно-сосудистой системы: пальпация, перкуссия, аускультация Организация и содержание государственного ветеринарного надзора
Организация и содержание государственного ветеринарного надзора Острый живот в гинекологии
Острый живот в гинекологии Питание кормящей матери
Питание кормящей матери Анксиолитики (транквилизаторы)
Анксиолитики (транквилизаторы) Инфекционные болезни собак
Инфекционные болезни собак Токсические поражения печени
Токсические поражения печени Система здравоохранения в России
Система здравоохранения в России Тиреоидиты. Классификация
Тиреоидиты. Классификация Выделительная система
Выделительная система