- Healthcare models in world practice

Содержание
- 2. THE UNIVERSAL DECLARATION OF HUMAN RIGHTS The General Assembly of the United Nations adopted and proclaimed
- 3. DIFFERENT HEALTHCARE MODELS Each nation’s health care system is a reflection of its: History Politics Economy
- 4. 1. THE BISMARCK MODEL Germany, Japan, France, Belgium, Switzerland, Japan, and Latin America Named for Prussian
- 5. 2. THE BEVERIDGE MODEL Named after William Beveridge – inspired Britain’s NHS Great Britain, Italy, Spain,
- 6. 3. THE NATIONAL HEALTH INSURANCE MODEL Canada, Taiwan, South Korea Characteristics: Providers are private Payer is
- 7. 4. THE OUT-OF-POCKET MODEL Rural regions of Africa, India, China, and South America “non-system” countries Characteristics:
- 8. The main features of world Insurance medicine are: a membership of Health Care; an equal by
- 9. GREAT BRITAIN Insured - 100% of population insured Spending - 7.5% of GDP Funding: Single payer
- 10. GREAT BRITAIN Physician Choice Patients have very little provider choice Copayment/Deductibles No deductibles Almost no copayments
- 11. CANADA Insured Single payer system – 100% insured Each province must make insurance: Universal (available to
- 12. CANADA Spending - 9% of GDP Private Insurance At one time all private insurance was prohibited;
- 13. CANADA Physician Choice Referrals are required for all specialist services except the ED Copayment/Deductibles Generally no
- 14. FRANCE Insured - About 99% of population covered Cost - 3rd most expensive health care system
- 15. FRANCE Physician Compensation Providers paid by national health insurance system based on a centrally planned fee
- 16. FRANCE Physician Choice Fair amount of choice in the doctors they choose Copayment/Deductible 10% to 40%
- 17. GERMANY Insured - 99.6% of population – sickness funds Those with higher incomes can buy private
- 18. GERMANY Private insurance 9% of Germans have supplemental insurance; covers items not paid for by the
- 19. GERMANY Technology Low technology compared to U.S. Waiting Times WHO reported that “waiting lists and explicit
- 20. JAPAN Insured Universal health insurance based around a mandatory, employment-based insurance “The Employee Health Insurance Program”
- 21. JAPAN Funding -8.5% (large business) or an 8.2% (small business) payroll tax Payroll taxes are split
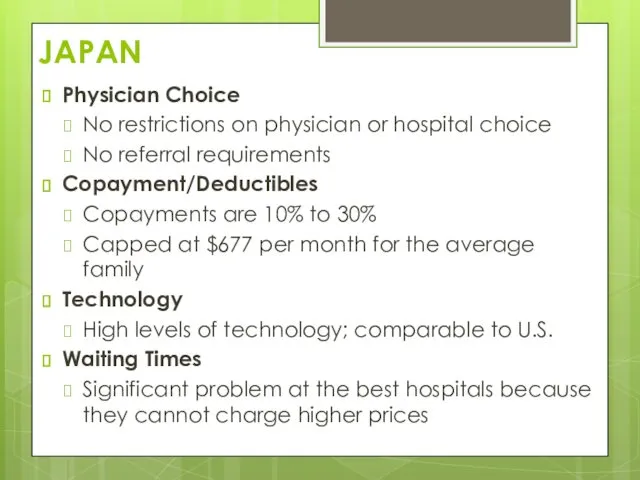
- 22. JAPAN Physician Choice No restrictions on physician or hospital choice No referral requirements Copayment/Deductibles Copayments are
- 24. Comparison of Global Healthcare by Rand Corporation
- 25. UNIVERSAL LAWS OF HEALTHCARE SYSTEMS No matter how good the healthcare in a particular country people
- 26. 5 MYTHS ABOUT HEALTH CARE AROUND THE WORLD It’s all socialized medicine out there Many countries
- 27. “Life is not about waiting for the storms to pass…it’s about learning to dance in the
- 29. Скачать презентацию
THE UNIVERSAL DECLARATION OF HUMAN RIGHTS
The General Assembly of the United
THE UNIVERSAL DECLARATION OF HUMAN RIGHTS
The General Assembly of the United
DIFFERENT HEALTHCARE MODELS
Each nation’s health care system is a reflection of
DIFFERENT HEALTHCARE MODELS
Each nation’s health care system is a reflection of
1. THE BISMARCK MODEL
Germany, Japan, France, Belgium, Switzerland, Japan, and Latin
1. THE BISMARCK MODEL
Germany, Japan, France, Belgium, Switzerland, Japan, and Latin
2. THE BEVERIDGE MODEL
Named after William Beveridge – inspired Britain’s NHS
Great
2. THE BEVERIDGE MODEL
Named after William Beveridge – inspired Britain’s NHS
Great
3. THE NATIONAL HEALTH
INSURANCE MODEL
Canada, Taiwan, South Korea
Characteristics:
Providers are private
Payer
3. THE NATIONAL HEALTH
INSURANCE MODEL
Canada, Taiwan, South Korea
Characteristics:
Providers are private
Payer
4. THE OUT-OF-POCKET MODEL
Rural regions of Africa, India, China, and South
4. THE OUT-OF-POCKET MODEL
Rural regions of Africa, India, China, and South

The main features of world Insurance medicine are:
a membership of
The main features of world Insurance medicine are:
a membership of

GREAT BRITAIN
Insured - 100% of population insured
Spending - 7.5% of GDP
Funding:
Single
GREAT BRITAIN
Insured - 100% of population insured
Spending - 7.5% of GDP
Funding:
Single
GREAT BRITAIN
Physician Choice
Patients have very little provider choice
Copayment/Deductibles
No deductibles
Almost no
GREAT BRITAIN
Physician Choice
Patients have very little provider choice
Copayment/Deductibles
No deductibles
Almost no
CANADA
Insured
Single payer system – 100% insured
Each province must make insurance:
Universal (available
CANADA
Insured
Single payer system – 100% insured
Each province must make insurance:
Universal (available
CANADA
Spending - 9% of GDP
Private Insurance
At one time all private insurance
CANADA
Spending - 9% of GDP
Private Insurance
At one time all private insurance
CANADA
Physician Choice
Referrals are required for all specialist services except the ED
Copayment/Deductibles
Generally
CANADA
Physician Choice
Referrals are required for all specialist services except the ED
Copayment/Deductibles
Generally
FRANCE
Insured - About 99% of population covered
Cost - 3rd most expensive
FRANCE
Insured - About 99% of population covered
Cost - 3rd most expensive
FRANCE
Physician Compensation
Providers paid by national health insurance system based on a
FRANCE
Physician Compensation
Providers paid by national health insurance system based on a
FRANCE
Physician Choice
Fair amount of choice in the doctors they choose
Copayment/Deductible
10% to
FRANCE
Physician Choice
Fair amount of choice in the doctors they choose
Copayment/Deductible
10% to
GERMANY
Insured - 99.6% of population – sickness funds
Those with higher incomes
GERMANY
Insured - 99.6% of population – sickness funds
Those with higher incomes

GERMANY
Private insurance
9% of Germans have supplemental insurance; covers items not paid
GERMANY
Private insurance
9% of Germans have supplemental insurance; covers items not paid

GERMANY
Technology
Low technology compared to U.S.
Waiting Times
WHO reported that “waiting lists
GERMANY
Technology
Low technology compared to U.S.
Waiting Times
WHO reported that “waiting lists
JAPAN
Insured
Universal health insurance based around a mandatory, employment-based insurance
“The Employee Health
JAPAN
Insured
Universal health insurance based around a mandatory, employment-based insurance
“The Employee Health
JAPAN
Funding -8.5% (large business) or an 8.2% (small business) payroll tax
Payroll
JAPAN
Funding -8.5% (large business) or an 8.2% (small business) payroll tax
Payroll
JAPAN
Physician Choice
No restrictions on physician or hospital choice
No referral requirements
Copayment/Deductibles
Copayments are
JAPAN
Physician Choice
No restrictions on physician or hospital choice
No referral requirements
Copayment/Deductibles
Copayments are
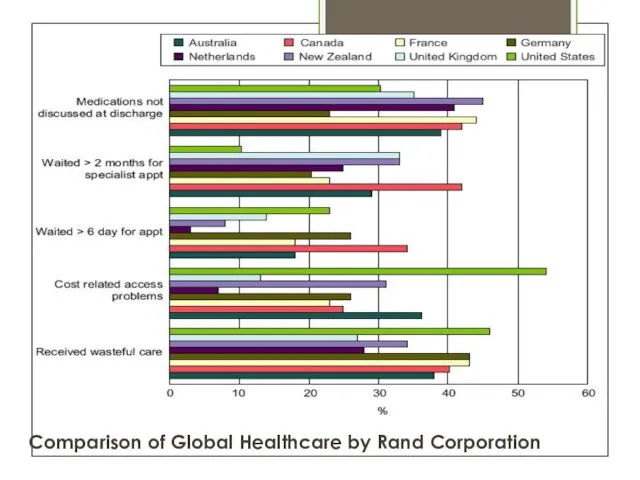
Comparison of Global Healthcare by Rand Corporation
Comparison of Global Healthcare by Rand Corporation
UNIVERSAL LAWS OF HEALTHCARE SYSTEMS
No matter how good the healthcare in
UNIVERSAL LAWS OF HEALTHCARE SYSTEMS
No matter how good the healthcare in
5 MYTHS ABOUT HEALTH CARE
AROUND THE WORLD
It’s all socialized medicine out
5 MYTHS ABOUT HEALTH CARE
AROUND THE WORLD
It’s all socialized medicine out
“Life is not about waiting for the storms to pass…it’s about
“Life is not about waiting for the storms to pass…it’s about
 Этические проблемы генной инженерии
Этические проблемы генной инженерии Виды прикусов
Виды прикусов Гастроэнтерологиядағы стандартты диагностикалау және емдеу әдістері
Гастроэнтерологиядағы стандартты диагностикалау және емдеу әдістері Шаншуға арналған дәрілік препараттар
Шаншуға арналған дәрілік препараттар Неврологический осмотр больного в коматозном состоянии
Неврологический осмотр больного в коматозном состоянии Бронхиальная астма
Бронхиальная астма ЭКСПЕРТИЗА ПРОФПРИГОДНОСТИ
ЭКСПЕРТИЗА ПРОФПРИГОДНОСТИ Реабилизация неврологических больных
Реабилизация неврологических больных Кандидоз слизистой оболочки полости рта
Кандидоз слизистой оболочки полости рта Endocrine system
Endocrine system Вступ до фармацевтичної біоетики
Вступ до фармацевтичної біоетики Патогенез лейкозов
Патогенез лейкозов Послеродовый период. Уход за родильницей
Послеродовый период. Уход за родильницей Тіндердің шығу тегі мен дамуының заңдылықтары. Тіндердің жіктелуі. Жүйе түзетін факторлар және оның тіндердің тұрақтылығын
Тіндердің шығу тегі мен дамуының заңдылықтары. Тіндердің жіктелуі. Жүйе түзетін факторлар және оның тіндердің тұрақтылығын Задержка роста (внутриутробного развития) плода
Задержка роста (внутриутробного развития) плода Определение центрального соотношения челюстей при полном отсутствии зубов
Определение центрального соотношения челюстей при полном отсутствии зубов Влияние алкоголя на организм человека
Влияние алкоголя на организм человека Правила обработки рук в соответствии с СанПиН. Методы и средства
Правила обработки рук в соответствии с СанПиН. Методы и средства Ультразвуковая диагностика заболеваний органов мошонки
Ультразвуковая диагностика заболеваний органов мошонки Дәрігерлік деонтология, семиология
Дәрігерлік деонтология, семиология Артериальная гипертензия
Артериальная гипертензия СПИД-ассоцированные инфекции. Хронические неинфекционные заболевания при ВИЧ-инфекции
СПИД-ассоцированные инфекции. Хронические неинфекционные заболевания при ВИЧ-инфекции Дитяче зубне протезування
Дитяче зубне протезування Заболевания суставов
Заболевания суставов Повреждение костей предплечья
Повреждение костей предплечья Растворы для обеспечения инфекционной безопасности
Растворы для обеспечения инфекционной безопасности Патофизиология сердечной недостаточности
Патофизиология сердечной недостаточности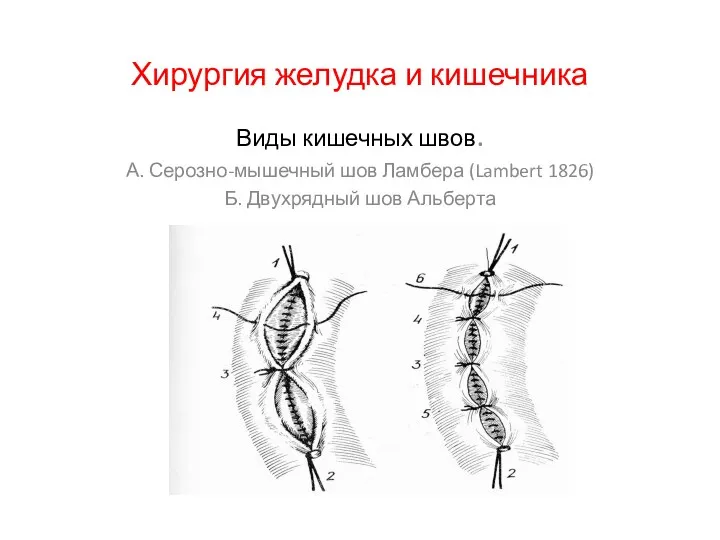 Хирургия желудка и кишечника
Хирургия желудка и кишечника