- Diverticular Disease of the Colon

Содержание
- 2. Nomenclature Diverticulum = sac-like protrusion of the colonic wall Diverticulosis = describes the presence of diverticuli
- 3. Epidemiology Increases with age Age 40 Age 60 30% Age 85 65%
- 4. Epidemiology Gender prevalence depends on age M>>F Age less than 40 M > F Age 40-50
- 5. Anatomic location of diverticuli varies with the geographic location “Westernized” nations (North America, Europe, Australia) have
- 6. Anatomic location of diverticuli varies with the geographic location Asia and Africa diverticulosis in general is
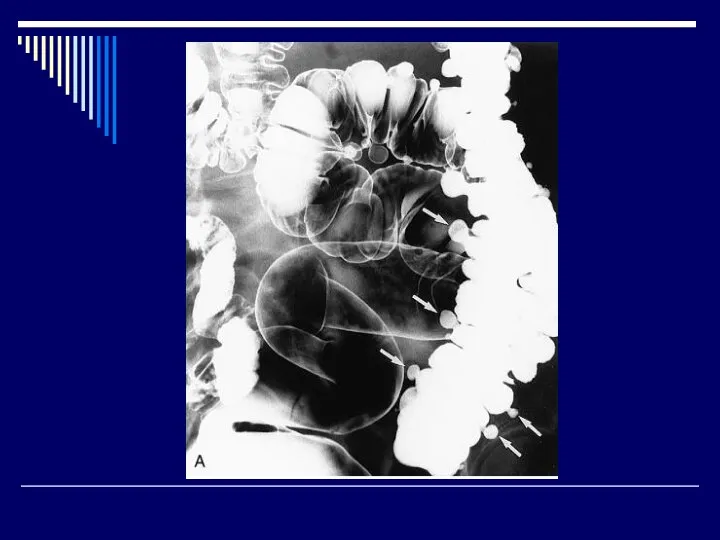
- 7. What exactly is a diverticulum? True diverticulum contains all layers of the GI wall (mucosa to
- 8. Pathophysiology Diverticuli develop in ‘weak’ regions of the colon. Specifically, local hernias develop where the vasa
- 9. Mucosa Submucosa Muscularis Serosa Vasa recta
- 10. Lifestyle factors associated with diverticular disease Low fiber ? diverticular disease Not absolutely proven in all
- 11. Lifestyle factors associated with diverticular disease Obesity associated with diverticulosis – particularly in men under the
- 13. Uncomplicated diverticulosis Usually an incidental finding at time of colonoscopy
- 16. Uncomplicated diverticulosis Considered ‘asymptomatic’ However, a significant minority of patients will complain of cramping, bloating, irregular
- 17. Uncomplicated diverticulosis Treatment: Fiber Bulk content reduces colonic pressure preventing underlying pathophysiology that lead to diverticulosis
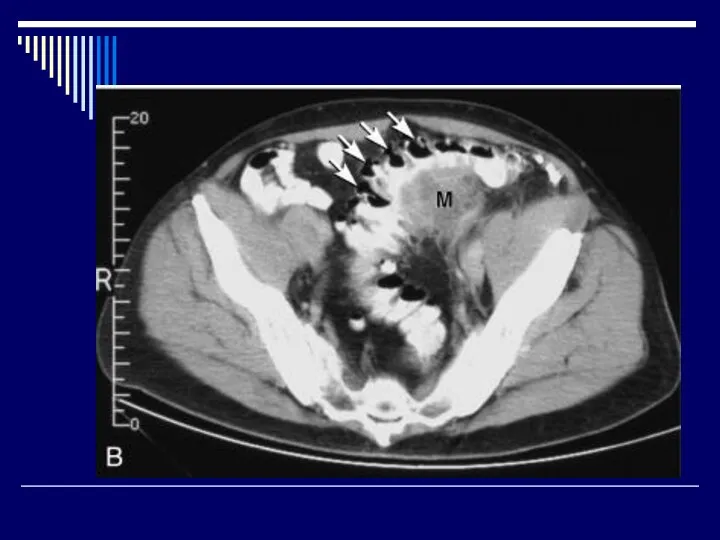
- 18. Diverticulitis Diverticulitis = inflammation of diverticuli Most common complication of diverticulosis Occurs in 10-25% of patients
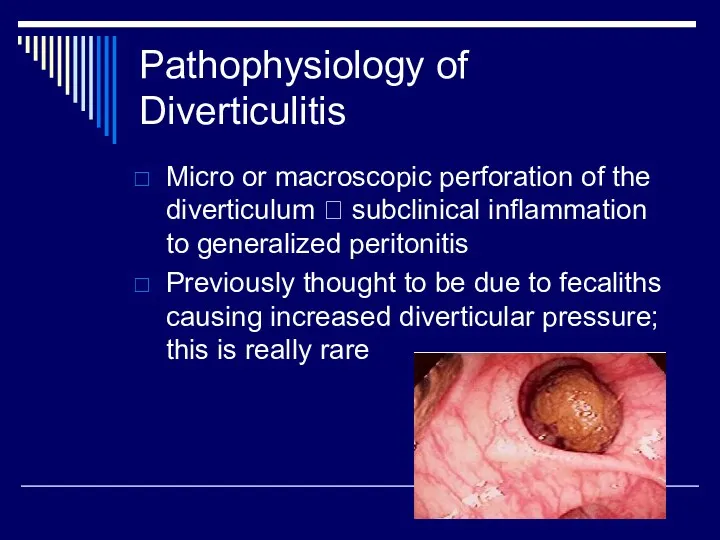
- 19. Pathophysiology of Diverticulitis Micro or macroscopic perforation of the diverticulum ? subclinical inflammation to generalized peritonitis
- 20. Pathophysiology of Diverticulitis Erosion of diverticular wall from increased intraluminal pressure ? inflammation ? focal necrosis
- 21. Diagnosis of Diverticulitis Classic history: increasing, constant, LLQ abdominal pain over several days prior to presentation
- 22. Diagnosis of Diverticulitis Previous of episodes of similar pain Associated symptoms Nausea/vomiting 20-62% Constipation 50% Diarrhea
- 23. Diagnosis of Diverticulitis Right sided diverticulitis tends to cause RLQ abdominal pain; can be difficult to
- 24. Diagnosis of Diverticulitis Physical examination Low grade fever LLQ abdominal tenderness Usually moderate with no peritoneal
- 25. Diagnosis of Diverticulitis Clinically, diagnosis can be made with typical history and examination Radiographic confirmation is
- 27. Treatment of Diverticulitis Complicated diverticulitis = Presence of macroperforation, obstruction, abscess, or fistula Uncomplicated diverticulitis =
- 28. Uncomplicated diverticulitis Bowel rest or restriction Clear liquids or NPO for 2-3 days Then advance diet
- 29. Uncomplicated diverticulitis Antibiotics Coverage of fecal flora Gram negative rods, anaerobes Common regimens Cipro + Flagyl
- 30. Uncomplicated diverticulitis Monitoring clinical course Pain should gradually improve several days (decrescendo) Normalization of temperature Tolerance
- 31. Uncomplicated diverticulitis After resolution of attack ? high fiber diet with supplemental fiber
- 32. Uncomplicated diverticulitis Follow-up: Colonoscopy in 4-6 weeks Purpose Exclude neoplasm Evaluate extent of the diverticulosis
- 33. Prognosis after resolution 30-40% of patients will remain asymptomatic 30-40% of pts will have episodic abdominal
- 34. Prognosis after resolution Second attack Risk of recurrent attacks is high (>50%) Some studies suggest a
- 35. Prognosis after resolution Some argue in the elderly recurrent attacks can be managed with medications Some
- 36. Complicated Diverticulitis Peritonitis Resuscitation Antibiotics Ampicillin + Gentamycin + Metronidazole Imipenem/cilastin Emergency exploration Mortality 6% purulent
- 37. Complicated Diverticulitis: Abscess Occurs in 16% of patients with acute diverticulitis Percutaneous drainage followed by single
- 38. Complicated Diverticulitis: Abscess Small abscesses too small to drain percutaneously ( These pts behave like uncomplicated
- 39. Complicated Diverticulitis: Fistulas Occurs in up to 80% of cases requiring surgery Major types Colovesical fistula
- 40. Complicated Diverticulitis: Fistulas - Symptoms Passage of gas and stool from the affected organ Colovesical fistula:
- 41. Complicated Diverticulitis: Fistulas Diagnosis CT: thickened bladder with associated colonic diverticuli adjacent and air in the
- 42. Complicated Diverticulitis: Treatment of Fistulas Surgery Resection of affected colon (origin of the fistula) Fistula tract
- 43. Surgical Treatment of Diverticulitis Elective single stage resection is ideal, ~6 weeks after episode Two stage
- 44. Diverticular bleeding Most common cause of brisk hematochezia (30-50% of cases) 15% of patients with diverticulosis
- 45. Diverticular bleeding Patients requiring less than 4 units of PRBC/ day ? 99% will stop bleeding
- 46. Diverticular bleeding: Localization Right colon is the source of diverticular bleeding in 50-90% of patients Possible
- 47. Diverticular bleeding: Localization Colonoscopy after rapid prep Can localize site of bleeding Offers possible therapeutic intervention
- 48. Diverticular bleeding: Localization Tagged red blood cell scan Can localize bleeding source 97% sensitivity 83% specificity
- 50. Скачать презентацию
Nomenclature
Diverticulum = sac-like protrusion of the colonic wall
Diverticulosis = describes the
Nomenclature
Diverticulum = sac-like protrusion of the colonic wall
Diverticulosis = describes the
Epidemiology
Increases with age
Age 40 <5%
Age 60 30%
Age 85 65%
Epidemiology
Increases with age
Age 40 <5%
Age 60 30%
Age 85 65%
Epidemiology
Gender prevalence depends on age
M>>F Age less than 40
M > F Age 40-50
F
Epidemiology
Gender prevalence depends on age
M>>F Age less than 40
M > F Age 40-50
F
Anatomic location of diverticuli varies with the geographic location
“Westernized” nations (North
Anatomic location of diverticuli varies with the geographic location
“Westernized” nations (North
Anatomic location of diverticuli varies with the geographic location
Asia and Africa
Anatomic location of diverticuli varies with the geographic location
Asia and Africa
What exactly is a diverticulum?
True diverticulum contains all layers of the
What exactly is a diverticulum?
True diverticulum contains all layers of the
Pathophysiology
Diverticuli develop in ‘weak’ regions of the colon. Specifically, local hernias
Pathophysiology
Diverticuli develop in ‘weak’ regions of the colon. Specifically, local hernias
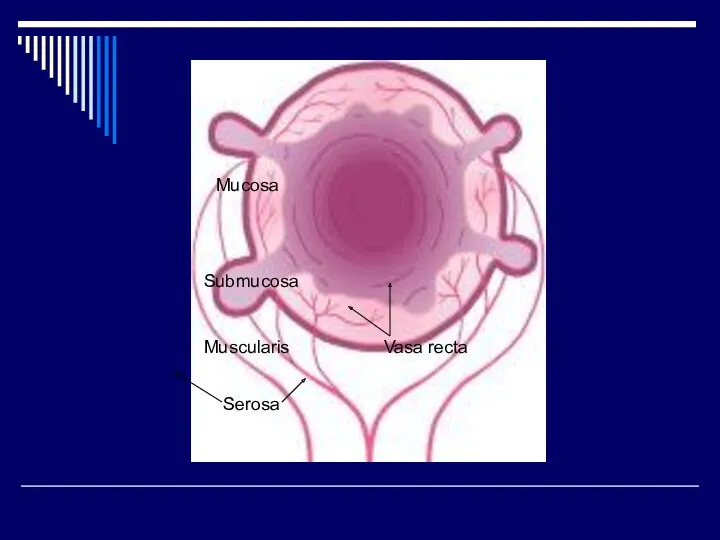
Mucosa
Submucosa
Muscularis
Serosa
Vasa recta
Mucosa
Submucosa
Muscularis
Serosa
Vasa recta
Lifestyle factors associated with diverticular disease
Low fiber ? diverticular disease
Not absolutely
Lifestyle factors associated with diverticular disease
Low fiber ? diverticular disease
Not absolutely
Lifestyle factors associated with diverticular disease
Obesity associated with diverticulosis – particularly
Lifestyle factors associated with diverticular disease
Obesity associated with diverticulosis – particularly
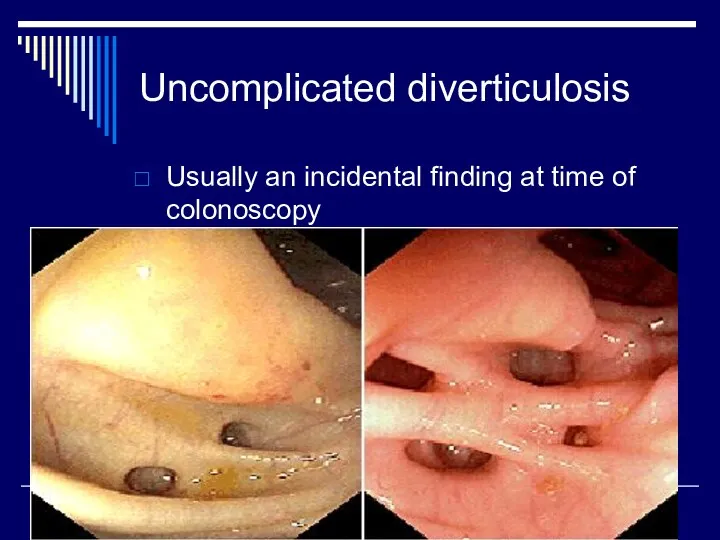
Uncomplicated diverticulosis
Usually an incidental finding at time of colonoscopy
Uncomplicated diverticulosis
Usually an incidental finding at time of colonoscopy
Uncomplicated diverticulosis
Considered ‘asymptomatic’
However, a significant minority of patients will complain
Uncomplicated diverticulosis
Considered ‘asymptomatic’
However, a significant minority of patients will complain
Uncomplicated diverticulosis
Treatment: Fiber
Bulk content reduces colonic pressure preventing underlying pathophysiology that
Uncomplicated diverticulosis
Treatment: Fiber
Bulk content reduces colonic pressure preventing underlying pathophysiology that
Diverticulitis
Diverticulitis = inflammation of diverticuli
Most common complication of diverticulosis
Occurs in 10-25%
Diverticulitis
Diverticulitis = inflammation of diverticuli
Most common complication of diverticulosis
Occurs in 10-25%
Pathophysiology of Diverticulitis
Micro or macroscopic perforation of the diverticulum ? subclinical
Pathophysiology of Diverticulitis
Micro or macroscopic perforation of the diverticulum ? subclinical
Pathophysiology of Diverticulitis
Erosion of diverticular wall from increased intraluminal pressure ?
Pathophysiology of Diverticulitis
Erosion of diverticular wall from increased intraluminal pressure ?
Diagnosis of Diverticulitis
Classic history: increasing, constant, LLQ abdominal pain over several
Diagnosis of Diverticulitis
Classic history: increasing, constant, LLQ abdominal pain over several
Diagnosis of Diverticulitis
Previous of episodes of similar pain
Associated symptoms
Nausea/vomiting 20-62%
Constipation 50%
Diarrhea 25-35%
Urinary
Diagnosis of Diverticulitis
Previous of episodes of similar pain
Associated symptoms
Nausea/vomiting 20-62%
Constipation 50%
Diarrhea 25-35%
Urinary
Diagnosis of Diverticulitis
Right sided diverticulitis tends to cause RLQ abdominal pain;
Diagnosis of Diverticulitis
Right sided diverticulitis tends to cause RLQ abdominal pain;
Diagnosis of Diverticulitis
Physical examination
Low grade fever
LLQ abdominal tenderness
Usually moderate with no
Diagnosis of Diverticulitis
Physical examination
Low grade fever
LLQ abdominal tenderness
Usually moderate with no
Diagnosis of Diverticulitis
Clinically, diagnosis can be made with typical history and
Diagnosis of Diverticulitis
Clinically, diagnosis can be made with typical history and

Treatment of Diverticulitis
Complicated diverticulitis = Presence of macroperforation, obstruction, abscess, or
Treatment of Diverticulitis
Complicated diverticulitis = Presence of macroperforation, obstruction, abscess, or
Uncomplicated diverticulitis
Bowel rest or restriction
Clear liquids or NPO for 2-3 days
Uncomplicated diverticulitis
Bowel rest or restriction
Clear liquids or NPO for 2-3 days
Uncomplicated diverticulitis
Antibiotics
Coverage of fecal flora
Gram negative rods, anaerobes
Common regimens
Cipro +
Uncomplicated diverticulitis
Antibiotics
Coverage of fecal flora
Gram negative rods, anaerobes
Common regimens
Cipro +
Uncomplicated diverticulitis
Monitoring clinical course
Pain should gradually improve several days (decrescendo)
Normalization of
Uncomplicated diverticulitis
Monitoring clinical course
Pain should gradually improve several days (decrescendo)
Normalization of
Uncomplicated diverticulitis
After resolution of attack ? high fiber diet with supplemental
Uncomplicated diverticulitis
After resolution of attack ? high fiber diet with supplemental
Uncomplicated diverticulitis
Follow-up: Colonoscopy in 4-6 weeks
Purpose
Exclude neoplasm
Evaluate extent of the diverticulosis
Uncomplicated diverticulitis
Follow-up: Colonoscopy in 4-6 weeks
Purpose
Exclude neoplasm
Evaluate extent of the diverticulosis
Prognosis after resolution
30-40% of patients will remain asymptomatic
30-40% of pts will
Prognosis after resolution
30-40% of patients will remain asymptomatic
30-40% of pts will
Prognosis after resolution
Second attack
Risk of recurrent attacks is high (>50%)
Some studies
Prognosis after resolution
Second attack
Risk of recurrent attacks is high (>50%)
Some studies
Prognosis after resolution
Some argue in the elderly recurrent attacks can be
Prognosis after resolution
Some argue in the elderly recurrent attacks can be
Complicated Diverticulitis
Peritonitis
Resuscitation
Antibiotics
Ampicillin + Gentamycin + Metronidazole
Imipenem/cilastin
Emergency exploration
Mortality 6% purulent peritonitis and
Complicated Diverticulitis
Peritonitis
Resuscitation
Antibiotics
Ampicillin + Gentamycin + Metronidazole
Imipenem/cilastin
Emergency exploration
Mortality 6% purulent peritonitis and
Complicated Diverticulitis: Abscess
Occurs in 16% of patients with acute diverticulitis
Percutaneous drainage
Complicated Diverticulitis: Abscess
Occurs in 16% of patients with acute diverticulitis
Percutaneous drainage
Complicated Diverticulitis: Abscess
Small abscesses too small to drain percutaneously (< 1cm)
Complicated Diverticulitis: Abscess
Small abscesses too small to drain percutaneously (< 1cm)
Complicated Diverticulitis: Fistulas
Occurs in up to 80% of cases requiring surgery
Major
Complicated Diverticulitis: Fistulas
Occurs in up to 80% of cases requiring surgery
Major
Complicated Diverticulitis: Fistulas - Symptoms
Passage of gas and stool from the
Complicated Diverticulitis: Fistulas - Symptoms
Passage of gas and stool from the
Complicated Diverticulitis: Fistulas
Diagnosis
CT: thickened bladder with associated colonic diverticuli adjacent and
Complicated Diverticulitis: Fistulas
Diagnosis
CT: thickened bladder with associated colonic diverticuli adjacent and
Complicated Diverticulitis: Treatment of Fistulas
Surgery
Resection of affected colon (origin of
Complicated Diverticulitis: Treatment of Fistulas
Surgery
Resection of affected colon (origin of
Surgical Treatment of Diverticulitis
Elective single stage resection is ideal, ~6 weeks
Surgical Treatment of Diverticulitis
Elective single stage resection is ideal, ~6 weeks
Diverticular bleeding
Most common cause of brisk hematochezia (30-50% of cases)
15% of
Diverticular bleeding
Most common cause of brisk hematochezia (30-50% of cases)
15% of
Diverticular bleeding
Patients requiring less than 4 units of PRBC/ day ?
Diverticular bleeding
Patients requiring less than 4 units of PRBC/ day ?
Diverticular bleeding: Localization
Right colon is the source of diverticular bleeding in
Diverticular bleeding: Localization
Right colon is the source of diverticular bleeding in
Diverticular bleeding:
Localization
Colonoscopy after rapid prep
Can localize site of bleeding
Offers possible therapeutic
Diverticular bleeding:
Localization
Colonoscopy after rapid prep
Can localize site of bleeding
Offers possible therapeutic
Diverticular bleeding: Localization
Tagged red blood cell scan
Can localize bleeding source
97%
Diverticular bleeding: Localization
Tagged red blood cell scan
Can localize bleeding source
97%
 Брюшной тиф
Брюшной тиф Сестринский уход за стомированным пациентом. Лекция №11
Сестринский уход за стомированным пациентом. Лекция №11 Обмен веществ
Обмен веществ Анатомия лицевого нерва
Анатомия лицевого нерва Спинальные амиотрофии
Спинальные амиотрофии Компенсаторно - приспособительные процессы
Компенсаторно - приспособительные процессы Артериальная гипертензия. Что нового в рекомендациях?
Артериальная гипертензия. Что нового в рекомендациях? Аорта аневризмасының ыдырауы
Аорта аневризмасының ыдырауы Принципы препарирования 1,2 класса по Блэку
Принципы препарирования 1,2 класса по Блэку Цена и ценовая политика. Ценообразование на лекарственные средства
Цена и ценовая политика. Ценообразование на лекарственные средства Порядок выдачи и оформления листков нетрудоспособности
Порядок выдачи и оформления листков нетрудоспособности Захворювання носа та приносових пазух
Захворювання носа та приносових пазух Применение ультразвука в анестезиологии и реаниматологии
Применение ультразвука в анестезиологии и реаниматологии Лечение гриппа
Лечение гриппа Гипотиреоз
Гипотиреоз Туберкулинодиагностика
Туберкулинодиагностика Местные анестетики
Местные анестетики История болезни
История болезни Исследовательская работа “Вегетарианство-основа здорового образа жизни”
Исследовательская работа “Вегетарианство-основа здорового образа жизни” Балалардың церебральды салдануы
Балалардың церебральды салдануы Хирургическая анатомия головы. Основные принципы оперативных вмешательств на голове
Хирургическая анатомия головы. Основные принципы оперативных вмешательств на голове Діагностика та лікування дифтерії у дітей
Діагностика та лікування дифтерії у дітей Общие вопросы наркологии
Общие вопросы наркологии Антигендер жалпы сипаттамасы
Антигендер жалпы сипаттамасы Вибрационная болезнь
Вибрационная болезнь Захворювання органів травневого каналу в дітей старшого віку. Хоцистохолангіт та дисфункція жовчовивідних шляхів. Коліт
Захворювання органів травневого каналу в дітей старшого віку. Хоцистохолангіт та дисфункція жовчовивідних шляхів. Коліт Неспецифические воспалительные заболевания мочеполовой системы
Неспецифические воспалительные заболевания мочеполовой системы Ветряная оспа
Ветряная оспа