- Chronic Rheumatic Heart Disease

Содержание
- 2. The diagnosis of heart disease must be * Etiological: → (Congenital - Rheumatic) * Anatomical: →
- 3. Occurs in severe cardiac involvement during initial or recurrent attacks of ARF Left - sided heart
- 4. MITRAL REGURGE (MR, Insufficiency, Regurgitation, Incompetence) The mitral valve consists of: an annulus 2 leaflets (
- 5. Healing of ARF results in Fibrosis & contracture of leaflets Shortening & thickening of chordea tendinea.
- 6. Mild MR → no symptoms Severe MR → Symptoms of HF, pulmonary congestion, pulmonary edema dyspnea
- 7. Signs: Apex → (LV apex), shifted downward, localized, forcible, hyperdynamic (ill sustained) with systolic thrill. S1
- 8. Mitral regurge CXR Mitral regurge Echocardiography
- 9. 1- VSD: -maximal intensity over the 3rd & 4th left intercostal spaces -propagated in fan manner
- 10. Prophylaxis → Against rheumatic recurrences (LONG ACTING PENECILLIN) → Against infective endocarditis Medical treatment of heart
- 11. MITRAL STENOSIS (MS) Pathophysiology -Thickening of valve leaflets - Fusion of commissures - Shortening & thickening
- 12. The clinical course depends on the severity of MS. Symptoms: Dyspnea on exertion. Orthopnea & paroxysmal
- 13. Signs Signs of RV hypertrophy: a- The apex is diffuse and shifted outward (RV apex), diastolic
- 14. Mitral stenosis CXR Mitral stenosis echo
- 15. Mitral flow murmur (functional MS) associated with large VSD, PDA, MR, AR (Austin flint murmur) -
- 16. Prophylaxis → Against rheumatic recurrences (LONG ACTING PENECILLIN) → Against infective endocarditis Medical treatment: Heart failure
- 17. Combined MS and MR Dilatation, scaring and narrowing → stenosis & leakage Obstruction and leakage of
- 18. Which of the following pathological change occur in rheumatic mitral stenosis ? Increased left atrial pressure
- 19. Rheumatic AR is the result of fibrosis and contracture of the aortic valve structure Hemodynamically AR
- 20. Symptoms Depend on the severity. In moderate and severe cases: Effort intolerance, palpitation, dyspnea, orthopnea &
- 21. The rapid run off of the blood from aorta during diastole causes the signs of hyperdynamic
- 22. * Manifestations of LV enlargement. The apex is shifted downword, forcible, localized and hyperdynamic (ill sustained)
- 23. Aortic regurge CXR Aortic regurge Echocardiography
- 24. Prophylaxis → Against rheumatic recurrences (LONG ACTING PENECILLIN) → Against infective endocarditis Surgery: Aortic valve replacement.
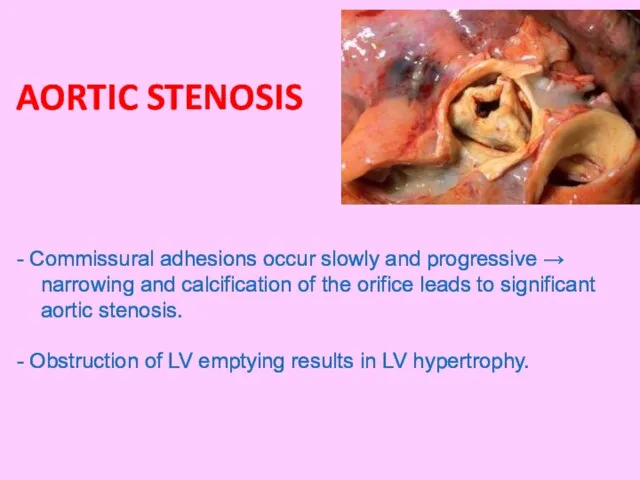
- 25. AORTIC STENOSIS - Commissural adhesions occur slowly and progressive → narrowing and calcification of the orifice
- 26. In cases with severe stenosis: Chest pain, exercise intolerance, dyspnea, syncope. Clinical manifestations: Symptoms:
- 27. - The apex: Localized, forceful & sustained (pressure overload). - Systolic thrill is common on Rt
- 28. Aortic stenosis CXR Aortic stenosis Echocardiography shows morphology of the valve and degree of stenosis.
- 29. → Against rheumatic recurrences (LONG ACTING PENECILLIN) → Against infective endocarditis Surgical intervention by valve replacement.
- 30. A case with dilated left ventricle and normal size of the other chamber. The most likely
- 32. Скачать презентацию
The diagnosis of heart disease must be
* Etiological: → (Congenital -
The diagnosis of heart disease must be
* Etiological: → (Congenital -
Occurs in severe cardiac
involvement during initial or
recurrent attacks of
Occurs in severe cardiac
involvement during initial or
recurrent attacks of
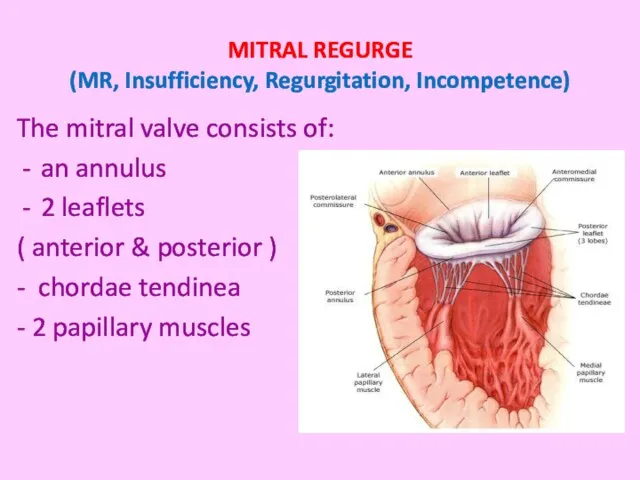
MITRAL REGURGE
(MR, Insufficiency, Regurgitation, Incompetence)
The mitral valve consists of:
an annulus
MITRAL REGURGE
(MR, Insufficiency, Regurgitation, Incompetence)
The mitral valve consists of:
an annulus
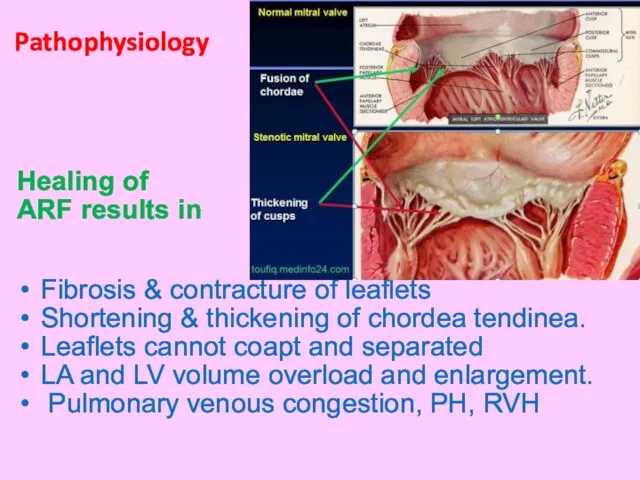
Healing of
ARF results in
Fibrosis & contracture of leaflets
Shortening &
Healing of
ARF results in
Fibrosis & contracture of leaflets
Shortening &
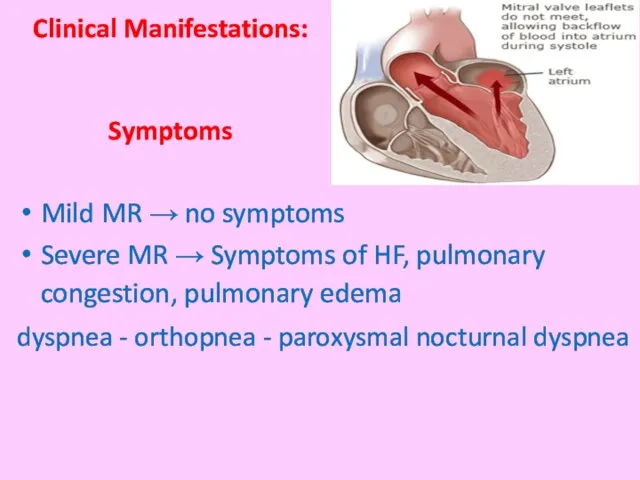
Mild MR → no symptoms
Severe MR → Symptoms of HF, pulmonary
Severe MR → Symptoms of HF, pulmonary
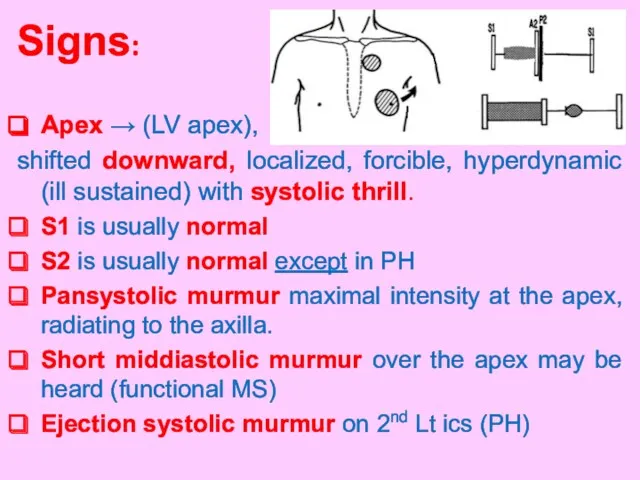
Signs:
Apex → (LV apex),
shifted downward, localized, forcible, hyperdynamic (ill sustained)
Signs:
Apex → (LV apex),
shifted downward, localized, forcible, hyperdynamic (ill sustained)
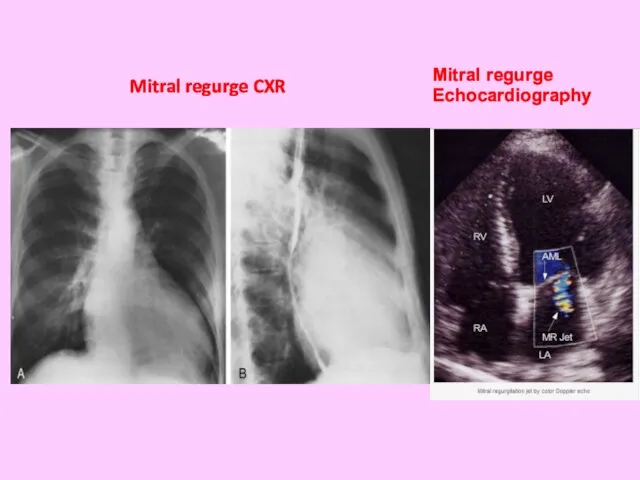
Mitral regurge CXR
Mitral regurge
Echocardiography
Mitral regurge CXR
Mitral regurge
Echocardiography

1- VSD:
-maximal intensity over the 3rd &
4th left intercostal
1- VSD:
-maximal intensity over the 3rd &
4th left intercostal
Prophylaxis
→ Against rheumatic recurrences (LONG ACTING PENECILLIN)
→ Against
Prophylaxis
→ Against rheumatic recurrences (LONG ACTING PENECILLIN)
→ Against
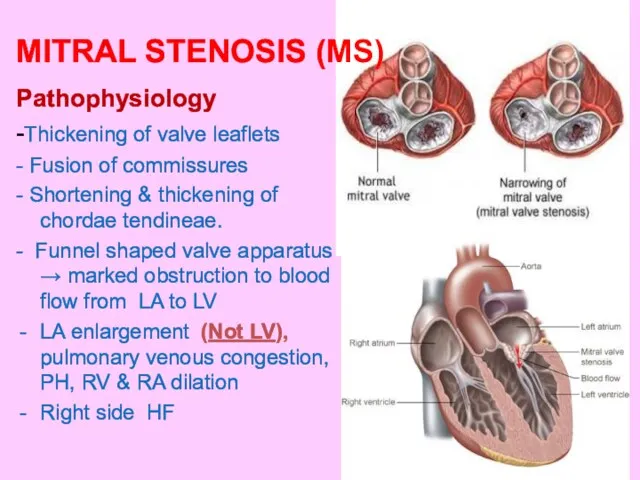
MITRAL STENOSIS (MS)
Pathophysiology
-Thickening of valve leaflets
- Fusion of commissures
- Shortening
MITRAL STENOSIS (MS)
Pathophysiology
-Thickening of valve leaflets
- Fusion of commissures
- Shortening

The clinical course depends
on the severity of MS.
Symptoms:
Dyspnea on exertion.
Orthopnea
The clinical course depends
on the severity of MS.
Symptoms:
Dyspnea on exertion.
Orthopnea
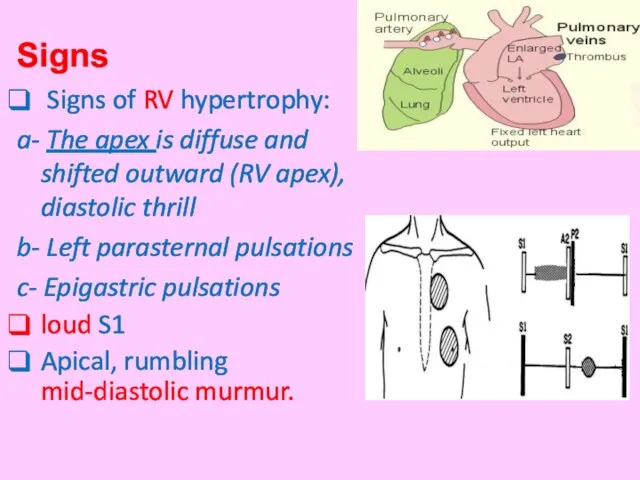
Signs
Signs of RV hypertrophy:
a- The apex is diffuse and shifted
Signs
Signs of RV hypertrophy:
a- The apex is diffuse and shifted
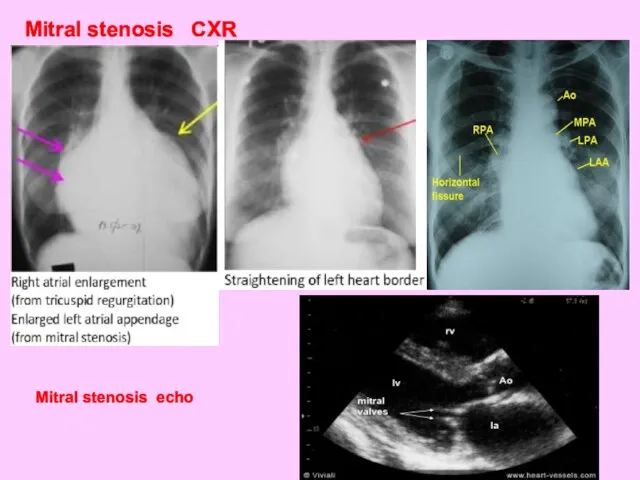
Mitral stenosis CXR
Mitral stenosis echo
Mitral stenosis CXR
Mitral stenosis echo
Mitral flow murmur (functional MS)
associated with large VSD, PDA,
Mitral flow murmur (functional MS)
associated with large VSD, PDA,
Prophylaxis
→ Against rheumatic recurrences (LONG ACTING PENECILLIN)
→ Against
Prophylaxis
→ Against rheumatic recurrences (LONG ACTING PENECILLIN)
→ Against
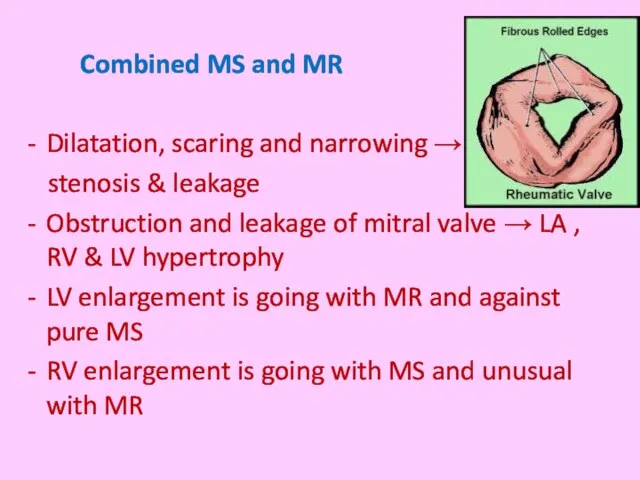
Combined MS and MR
Dilatation, scaring and narrowing →
stenosis
Combined MS and MR
Dilatation, scaring and narrowing →
stenosis
Which of the following pathological change occur in rheumatic mitral stenosis
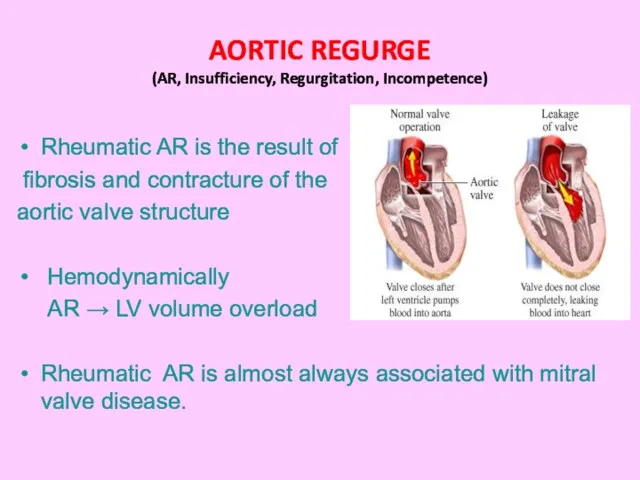
Rheumatic AR is the result of
fibrosis and contracture of the
Rheumatic AR is the result of
fibrosis and contracture of the
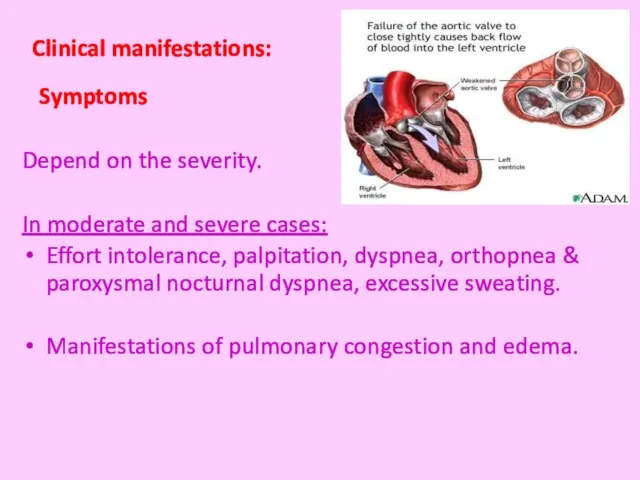
Symptoms
Depend on the severity.
In moderate and severe cases:
Effort intolerance, palpitation,
Symptoms
Depend on the severity.
In moderate and severe cases:
Effort intolerance, palpitation,
The rapid run off of the blood from aorta
during diastole
The rapid run off of the blood from aorta
during diastole

* Manifestations of LV enlargement.
The apex is shifted downword, forcible,
localized
The apex is shifted downword, forcible,
localized
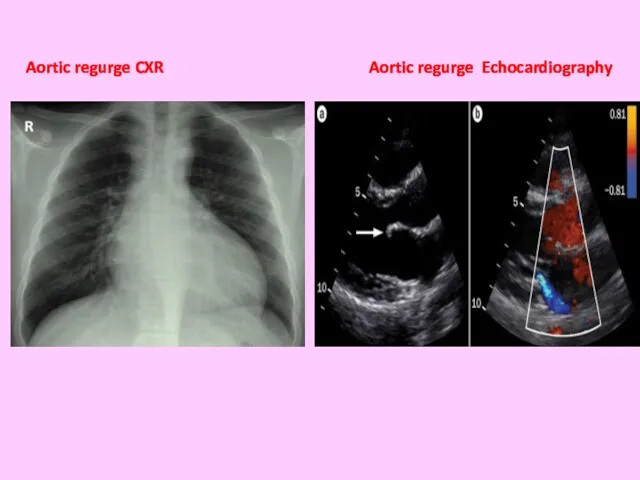
Aortic regurge CXR Aortic regurge Echocardiography
Aortic regurge CXR Aortic regurge Echocardiography
Prophylaxis
→ Against rheumatic recurrences (LONG ACTING PENECILLIN)
→ Against
Prophylaxis
→ Against rheumatic recurrences (LONG ACTING PENECILLIN)
→ Against
AORTIC STENOSIS
- Commissural adhesions occur slowly and progressive → narrowing and
AORTIC STENOSIS
- Commissural adhesions occur slowly and progressive → narrowing and
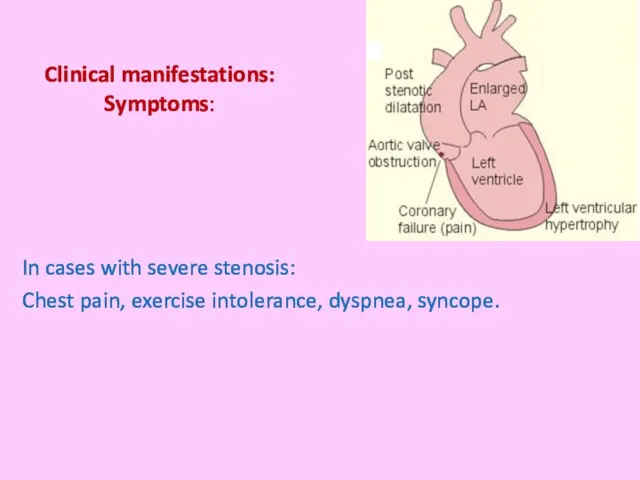
In cases with severe stenosis:
Chest pain, exercise intolerance, dyspnea, syncope.
Clinical manifestations:
In cases with severe stenosis:
Chest pain, exercise intolerance, dyspnea, syncope.
Clinical manifestations:
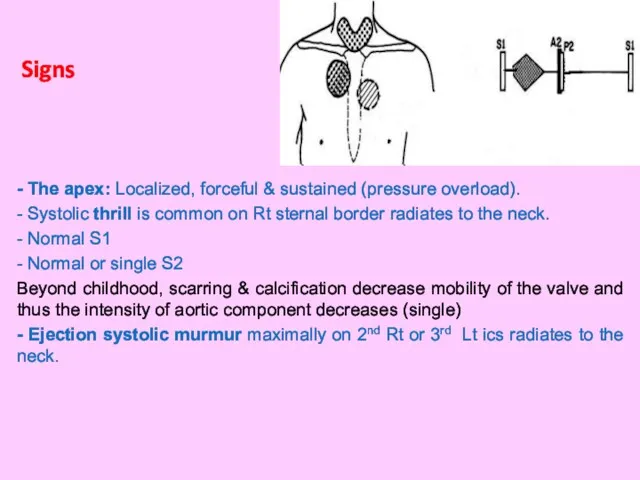
- The apex: Localized, forceful & sustained (pressure overload).
- Systolic thrill
- The apex: Localized, forceful & sustained (pressure overload).
- Systolic thrill
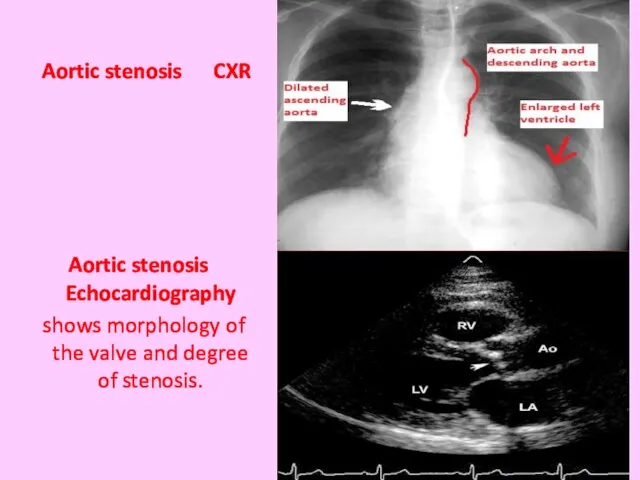
Aortic stenosis CXR
Aortic stenosis Echocardiography
shows morphology of
Aortic stenosis CXR
Aortic stenosis Echocardiography
shows morphology of
→ Against rheumatic recurrences (LONG ACTING PENECILLIN)
→ Against infective
→ Against rheumatic recurrences (LONG ACTING PENECILLIN)
→ Against infective
 Недоношенные дети: патология
Недоношенные дети: патология Алгоритм диагностики и оказания скорой помощи при гипертензивных кризах
Алгоритм диагностики и оказания скорой помощи при гипертензивных кризах Т-клеточное звено иммунитета. Субпопуляции Т-лимфоцитов. Регуляторная роль CD4-лимфоцитов. Иммунный ответ по Тх1 пути
Т-клеточное звено иммунитета. Субпопуляции Т-лимфоцитов. Регуляторная роль CD4-лимфоцитов. Иммунный ответ по Тх1 пути Катаральный мастит
Катаральный мастит Аномалии развития аноректальной области
Аномалии развития аноректальной области Нейропластичность и нейродегенерация
Нейропластичность и нейродегенерация Хроническая ишемия мозга
Хроническая ишемия мозга Средства, влияющие на систему крови
Средства, влияющие на систему крови Шок және коллапс
Шок және коллапс Регламент оператора горячей линии по вопросу covid-2019 (коронавирус)
Регламент оператора горячей линии по вопросу covid-2019 (коронавирус) Туберкулез животных
Туберкулез животных Ведение пожилых больных в поликлинике
Ведение пожилых больных в поликлинике Ортодонтическое лечение
Ортодонтическое лечение Медицинский осмотр студентов 3 курса
Медицинский осмотр студентов 3 курса Дифференциальный диагноз суставного синдрома
Дифференциальный диагноз суставного синдрома Анемия в искусстве…и в жизни
Анемия в искусстве…и в жизни Функция внешнего дыхания
Функция внешнего дыхания Микробиологические основы антимикробной терапии и профилактики
Микробиологические основы антимикробной терапии и профилактики Өкпе туберкулезі
Өкпе туберкулезі Опыт использования и интеграции в медицинском центре
Опыт использования и интеграции в медицинском центре Адаптация к мышечной деятельности
Адаптация к мышечной деятельности Арком. Междисциплинарное планирование и лечение в стоматологии
Арком. Междисциплинарное планирование и лечение в стоматологии Болезнь Паркинсона
Болезнь Паркинсона Современные представления о заболеваниях пародонта. Классификации заболеваний пародонта. Клиника. Диагностика
Современные представления о заболеваниях пародонта. Классификации заболеваний пародонта. Клиника. Диагностика Тістерді ағарту. Көрсеткіштері, заттары, әдістері
Тістерді ағарту. Көрсеткіштері, заттары, әдістері Сбалансированное питание
Сбалансированное питание Фармацевтическая опека при травматических и инфекционных повреждениях кожи
Фармацевтическая опека при травматических и инфекционных повреждениях кожи Экстрапирамдалық жүйе аурулары
Экстрапирамдалық жүйе аурулары