- Acute respiratory diseases in children

Содержание
- 2. Plan of the lecture Etiology of ARD Transmission mechanism in ARD Hyperthermic syndrome Toxic syndrome Stridor
- 3. ARD is etiologically heterogeneous group of infectious diseases with similar epidemiologic and clinic characteristics. Typical clinical
- 4. Etiology of ARD respiratory viruses enteroviruses coronaviruses bacteria atypical microorganisms like Chlamidia, Mycoplasma, Pneumocystis fungus
- 5. As a rule ARD course isn’t severe and rarely produce complications, but sometimes it can initialize
- 6. Transmission mechanism in ARD Air way. Viruses has significantly minor sizes of particles than microbes so
- 7. Susceptibility for ARD infection is universal, but is more prominent in age of 6 mo to
- 8. The total viral serotypes count is about 180 and they cause respiratory tract affection in 95
- 9. All viruses produce very similar clinical picture – catarhhal events, running nose, cough and hyperthermia. But
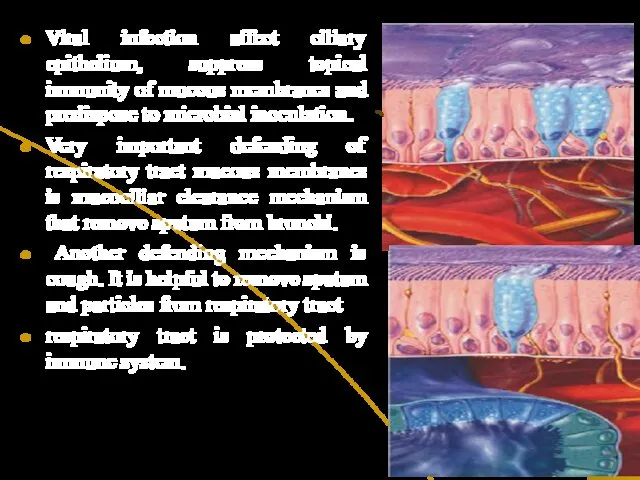
- 10. Viral infection affect ciliary epithelium, suppress topical immunity of mucous membranes and predispose to microbial inoculation.
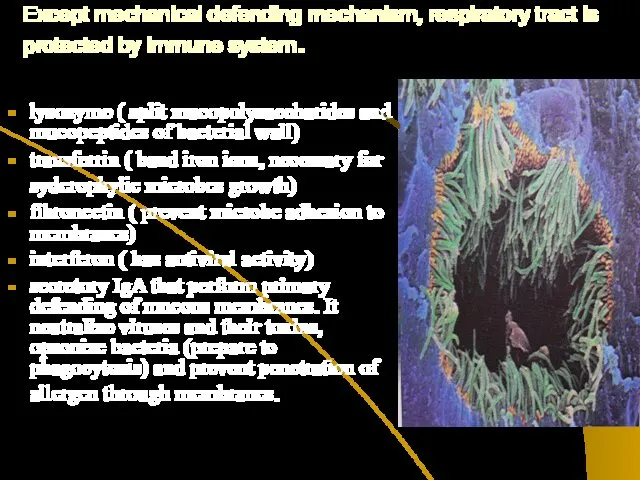
- 11. Except mechanical defending mechanism, respiratory tract is protected by immune system. lysozyme ( split mucopolysaccharides and
- 12. Neonates after birth are defended by adequate immune response. Besides this they are protected by mother’s
- 13. Fever is the protective- accommodate reaction of organism caused by pathologic agents and characterized by remodeling
- 14. Types of fever “Pink fever” or moderate hyperemia of skin. Skin is moist and hot by
- 15. Indications for antipyretic medications 1. For children without anaemnestic problems - if body T more than
- 16. Risk group for complications due to fever Children less than 2 mo old with T> 38,0
- 17. Hyperthermic syndrome is pathologic type of fever when fast raising of body T is accompanied with
- 18. Main signs of hyperthermia condition: Stable elevation of body T more than 40C within 3-6 hours
- 19. Medication choice in fever are Paracetamol Ibufen Antifebrile action of antipyretics is based on supression of
- 20. Paracetamol is the most safe antipyretic drug. It’s dosage is 10-15 mg/kg tid or 4 times
- 21. Lytic mixture is prescribed only for hyperthermia condition and “pale” fever IM Analgini 50% sol 0,1-0,2
- 22. If child has generalized convulsions it’s necessary Turn him to one side Band his head backward
- 23. To relief convulsions prescribe parenterally Diazepam (Seduxen, Relanium) 0,5% sol (5 mg in 1 ml) Dosage
- 24. Toxic syndrome –(acute infectious toxicosis, neurotoxicosis, toxic encephalopathy) is typical for initial period and has several
- 25. Irritative phase Nocturnal agitation, painful crying, fast raising of T, tachypnoe and tachycardia, elevation of BP
- 26. Typical for toxicosis changes ( edema, stasis, hemorrhages, acute dystrophy and alteration) will more visible in
- 27. Toxicosis treatment Droperidol ( adrenolytic, neuroleptic analgetic anticonvulsant and antiemetic effects) 0,1 mg/kg ( 0,3-0,5 ml
- 28. Neuro-vegetative protection is performed taking into account such rules: Lytic mixture is injected immediately in irritation
- 29. Typical symptoms of stridor Voice mutation Noisy, hoarse breathing Tachypnoe Obstructive, difficult inspiration ( in 1
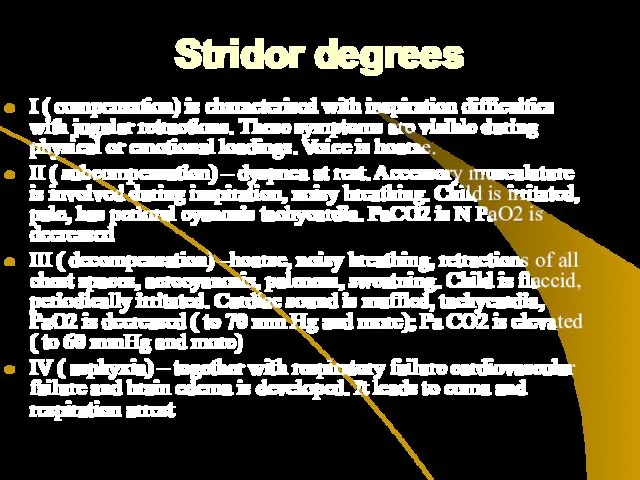
- 30. Stridor degrees I ( compensation) is characterised with inspiration difficulties with jugular retractions. These symptoms are
- 31. Treatment of stridor (only in hospital!) I degree -Fresh air access, oxygen therapy, warm bath for
- 32. Indications for invasive treatment Growing respiratory failure Pulse deficiency Heart borders dilation, decreasing of oxygen saturation
- 33. Clinical peculiarities and signs of ARD Rhinitis can be isolated or combined symptom in ARD Clinical
- 34. Rhinitis treatment is symptomatic: Nasal lavage with physiological solution Decongestants ( xylomethazoline, nafazoline, oxymetazoline) in spray
- 35. Pharyngitis - mucous layer inflammation of pharynx. It is frequently combined with rhinitis and is called
- 36. Pharyngitis treatment Proper feeding Gargling by antiseptic phytosolutions Sea salt solutions inhalations Lysozym in tablets Topical
- 37. Etiotropic therapy in ARD For influenza treatment (especially A2) – Remantadin may be prescribed (antiviral action
- 38. Etiotropic therapy in ARD Arbidol –interferon inductor. Dosages 6-12 y.o.0,1, 12 y.o. –older -0,2 4 times
- 39. Etiotropic therapy in ARD Interferones –are proteins that are synthesized by leucocytes and have properties of
- 40. Etiotropic therapy in ARD Combined medication (Viferone – Reaferone +Vit E and VitC) is produced in
- 41. Indications for antibiotics in ARD Recurrent otitis in anamnesis Children of first 6 mo with severe
- 43. Скачать презентацию
Plan of the lecture
Etiology of ARD
Transmission mechanism in ARD
Hyperthermic syndrome
Toxic
Plan of the lecture
Etiology of ARD
Transmission mechanism in ARD
Hyperthermic syndrome
Toxic
ARD is etiologically heterogeneous group of infectious diseases with similar epidemiologic
ARD is etiologically heterogeneous group of infectious diseases with similar epidemiologic
Etiology of ARD
respiratory viruses
enteroviruses
coronaviruses
bacteria
atypical microorganisms like
Etiology of ARD
respiratory viruses
enteroviruses
coronaviruses
bacteria
atypical microorganisms like
As a rule ARD course isn’t severe and rarely produce
As a rule ARD course isn’t severe and rarely produce
Transmission mechanism in ARD
Air way. Viruses has significantly minor sizes
Transmission mechanism in ARD
Air way. Viruses has significantly minor sizes
Susceptibility for ARD infection is universal, but is more prominent
Susceptibility for ARD infection is universal, but is more prominent
The total viral serotypes count is about 180 and they cause
The total viral serotypes count is about 180 and they cause
All viruses produce very similar clinical picture – catarhhal events,
All viruses produce very similar clinical picture – catarhhal events,
Viral infection affect ciliary epithelium, suppress topical immunity of mucous membranes
Viral infection affect ciliary epithelium, suppress topical immunity of mucous membranes
Except mechanical defending mechanism, respiratory tract is protected by immune system.
Except mechanical defending mechanism, respiratory tract is protected by immune system.
Neonates after birth are defended by adequate immune response. Besides
Neonates after birth are defended by adequate immune response. Besides
Fever is the protective- accommodate reaction of organism caused by pathologic
Fever is the protective- accommodate reaction of organism caused by pathologic
Types of fever
“Pink fever” or moderate hyperemia of skin. Skin is
Types of fever
“Pink fever” or moderate hyperemia of skin. Skin is
Indications for antipyretic medications
1. For children without anaemnestic problems
- if
Indications for antipyretic medications
1. For children without anaemnestic problems
- if
Risk group for complications due to fever
Children less than 2
Risk group for complications due to fever
Children less than 2
Hyperthermic syndrome is pathologic type of fever when fast raising of
Hyperthermic syndrome is pathologic type of fever when fast raising of
Main signs of hyperthermia condition:
Stable elevation of body T more than
Main signs of hyperthermia condition:
Stable elevation of body T more than
Medication choice in fever are
Paracetamol
Ibufen
Antifebrile action of antipyretics is based
Medication choice in fever are
Paracetamol
Ibufen
Antifebrile action of antipyretics is based
Paracetamol is the most safe antipyretic drug. It’s dosage is
Paracetamol is the most safe antipyretic drug. It’s dosage is
Lytic mixture is prescribed only for hyperthermia condition and “pale” fever
Lytic mixture is prescribed only for hyperthermia condition and “pale” fever
If child has generalized convulsions it’s necessary
Turn him to one
If child has generalized convulsions it’s necessary
Turn him to one
To relief convulsions prescribe parenterally
Diazepam (Seduxen, Relanium) 0,5% sol (5
To relief convulsions prescribe parenterally
Diazepam (Seduxen, Relanium) 0,5% sol (5
Toxic syndrome –(acute infectious toxicosis, neurotoxicosis, toxic encephalopathy) is typical for
Toxic syndrome –(acute infectious toxicosis, neurotoxicosis, toxic encephalopathy) is typical for
Irritative phase Nocturnal agitation, painful crying, fast raising of T, tachypnoe
Irritative phase Nocturnal agitation, painful crying, fast raising of T, tachypnoe
Typical for toxicosis changes ( edema, stasis, hemorrhages, acute dystrophy
Typical for toxicosis changes ( edema, stasis, hemorrhages, acute dystrophy
Toxicosis treatment
Droperidol ( adrenolytic, neuroleptic analgetic anticonvulsant and antiemetic effects)
Toxicosis treatment
Droperidol ( adrenolytic, neuroleptic analgetic anticonvulsant and antiemetic effects)
Neuro-vegetative protection is performed taking into account such rules:
Lytic mixture is
Neuro-vegetative protection is performed taking into account such rules:
Lytic mixture is
Typical symptoms of stridor
Voice mutation
Noisy, hoarse breathing
Tachypnoe
Obstructive, difficult inspiration ( in
Typical symptoms of stridor
Voice mutation
Noisy, hoarse breathing
Tachypnoe
Obstructive, difficult inspiration ( in
Stridor degrees
I ( compensation) is characterised with inspiration difficulties with jugular
Stridor degrees
I ( compensation) is characterised with inspiration difficulties with jugular
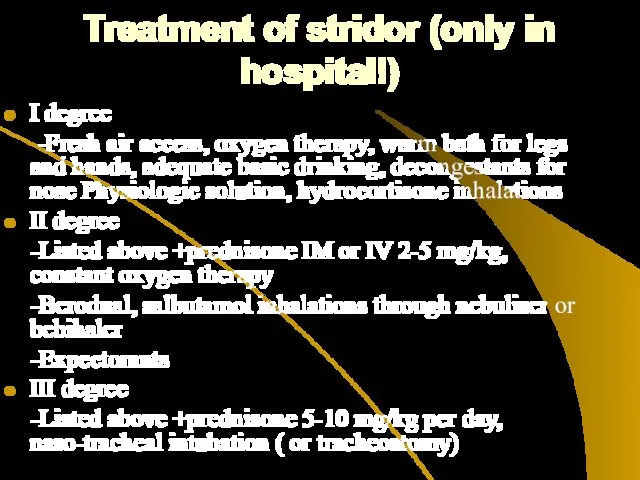
Treatment of stridor (only in hospital!)
I degree
-Fresh air access,
Treatment of stridor (only in hospital!)
I degree
-Fresh air access,
Indications for invasive treatment
Growing respiratory failure
Pulse deficiency
Heart borders dilation, decreasing of
Indications for invasive treatment
Growing respiratory failure
Pulse deficiency
Heart borders dilation, decreasing of
Clinical peculiarities and signs of ARD
Rhinitis can be isolated or combined
Clinical peculiarities and signs of ARD
Rhinitis can be isolated or combined
Rhinitis treatment is symptomatic:
Nasal lavage with physiological solution
Decongestants ( xylomethazoline, nafazoline,
Rhinitis treatment is symptomatic:
Nasal lavage with physiological solution
Decongestants ( xylomethazoline, nafazoline,
Pharyngitis - mucous layer inflammation of pharynx. It is frequently combined
Pharyngitis - mucous layer inflammation of pharynx. It is frequently combined
Pharyngitis treatment
Proper feeding
Gargling by antiseptic phytosolutions
Sea salt solutions inhalations
Lysozym in tablets
Topical
Pharyngitis treatment
Proper feeding
Gargling by antiseptic phytosolutions
Sea salt solutions inhalations
Lysozym in tablets
Topical
Etiotropic therapy in ARD
For influenza treatment (especially A2) – Remantadin may
Etiotropic therapy in ARD
For influenza treatment (especially A2) – Remantadin may
Etiotropic therapy in ARD
Arbidol –interferon inductor. Dosages 6-12 y.o.0,1, 12
Etiotropic therapy in ARD
Arbidol –interferon inductor. Dosages 6-12 y.o.0,1, 12
Etiotropic therapy in ARD
Interferones –are proteins that are synthesized by
Etiotropic therapy in ARD
Interferones –are proteins that are synthesized by
Etiotropic therapy in ARD
Combined medication (Viferone – Reaferone +Vit E
Etiotropic therapy in ARD
Combined medication (Viferone – Reaferone +Vit E
Indications for antibiotics in ARD
Recurrent otitis in anamnesis
Children of first
Indications for antibiotics in ARD
Recurrent otitis in anamnesis
Children of first
 Diabetes mellitus. (Subject 8)
Diabetes mellitus. (Subject 8) Омолаживающие операции на лице и шее
Омолаживающие операции на лице и шее Переход к системе непрерывного медицинского (фармацевтического) образования
Переход к системе непрерывного медицинского (фармацевтического) образования Контрацепция для подростков
Контрацепция для подростков Правовая и юридическая база сестринского дела
Правовая и юридическая база сестринского дела Ультразвуковая диагностика внематочной беременности
Ультразвуковая диагностика внематочной беременности Нәрестелер иммунитетіндегі иммуноглобулиндердің ролі
Нәрестелер иммунитетіндегі иммуноглобулиндердің ролі Физиотерапия, кинезитерапия при травматических повреждениях
Физиотерапия, кинезитерапия при травматических повреждениях Повреждение ключицы. Лечение
Повреждение ключицы. Лечение Рентгенодиагностика при хроническом бруцеллезе
Рентгенодиагностика при хроническом бруцеллезе Клубные наркотики
Клубные наркотики Современное представление о нормальных родах
Современное представление о нормальных родах Клинико-фармакологические подходы к выбору и применению антиаритмических лекарственных средств
Клинико-фармакологические подходы к выбору и применению антиаритмических лекарственных средств Бронхиальная астма
Бронхиальная астма Первая медицинская помощь при травмах
Первая медицинская помощь при травмах Роль медицинской сестры при уходе за пациентами с сахарным диабетом II типа. Участие в лечебно-диагностических процессах
Роль медицинской сестры при уходе за пациентами с сахарным диабетом II типа. Участие в лечебно-диагностических процессах Врачебная этика И. Канта
Врачебная этика И. Канта Хроническое воспаление. Гранулематозное и специфическое воспаление
Хроническое воспаление. Гранулематозное и специфическое воспаление Лечение ХОБЛ и бронхиальной астмы
Лечение ХОБЛ и бронхиальной астмы Чипсы: польза или вред
Чипсы: польза или вред Ошибки лабораторной диагностики. Нормативно-правовая база
Ошибки лабораторной диагностики. Нормативно-правовая база Клиника интеллектуальных нарушений при деменции
Клиника интеллектуальных нарушений при деменции Введение в эпидемиологию. Основы учения об эпидемическом процессе. Место эпидемиологии в структуре медицинских наук
Введение в эпидемиологию. Основы учения об эпидемическом процессе. Место эпидемиологии в структуре медицинских наук Профессиональное здоровье педагогов по результатам социологического опроса
Профессиональное здоровье педагогов по результатам социологического опроса Turner syndrome
Turner syndrome Недоношенные новорожденные
Недоношенные новорожденные Лечение артериальной гипертензии в сочетании с сахарным диабетом
Лечение артериальной гипертензии в сочетании с сахарным диабетом Бүйрек-тас ауруы
Бүйрек-тас ауруы