- Obsessive-Compulsive Disorder

Содержание
- 2. Why Discuss OCD? Underdiagnosed (4th most common psychiatric diagnosis) More common than previously recognized (mental compulsions
- 3. Why is OCD Underdiagnosed? Symptoms are embarrassing Lack of insight into problems with the illness Average
- 4. OCD – a secretive disorder 62% - ignorance of illness 35% - fear to be considered
- 5. The Problem... The average patient does not receive appropriate treatment for 17 years after OCD diagnosed!!!
- 6. Epidemiology Lifetime prevalence 2-3% U.S.A. 5-7 million adults 1 million kids Mean age of onset 20
- 7. Etiology Genetic factors Biologic factors Behavioral theory Psychodynamic theory
- 8. Genetic Factors Inheritance most evident in childhood onset OCD 10% of 1st degree relatives of OCD
- 9. Neuroanatomy: striatal disorders Tourette’s syndrome Sydenham’s chorea Huntington’s disease Parkinson’s disease Encephalitis Economo
- 10. OCD: brain disorder (Cortico-striatal-thalamo-cortical circuit) Neurological soft signs Evoked potentials Prepulse inhibition Executive function TMS Conclusion:
- 11. OCD: brain disorder Frontal lobe basal ganglia anterior/posterior cingulate PET scan: > metabolic activity in: -
- 14. Neurochemistry: 5HT system Neurotransmitter dysregulation Serotonin - SRI drugs work - > CSF 5-HIAA suggests higher
- 15. Neurochemistry: dopamine Dopamine agonists – induced OCD (cocaine, methylphenidate) Dopamine antagonists – effective in some types
- 16. Neurochemistry: other than 5HT/DA systems Glutamate Neuropeptides Gonadal steroids Second/third messengers (protein kinase C) Opiates
- 17. Diagnosis (DSM-5) Must have either obsessions or compulsions Obsessions - increase anxiety Compulsions - decrease anxiety
- 18. Diagnosis (cont.) Compulsions: - repetitive behaviors or thoughts - patient feels compelled to perform to reduce
- 19. Diagnosis (cont.) Patient realizes that the obsessions and compulsions are excessive and unreasonable Obsessions and compulsions:
- 20. Clinical Presentation OCD patients often first seen by clinician other than psychiatrist/psychologist 75-85% have both obsessions
- 21. Clinical Presentation (cont.) 50-75% onset after stressful event (ex., move/ new school story) Chronic course –
- 22. Contamination Obsession (cont.) Lengthy shower Family collusion (father/garage)
- 23. Pathological Doubt Obsession How many times do you check your locked door, or the coffee pot?
- 24. Pathological Doubt Cases Front door checking/staring (20 min.) Jack Nicholson (door) in “As Good as It
- 25. Aggressive Thoughts Obsession Religious theme suggests harsh, punitive superego Urge to shout obscenities in church Sexual
- 26. Obsession about Symmetry/Precision Compulsive ritual involves slow and meticulous behavior Jack Nicholson avoiding sidewalk cracks Shaving
- 27. Other Presentations Touching Religious obsessions (hypermorality) Pathological fear of voiding in public (planning and searching for
- 28. Rituals vs Compulsions Rituals Compulsions Calming Suffering Socializing function Aggravation of anxiety
- 29. OCD dimensions Symmetry / ordering, counting, repeating Hoarding obsessions / compulsions Contamination obsessions / cleaning rituals
- 30. OCD dimensions Stability over time Differential treatment response Neural correlates Possible differential genetic underprint
- 31. Early-onset OCD Anger attacks Continuous compulsive questions “Mom, you won’t due tonight?” Tyrannical orders :”Mom, give
- 32. Neural Correlates Striatal/thalamic I. Checking compulsions / sexual, aggressive obsessions II. Symmetry obsessions / ordering, repeating,
- 33. Differential Diagnosis - Organic Tics - less complex than compulsion - not preceded by obsessive thought
- 34. PANDAS Pediatric Autoimmune Neuropsychiatric Disorders Associated with group A beta-haemolytic streptococcus (GABHS) Some kids may develop
- 35. PANDAS:clinical phenotypes Psychiatric disorders: OCD, ADHD, anxiety,depression, emotional instability Movement disorders: Sydenham’s chorea, tic disorder, dystonia
- 36. PANDAS:Pathogenesis Molecular mimicry: M protein amino acid sequence on streptococcal cell wall share homology with host
- 37. PANDAS:Pathogenesis (con’t) Five criteria for autoimmune neurological disease: a/ presence of autoantibody b/ immunoglobulins at target
- 38. Differential Diagnosis - Psychiatric Schizophrenia - delusional belief is “fixed” (overvalued idea in OCD) Major Depressive
- 39. Differential Diagnosis - Psychiatric Obsessive-Compulsive Personality Disorder (ego syntonic vs. dystonic in OCD) Pervasive Developmental Disorder
- 40. Differential Diagnosis -Psychiatric/Veterinary Canine Acral Lick Syndrome in patient with Lycanthropy Veterinarians treat acral lick with
- 41. Comorbid Diagnoses Major Depressive Disorder - most common (1/3 to 2/3 of OCD patients have MDD)
- 42. Comorbid Diagnoses (cont.) Tourette’s Syndrome - 1/3 to 2/3 have OCD Attention-Deficit/Hyperactivity Disorder Classic triad: ADHD
- 43. Treatment Combination (pharmacotherapy/psychotherapy) treatment best Serotinergic antidepressants (SRIs) Behavioral therapy Cognitive therapy Group therapy Family/marital therapy
- 44. Pharmacotherapy - SRIs SSRIs fluoxetine (60-80mg) sertraline (150-200mg) paroxetine (40-60mg) fluvoxamine (200-300mg) citalopram (40-60gm) All equally
- 45. Resistant OCD: Switch/Augmentation First, try a second SSRI, venlafaxine or clomipramine Neuroleptic -tics, TS, schizoid IV
- 46. OCD: experimental approaches 5HT1D receptor agonists –sumatriptan, zolmitriptan Inositol – membrane stabilization Clonidine – alpha2 –adrenergic
- 47. Behavioral Treatment More effective for compulsions As effective as medications Improvement lasts longer than medications Exposure
- 48. Example of exposure hierarchy for a obsessional fear of cancer Read an article about cancer Watch
- 49. Cognitive psychotherapy Inflated responsibility Overimportance of thoughts Excessive concern about controlling thoughts Overestimation of threat Salkovskis,
- 50. Behavioral observations that suggest OCD Raw or reddened hands skin from excessive washing Questions from the
- 51. “Heroic” Treatments Electroconvulsive therapy - case studies Psychosurgery - 25-65% success - stereotactic cingulotomy - limbic
- 52. Therapeutic brain stimulation TMS, DBS, VNS TMS-transcranial magnetic stimulation Single session of right prefrontal rTMS (20Hz)decrease
- 53. TMS TMS-noninvasive focal brain stimulation TMS-high-intensity current is rapidly turned on and off in the electromagnetic
- 54. TMS TMS - MDD TMS-side effects: seizures
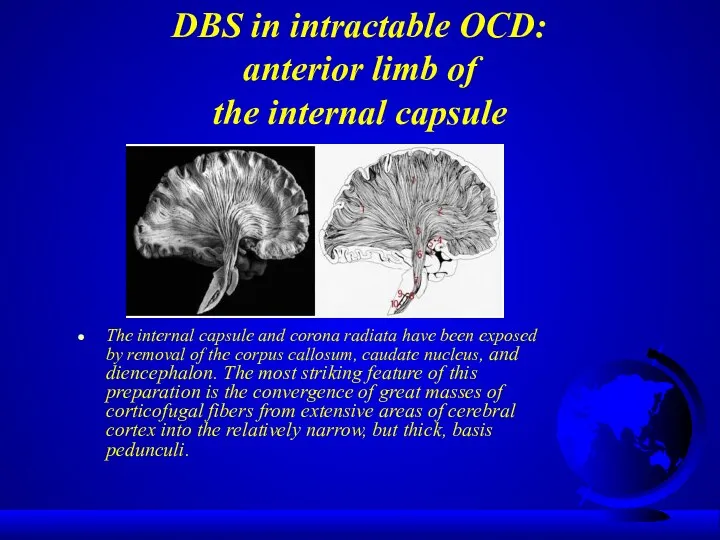
- 55. DBS in intractable OCD: anterior limb of the internal capsule The internal capsule and corona radiata
- 56. Treatment response 25% significant improvement 50% moderate improvement 25% unchanged or worse
- 57. Poor Prognosis yield to compulsive rituals severe symptoms + functional impairment comorbid diagnoses childhood onset poor
- 58. Most Common Presentations Contamination - cleaning - avoid touching Doubt/incompleteness - checking Agressive thought - mental
- 59. Good Prognosis precipitating event episodic symptoms good premorbid functioning shorter duration comorbid additional anxiety disorder diagnosis
- 60. Obsessive-Compulsive Spectrum Disorders Similar symptoms (repetitive thoughts and/or behaviors) Similar features: - age of onset -
- 61. OC Spectrum Disorders Focus on body appearence and sensations: Somatoform Disorders: - Hypochondriasis - Body Dysmorphic
- 62. Psychodynamic Theory Obsessions and compulsions involve regression from the oedipal to the anal stage of development
- 63. OC Spectrum Disorders Neurological Disorders: - Tourette’s Syndrome - Sydenham’s Chorea - Torticollis Impulse Control Disorders:
- 64. OC Spectrum Disorders “Mall Disorder”: Kleptomania + Compulsive Shopping + Binge Eating
- 65. Compulsive / impulsive subspectrum BDD,OCD, anorexia, hypochondriasis High harm avoidance Risk aversion Resistance Anticipatory anxiety Lack
- 66. Similarities between OCD and selected OCD-spectrum disorders Domain BDD Tourette’s Hypochondriasis Trichotillomania Symptoms Comorbidity with OCD
- 67. Finis
- 69. Outline Epidemiology Etiology Diagnostic Criteria Clinical Presentation Differential Diagnosis Comorbidity Treatment Prognosis Obsessive-Compulsive Spectrum Disorders
- 70. The ritual takes 1 minute and 25 seconds to put on each foot sneaker, a task
- 71. Behavioral Theory Obsession is a conditioned stimulus A neutral stimulus is paired with an event that
- 72. Integration Ventral cortico-striatal-thalamo-cortical circuit - recognition of behaviorally significant stimuli and in error detection - regulation
- 74. Скачать презентацию
Why Discuss OCD?
Underdiagnosed (4th most common psychiatric diagnosis)
More common than previously
Why Discuss OCD?
Underdiagnosed (4th most common psychiatric diagnosis)
More common than previously
Why is OCD Underdiagnosed?
Symptoms are embarrassing
Lack of insight into problems
Why is OCD Underdiagnosed?
Symptoms are embarrassing
Lack of insight into problems
OCD – a secretive disorder
62% - ignorance of illness
35% - fear
OCD – a secretive disorder
62% - ignorance of illness
35% - fear
The Problem...
The average patient does not receive appropriate treatment for 17
The Problem...
The average patient does not receive appropriate treatment for 17
Epidemiology
Lifetime prevalence 2-3%
U.S.A. 5-7 million adults
1 million kids
Mean age of
Epidemiology
Lifetime prevalence 2-3%
U.S.A. 5-7 million adults
1 million kids
Mean age of
Etiology
Genetic factors
Biologic factors
Behavioral theory
Psychodynamic theory
Etiology
Genetic factors
Biologic factors
Behavioral theory
Psychodynamic theory
Genetic Factors
Inheritance most evident in childhood onset OCD
10% of 1st degree
Genetic Factors
Inheritance most evident in childhood onset OCD
10% of 1st degree
Neuroanatomy: striatal disorders
Tourette’s syndrome
Sydenham’s chorea
Huntington’s disease
Parkinson’s disease
Encephalitis Economo
Neuroanatomy: striatal disorders
Tourette’s syndrome
Sydenham’s chorea
Huntington’s disease
Parkinson’s disease
Encephalitis Economo
OCD: brain disorder
(Cortico-striatal-thalamo-cortical circuit)
Neurological soft signs
Evoked potentials
Prepulse inhibition
Executive function
TMS
Conclusion:
OCD: brain disorder
(Cortico-striatal-thalamo-cortical circuit)
Neurological soft signs
Evoked potentials
Prepulse inhibition
Executive function
TMS
Conclusion:
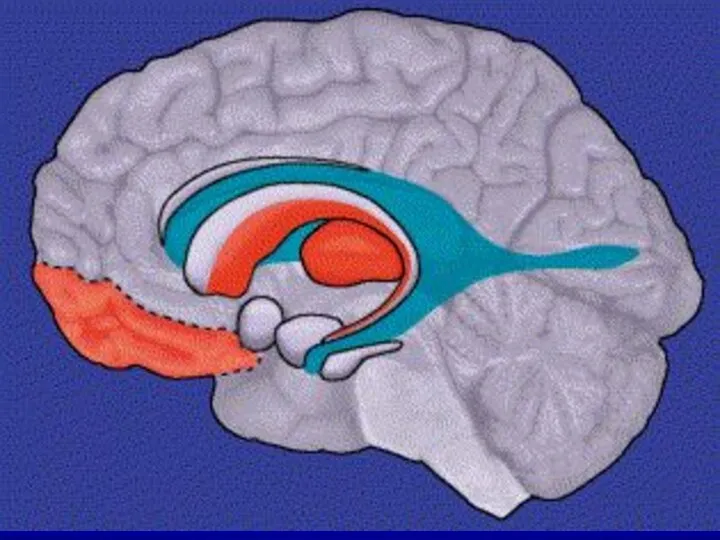
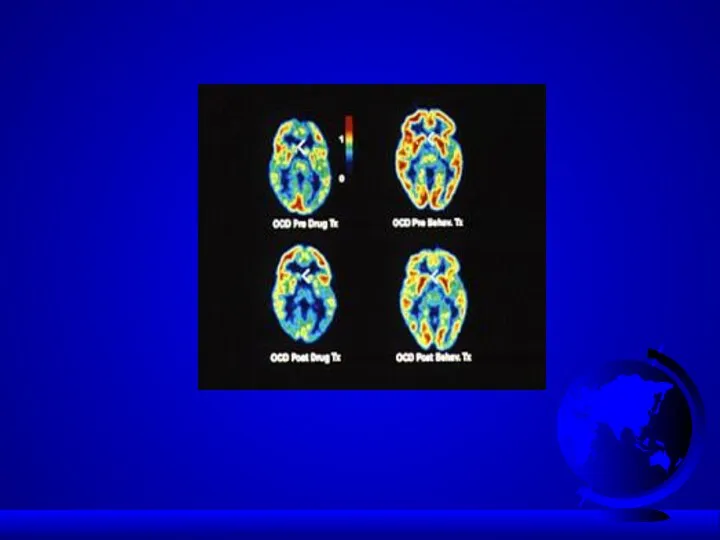
OCD: brain disorder
Frontal lobe
basal ganglia
anterior/posterior cingulate
PET scan:
OCD: brain disorder
Frontal lobe
basal ganglia
anterior/posterior cingulate
PET scan:
Neurochemistry: 5HT system
Neurotransmitter dysregulation
Serotonin
- SRI drugs work
- >
Neurochemistry: 5HT system
Neurotransmitter dysregulation
Serotonin
- SRI drugs work
- >
Neurochemistry: dopamine
Dopamine agonists – induced OCD (cocaine, methylphenidate)
Dopamine antagonists – effective
Neurochemistry: dopamine
Dopamine agonists – induced OCD (cocaine, methylphenidate)
Dopamine antagonists – effective
Neurochemistry:
other than 5HT/DA systems
Glutamate
Neuropeptides
Gonadal steroids
Second/third messengers (protein kinase C)
Opiates
Neurochemistry:
other than 5HT/DA systems
Glutamate
Neuropeptides
Gonadal steroids
Second/third messengers (protein kinase C)
Opiates
Diagnosis (DSM-5)
Must have either obsessions or compulsions
Obsessions - increase anxiety
Compulsions -
Diagnosis (DSM-5)
Must have either obsessions or compulsions
Obsessions - increase anxiety
Compulsions -
Diagnosis (cont.)
Compulsions:
- repetitive behaviors or thoughts
- patient feels compelled
Diagnosis (cont.)
Compulsions:
- repetitive behaviors or thoughts
- patient feels compelled
Diagnosis (cont.)
Patient realizes that the obsessions and compulsions are excessive and
Diagnosis (cont.)
Patient realizes that the obsessions and compulsions are excessive and
Clinical Presentation
OCD patients often first seen by clinician other than psychiatrist/psychologist
75-85%
Clinical Presentation
OCD patients often first seen by clinician other than psychiatrist/psychologist
75-85%
Clinical Presentation (cont.)
50-75% onset after stressful event (ex., move/ new school
Clinical Presentation (cont.)
50-75% onset after stressful event (ex., move/ new school
Contamination Obsession (cont.)
Lengthy shower
Family collusion (father/garage)
Contamination Obsession (cont.)
Lengthy shower
Family collusion (father/garage)
Pathological Doubt Obsession
How many times do you check your locked door,
Pathological Doubt Obsession
How many times do you check your locked door,
Pathological Doubt Cases
Front door checking/staring (20 min.)
Jack Nicholson (door) in “As
Pathological Doubt Cases
Front door checking/staring (20 min.)
Jack Nicholson (door) in “As
Aggressive Thoughts Obsession
Religious theme suggests harsh, punitive superego
Urge to shout obscenities
Aggressive Thoughts Obsession
Religious theme suggests harsh, punitive superego
Urge to shout obscenities
Obsession about Symmetry/Precision
Compulsive ritual involves slow and meticulous behavior
Jack Nicholson avoiding
Obsession about Symmetry/Precision
Compulsive ritual involves slow and meticulous behavior
Jack Nicholson avoiding
Other Presentations
Touching
Religious obsessions (hypermorality)
Pathological fear of voiding in public
(planning and
Other Presentations
Touching
Religious obsessions (hypermorality)
Pathological fear of voiding in public
(planning and

Rituals vs Compulsions
Rituals Compulsions
Calming Suffering
Socializing function Aggravation
Rituals vs Compulsions
Rituals Compulsions
Calming Suffering
Socializing function Aggravation
OCD dimensions
Symmetry / ordering, counting, repeating
Hoarding obsessions / compulsions
Contamination obsessions
OCD dimensions
Symmetry / ordering, counting, repeating
Hoarding obsessions / compulsions
Contamination obsessions
OCD dimensions
Stability over time
Differential treatment response
Neural correlates
Possible differential genetic underprint
OCD dimensions
Stability over time
Differential treatment response
Neural correlates
Possible differential genetic underprint
Early-onset OCD
Anger attacks
Continuous compulsive questions “Mom, you won’t due tonight?”
Tyrannical orders
Early-onset OCD
Anger attacks
Continuous compulsive questions “Mom, you won’t due tonight?”
Tyrannical orders
Neural Correlates
Striatal/thalamic I. Checking compulsions /
sexual, aggressive obsessions
II. Symmetry obsessions
Neural Correlates
Striatal/thalamic I. Checking compulsions /
sexual, aggressive obsessions
II. Symmetry obsessions
Differential Diagnosis - Organic
Tics - less complex than compulsion
-
Differential Diagnosis - Organic
Tics - less complex than compulsion
-

PANDAS
Pediatric Autoimmune Neuropsychiatric Disorders Associated with group A beta-haemolytic streptococcus (GABHS)
Some
PANDAS
Pediatric Autoimmune Neuropsychiatric Disorders Associated with group A beta-haemolytic streptococcus (GABHS)
Some

PANDAS:clinical phenotypes
Psychiatric disorders: OCD, ADHD, anxiety,depression, emotional instability
Movement disorders: Sydenham’s chorea,
PANDAS:clinical phenotypes
Psychiatric disorders: OCD, ADHD, anxiety,depression, emotional instability
Movement disorders: Sydenham’s chorea,
PANDAS:Pathogenesis
Molecular mimicry: M protein amino acid sequence on streptococcal cell wall
PANDAS:Pathogenesis
Molecular mimicry: M protein amino acid sequence on streptococcal cell wall

PANDAS:Pathogenesis (con’t)
Five criteria for autoimmune neurological disease:
a/ presence of autoantibody
PANDAS:Pathogenesis (con’t)
Five criteria for autoimmune neurological disease:
a/ presence of autoantibody
Differential Diagnosis - Psychiatric
Schizophrenia - delusional belief is “fixed” (overvalued idea
Differential Diagnosis - Psychiatric
Schizophrenia - delusional belief is “fixed” (overvalued idea
Differential Diagnosis - Psychiatric
Obsessive-Compulsive Personality Disorder (ego syntonic vs. dystonic in
Differential Diagnosis - Psychiatric
Obsessive-Compulsive Personality Disorder (ego syntonic vs. dystonic in
Differential Diagnosis -Psychiatric/Veterinary
Canine Acral Lick Syndrome in patient with Lycanthropy
Veterinarians treat
Differential Diagnosis -Psychiatric/Veterinary
Canine Acral Lick Syndrome in patient with Lycanthropy
Veterinarians treat

Comorbid Diagnoses
Major Depressive Disorder - most common (1/3 to 2/3 of
Comorbid Diagnoses
Major Depressive Disorder - most common (1/3 to 2/3 of
Comorbid Diagnoses (cont.)
Tourette’s Syndrome - 1/3 to 2/3 have OCD
Attention-Deficit/Hyperactivity Disorder
Classic
Comorbid Diagnoses (cont.)
Tourette’s Syndrome - 1/3 to 2/3 have OCD
Attention-Deficit/Hyperactivity Disorder
Classic

Treatment
Combination (pharmacotherapy/psychotherapy) treatment best
Serotinergic antidepressants (SRIs)
Behavioral therapy
Cognitive therapy
Group therapy
Family/marital
Treatment
Combination (pharmacotherapy/psychotherapy) treatment best
Serotinergic antidepressants (SRIs)
Behavioral therapy
Cognitive therapy
Group therapy
Family/marital
Pharmacotherapy - SRIs
SSRIs fluoxetine (60-80mg) sertraline (150-200mg)
paroxetine (40-60mg) fluvoxamine
Pharmacotherapy - SRIs
SSRIs fluoxetine (60-80mg) sertraline (150-200mg)
paroxetine (40-60mg) fluvoxamine
Resistant OCD: Switch/Augmentation
First, try a second SSRI, venlafaxine or clomipramine
Neuroleptic -tics,
Resistant OCD: Switch/Augmentation
First, try a second SSRI, venlafaxine or clomipramine
Neuroleptic -tics,
OCD: experimental approaches
5HT1D receptor agonists –sumatriptan, zolmitriptan
Inositol – membrane stabilization
Clonidine –
OCD: experimental approaches
5HT1D receptor agonists –sumatriptan, zolmitriptan
Inositol – membrane stabilization
Clonidine –
Behavioral Treatment
More effective for compulsions
As effective as medications
Improvement lasts longer
Behavioral Treatment
More effective for compulsions
As effective as medications
Improvement lasts longer

Example of exposure hierarchy for a obsessional fear of cancer
Read an
Example of exposure hierarchy for a obsessional fear of cancer
Read an
Cognitive psychotherapy
Inflated responsibility
Overimportance of thoughts
Excessive concern about controlling thoughts
Overestimation of threat
Salkovskis,
Cognitive psychotherapy
Inflated responsibility
Overimportance of thoughts
Excessive concern about controlling thoughts
Overestimation of threat
Salkovskis,
Behavioral observations that suggest OCD
Raw or reddened hands skin from excessive
Behavioral observations that suggest OCD
Raw or reddened hands skin from excessive
“Heroic” Treatments
Electroconvulsive therapy - case studies
Psychosurgery - 25-65% success
- stereotactic
“Heroic” Treatments
Electroconvulsive therapy - case studies
Psychosurgery - 25-65% success
- stereotactic
Therapeutic brain stimulation
TMS, DBS, VNS
TMS-transcranial magnetic stimulation
Single session of right
Therapeutic brain stimulation
TMS, DBS, VNS
TMS-transcranial magnetic stimulation
Single session of right

TMS
TMS-noninvasive focal brain stimulation
TMS-high-intensity current is rapidly turned on and off
TMS
TMS-noninvasive focal brain stimulation
TMS-high-intensity current is rapidly turned on and off
TMS
TMS - MDD
TMS-side effects: seizures
TMS
TMS - MDD
TMS-side effects: seizures
DBS in intractable OCD:
anterior limb of
the internal capsule
The internal
DBS in intractable OCD:
anterior limb of
the internal capsule
The internal
Treatment response
25% significant improvement
50% moderate improvement
25% unchanged or worse
Treatment response
25% significant improvement
50% moderate improvement
25% unchanged or worse
Poor Prognosis
yield to compulsive rituals
severe symptoms + functional impairment
comorbid diagnoses
childhood
Poor Prognosis
yield to compulsive rituals
severe symptoms + functional impairment
comorbid diagnoses
childhood
Most Common Presentations
Contamination - cleaning
- avoid touching
Doubt/incompleteness - checking
Agressive thought
Most Common Presentations
Contamination - cleaning
- avoid touching
Doubt/incompleteness - checking
Agressive thought

Good Prognosis
precipitating event
episodic symptoms
good premorbid functioning
shorter duration
comorbid additional anxiety
Good Prognosis
precipitating event
episodic symptoms
good premorbid functioning
shorter duration
comorbid additional anxiety
Obsessive-Compulsive Spectrum Disorders
Similar symptoms (repetitive thoughts and/or behaviors)
Similar features:
- age
Obsessive-Compulsive Spectrum Disorders
Similar symptoms (repetitive thoughts and/or behaviors)
Similar features:
- age
OC Spectrum Disorders
Focus on body appearence and sensations: Somatoform Disorders:
OC Spectrum Disorders
Focus on body appearence and sensations: Somatoform Disorders:
Psychodynamic Theory
Obsessions and compulsions involve regression from the oedipal to the
Psychodynamic Theory
Obsessions and compulsions involve regression from the oedipal to the

OC Spectrum Disorders
Neurological Disorders:
- Tourette’s Syndrome
- Sydenham’s Chorea
-
OC Spectrum Disorders
Neurological Disorders:
- Tourette’s Syndrome
- Sydenham’s Chorea
-
OC Spectrum Disorders
“Mall Disorder”:
Kleptomania
+ Compulsive Shopping
+ Binge
OC Spectrum Disorders
“Mall Disorder”:
Kleptomania
+ Compulsive Shopping
+ Binge

Compulsive / impulsive subspectrum
BDD,OCD, anorexia, hypochondriasis
High harm avoidance
Risk aversion
Resistance
Anticipatory anxiety
Lack of
Compulsive / impulsive subspectrum
BDD,OCD, anorexia, hypochondriasis
High harm avoidance
Risk aversion
Resistance
Anticipatory anxiety
Lack of
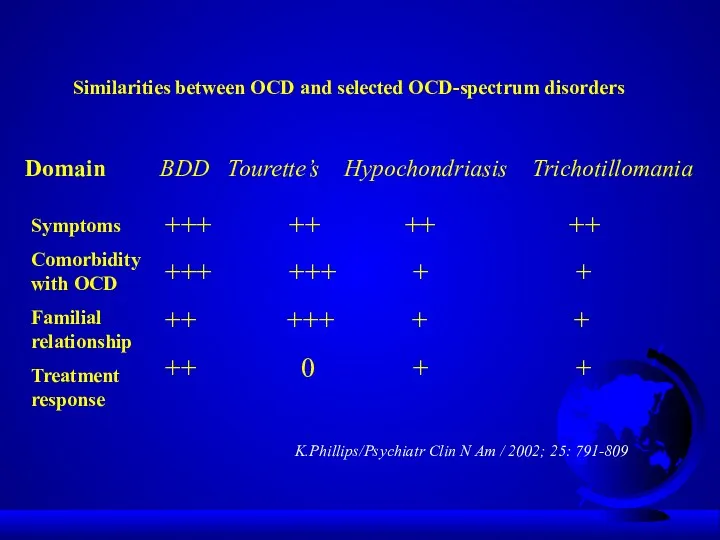
Similarities between OCD and selected OCD-spectrum disorders
Domain BDD Tourette’s Hypochondriasis Trichotillomania
Symptoms
Comorbidity
Similarities between OCD and selected OCD-spectrum disorders
Domain BDD Tourette’s Hypochondriasis Trichotillomania
Symptoms
Comorbidity
Finis
Finis

Outline
Epidemiology
Etiology
Diagnostic Criteria
Clinical Presentation
Differential Diagnosis
Comorbidity
Treatment
Prognosis
Obsessive-Compulsive Spectrum Disorders
Outline
Epidemiology
Etiology
Diagnostic Criteria
Clinical Presentation
Differential Diagnosis
Comorbidity
Treatment
Prognosis
Obsessive-Compulsive Spectrum Disorders
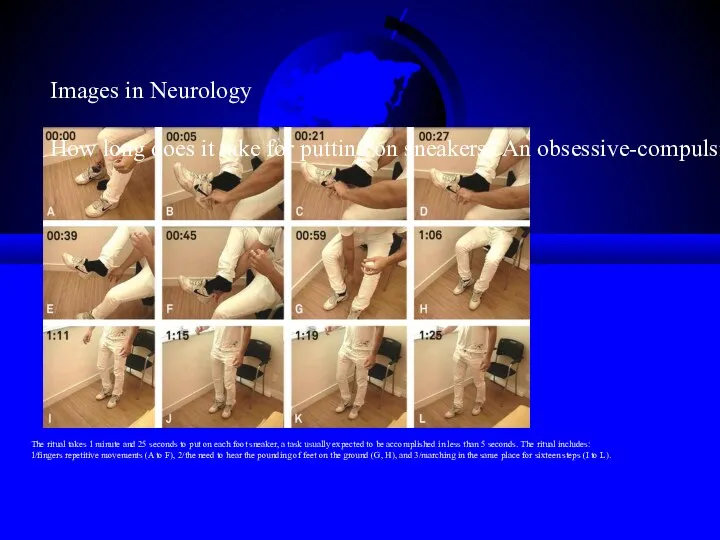
The ritual takes 1 minute and 25 seconds to put on
The ritual takes 1 minute and 25 seconds to put on
Behavioral Theory
Obsession is a conditioned stimulus
A neutral stimulus is paired with
Behavioral Theory
Obsession is a conditioned stimulus
A neutral stimulus is paired with
Integration
Ventral cortico-striatal-thalamo-cortical circuit
- recognition of behaviorally significant
stimuli and in
Integration
Ventral cortico-striatal-thalamo-cortical circuit
- recognition of behaviorally significant
stimuli and in
 Утомление, переутомление, перетренированность. Хроническое физическое перенапряжение систем организма. Внезапная смерть в спорте
Утомление, переутомление, перетренированность. Хроническое физическое перенапряжение систем организма. Внезапная смерть в спорте Принципы лучевой терапии ЗНО. Брахитерапия и сочетано-лучевая терапия
Принципы лучевой терапии ЗНО. Брахитерапия и сочетано-лучевая терапия Микробиологические методы лабораторной диагностики инфекционных заболеваний
Микробиологические методы лабораторной диагностики инфекционных заболеваний Особиста профілактика інфекційних захворюваннь
Особиста профілактика інфекційних захворюваннь Хронический пиелонефрит в практике участкового терапевта
Хронический пиелонефрит в практике участкового терапевта Геморрагическая лихорадка с почечным синдромом (ГЛПС)
Геморрагическая лихорадка с почечным синдромом (ГЛПС) Теория рационального питания. Гигиенические требования к рациональному питанию человека
Теория рационального питания. Гигиенические требования к рациональному питанию человека Виды ущемлений грыж
Виды ущемлений грыж Острые кишечные инфекции. Шигеллез. Сальмонеллез. (Лекция 4)
Острые кишечные инфекции. Шигеллез. Сальмонеллез. (Лекция 4) Микробиология чумы
Микробиология чумы Спортивное питание
Спортивное питание Лечение псориаза средней тяжести и тяжелого течения в эру биологической терапии
Лечение псориаза средней тяжести и тяжелого течения в эру биологической терапии Морально-этические проблемы трансплантологии
Морально-этические проблемы трансплантологии Нәрестенің гемолитикалық ауруы
Нәрестенің гемолитикалық ауруы Инфекции, передаваемые половым путём. Пути передачи, основные заболевания, меры профилактики
Инфекции, передаваемые половым путём. Пути передачи, основные заболевания, меры профилактики Жақ - бет аймағының одонтогенді емес ісіктері
Жақ - бет аймағының одонтогенді емес ісіктері Гипертензия, ишемическая болезнь сердца
Гипертензия, ишемическая болезнь сердца Острая жировая дистрофия печени. Холестатический гепатоз беременных
Острая жировая дистрофия печени. Холестатический гепатоз беременных Afecțiunile frecvente în neurorecuperare
Afecțiunile frecvente în neurorecuperare Основные симптомы неврологических расстройств
Основные симптомы неврологических расстройств Болезни органов дыхания. Гигиена дыхания
Болезни органов дыхания. Гигиена дыхания Стабільна ішемічна хвороба серця
Стабільна ішемічна хвороба серця Florence Nightingale - Pioneer of nursing
Florence Nightingale - Pioneer of nursing Клиническая анатомия позвоночника и спинного мозга
Клиническая анатомия позвоночника и спинного мозга Методы лучевой диагностики при исследовании тонкой кишки
Методы лучевой диагностики при исследовании тонкой кишки Курация больного с оформлением учебной истории болезни
Курация больного с оформлением учебной истории болезни Культура питания. Правила рационального питания
Культура питания. Правила рационального питания Санаторий-профилакторий ООО СО АРУ Саянская благодать
Санаторий-профилакторий ООО СО АРУ Саянская благодать