- Биомаркеры ишемического инсульта

Содержание
- 2. Актуальность темы: Существует множество факторов риска, таких как АГ, атеросклероз, СД 2типа, курение, которые предрасполагают людей
- 3. Гипотеза
- 4. Гипотеза:
- 5. Цель исследования: основная цель этого исследования - охарактеризовать профили miRNA у пациентов с ишемическим инсультом низкого
- 6. Задачи исследования: Произвести литературный обзор. Набрать группу пациентов в инсультных центрах г.Актобе молодого возраста либо с
- 7. Дизайн исследования: Исследование «серий случаев», так мы подбираем пациентов молодого возраста, или пациентов без факторов риска
- 8. Выборка: Акцидентная выборка(удобная, произвольная) В исследования были взяты пациенты , находившиеся на базах инсультного центра г.
- 9. Критерии включения: Пациенты от 18 лет до 42 лет . Наличие ишемического инсульта.
- 10. Критерии исключения: Пациенты, с артериальной гипертензией. Пациенты, с сахарным диабетом II типа Пациенты, с повышенным липидным
- 11. Этические аспекты: Одобрено КЭ Информированное согласие с полным раскрытием всей необходимой информацией на понятном языке (на
- 12. Исследовательский вопрос:
- 13. Blood microRNAs in Low or No Risk Ischemic Stroke Patients 1. Introduction Ischemic stroke is a
- 14. 3.Experimental Section This study was approved by the Medical Ethics Committee of the University Malaya Medical
- 15. Исследовательский вопрос по статье: Вопрос: Различаются ли молекулярная основа патологии инсульта у пациентов с низким или
- 16. Дизайн исследования по статье: Когортное исследование. Способ формирования выборки: Выборка –удобная выборка, пациенты находящие на лечении
- 17. Критерии включения по статье: Пациенты от 18 лет до 42 лет с ИИ. Пациенты от 42
- 18. Критерии исключения: Пациенты, у которых имеются факторы риска: В нашей базе данных факторы риска были определены
- 20. Скачать презентацию
Актуальность темы:
Существует множество факторов риска, таких как АГ, атеросклероз, СД 2типа,
Актуальность темы:
Существует множество факторов риска, таких как АГ, атеросклероз, СД 2типа,
Гипотеза
Гипотеза
Гипотеза:
Гипотеза:
Цель исследования:
основная цель этого исследования - охарактеризовать профили miRNA у пациентов
Цель исследования:
основная цель этого исследования - охарактеризовать профили miRNA у пациентов
Задачи исследования:
Произвести литературный обзор.
Набрать группу пациентов в инсультных центрах г.Актобе молодого
Задачи исследования:
Произвести литературный обзор.
Набрать группу пациентов в инсультных центрах г.Актобе молодого
Дизайн исследования:
Исследование «серий случаев», так мы подбираем пациентов молодого возраста, или
Дизайн исследования:
Исследование «серий случаев», так мы подбираем пациентов молодого возраста, или
Выборка:
Акцидентная выборка(удобная, произвольная)
В исследования были взяты пациенты , находившиеся на базах
Выборка:
Акцидентная выборка(удобная, произвольная)
В исследования были взяты пациенты , находившиеся на базах
Критерии включения:
Пациенты от 18 лет до 42 лет .
Наличие ишемического инсульта.
Критерии включения:
Пациенты от 18 лет до 42 лет .
Наличие ишемического инсульта.
Критерии исключения:
Пациенты, с артериальной гипертензией.
Пациенты, с сахарным диабетом II типа
Пациенты, с
Критерии исключения:
Пациенты, с артериальной гипертензией.
Пациенты, с сахарным диабетом II типа
Пациенты, с
Этические аспекты:
Одобрено КЭ
Информированное согласие с полным раскрытием всей необходимой информацией на
Этические аспекты:
Одобрено КЭ
Информированное согласие с полным раскрытием всей необходимой информацией на
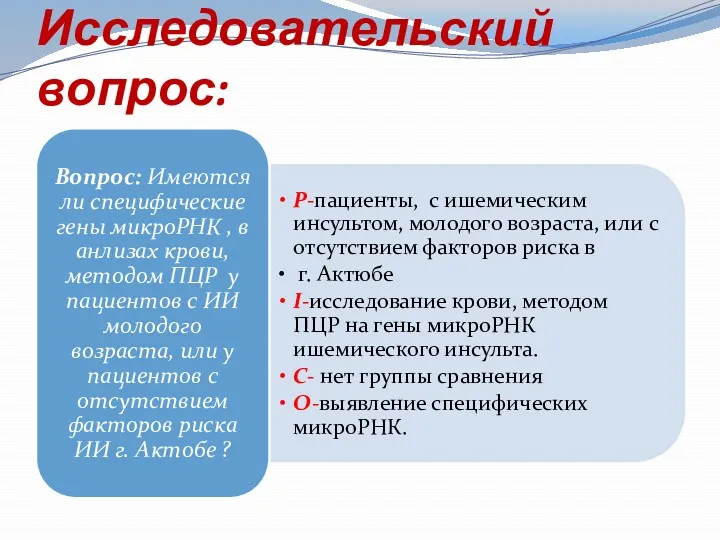
Исследовательский вопрос:
Исследовательский вопрос:
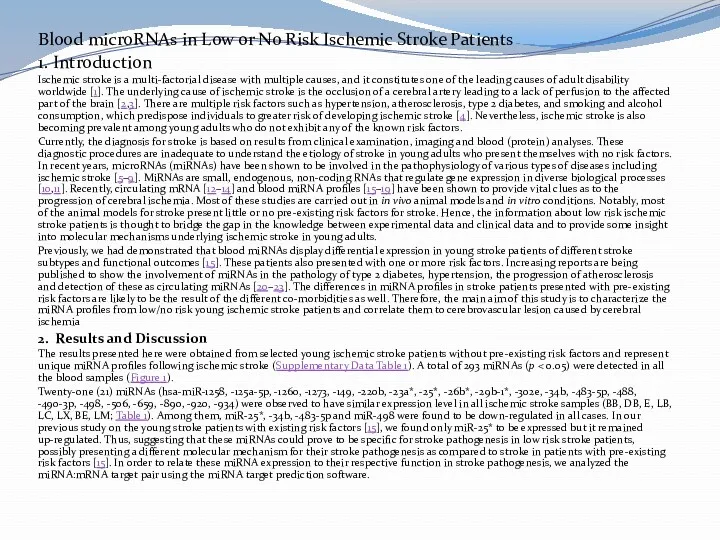
Blood microRNAs in Low or No Risk Ischemic Stroke Patients
1. Introduction
Ischemic
Blood microRNAs in Low or No Risk Ischemic Stroke Patients
1. Introduction
Ischemic
3.Experimental Section
This study was approved by the Medical Ethics Committee of
3.Experimental Section
This study was approved by the Medical Ethics Committee of
Исследовательский вопрос по статье:
Вопрос: Различаются ли молекулярная основа патологии инсульта у
Исследовательский вопрос по статье:
Вопрос: Различаются ли молекулярная основа патологии инсульта у
Дизайн исследования по статье:
Когортное исследование.
Способ формирования выборки:
Выборка –удобная выборка, пациенты находящие
Дизайн исследования по статье:
Когортное исследование.
Способ формирования выборки:
Выборка –удобная выборка, пациенты находящие
Критерии включения по статье:
Пациенты от 18 лет до 42 лет с
Критерии включения по статье:
Пациенты от 18 лет до 42 лет с
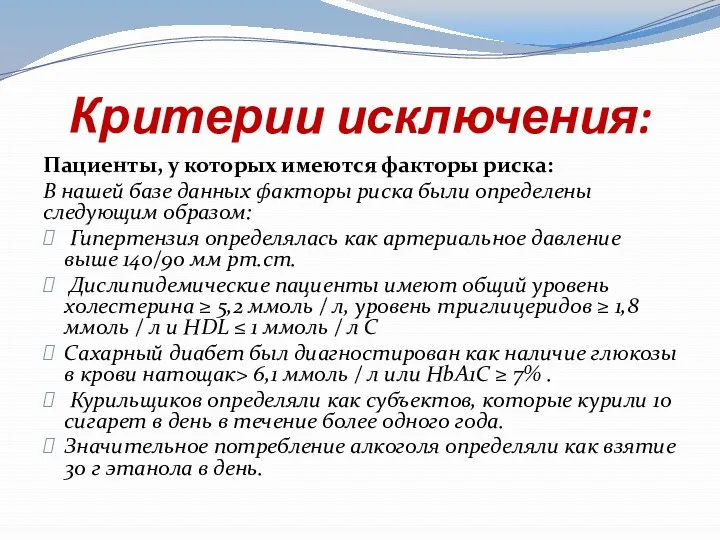
Критерии исключения:
Пациенты, у которых имеются факторы риска:
В нашей базе данных факторы
Критерии исключения:
Пациенты, у которых имеются факторы риска:
В нашей базе данных факторы
Похожие презентации
 Двухслойные базисы протезов при полном отсутствии зубов
Двухслойные базисы протезов при полном отсутствии зубов Гастроэзофагиальді рефлюкс
Гастроэзофагиальді рефлюкс Ортодонтияда иновациялық емдеу әдістері, инвизилайн (invisalign) жүйесі
Ортодонтияда иновациялық емдеу әдістері, инвизилайн (invisalign) жүйесі Захворювання молочної залози та шийки матки
Захворювання молочної залози та шийки матки Угревая болезнь (акне): актуальность проблемы, этиология, патогенез, клиника
Угревая болезнь (акне): актуальность проблемы, этиология, патогенез, клиника Суппозиторийлер өндірісінде қолданылатын негіздер, олардың жіктелуі, номенклатурасы
Суппозиторийлер өндірісінде қолданылатын негіздер, олардың жіктелуі, номенклатурасы Организация амбулаторно-поликлинической помощи новорожденным в Республике Казахстан
Организация амбулаторно-поликлинической помощи новорожденным в Республике Казахстан Паралич гортани
Паралич гортани Анализ ухода за волосами разных типов и выбор способа ухода за волосами
Анализ ухода за волосами разных типов и выбор способа ухода за волосами Anhui Greenland Biotech Co. Ltd
Anhui Greenland Biotech Co. Ltd Профилактика чрезмерного употребления алкоголя
Профилактика чрезмерного употребления алкоголя ЛФ упруго-вязко-пластичной консистенций. Мази
ЛФ упруго-вязко-пластичной консистенций. Мази Заболевания передающиеся половым путём
Заболевания передающиеся половым путём Лечение синдромов инфекционных заболеваний. Инфекционная лихорадка у детей
Лечение синдромов инфекционных заболеваний. Инфекционная лихорадка у детей Drug allergy: the mechanisms of development, symptoms, diagnostics, and treatment. Measures preventing the drug allergy
Drug allergy: the mechanisms of development, symptoms, diagnostics, and treatment. Measures preventing the drug allergy Требования к условиям труда медицинских работников и правилам личной гигиены пациентов
Требования к условиям труда медицинских работников и правилам личной гигиены пациентов Ісіктік процесстің зертханалық диагностикасы
Ісіктік процесстің зертханалық диагностикасы Ас қорыту жүйесіне жалпы шолу
Ас қорыту жүйесіне жалпы шолу Гипоксия. Классификация гипоксии
Гипоксия. Классификация гипоксии Зрительные функции. Орган зрения
Зрительные функции. Орган зрения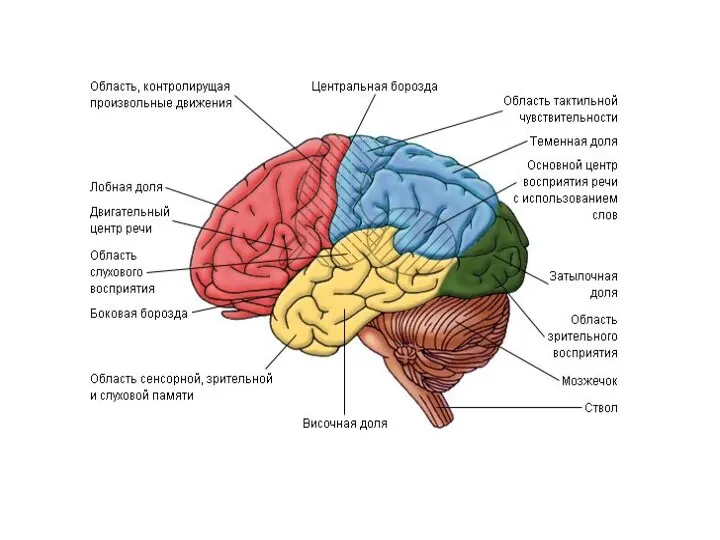 Поражения лобной доли
Поражения лобной доли Заболевания желудка и двенадцатиперсной кишки. Лекция №3
Заболевания желудка и двенадцатиперсной кишки. Лекция №3 Повреждения позвоночника
Повреждения позвоночника Congenital Adrenal Hyperplasia
Congenital Adrenal Hyperplasia
 Артриты, вызываемые инфекционными агентами. Клинические проявления. Диффериенциальный диагноз. Принципы лечения
Артриты, вызываемые инфекционными агентами. Клинические проявления. Диффериенциальный диагноз. Принципы лечения Неонатальный скрининг
Неонатальный скрининг Осложнения сахарного диабета
Осложнения сахарного диабета