- Pharmacology of the respiratory system

Содержание
- 2. Respiratory Stimulants 1. Activating Respiratory Center Directly: Caffeine Bemegride – amp. 0.5% - 10 ml Etimizol
- 3. Mechanisms of Action of Caffeine 1). Blockade of Phosphodiesterase => ⇑ cAMP and ⇑cGMP 2) Blockade
- 4. Cordiamin (Niketamide) amp. 1 ml, vial 30 ml – an analeptic of mixed action ? Direct
- 5. Carbogen – is a mixture of 93-95% O2 with Carbon dioxide 5-7% CO2 It is used
- 6. Clinical Uses of Breathing Stimulants Acute Respiratory Failure : ► Asphyxia (Respiratory Arrest) in newborns and
- 7. Antitussive Drugs I. Central Cough Suppressants: 1. With opioid mechanism of action: Codeine Ethylmorphine Dextromethorphan 2.
- 8. Codeine (Methylmorphine) - an opioid alkaloid Analgesic properties – agonist activity at the opiate receptors Antitussive
- 9. ● Tablets Codeine: 0.015 g with Sodium Bicarbonate ● Tablets “Codterpine”: Codeine 0.015 g Sodium Bicarbonate
- 10. Glaucine hydrochloride – Tab. 0.05 g – It is an alkaloid from the Yellow Poppy plant
- 11. Libexine (Prenoxdiazine)- Tab. 0.1 g - a synthetic Antitussive of Peripheral Action Mechanism of action: inhibits
- 12. EXPECTORANTS I. BRONCHOSECRETOR DRUGS: 1. Reflex type of action: Thermopsis Grass Infusion: (0.6 – 180 ml)
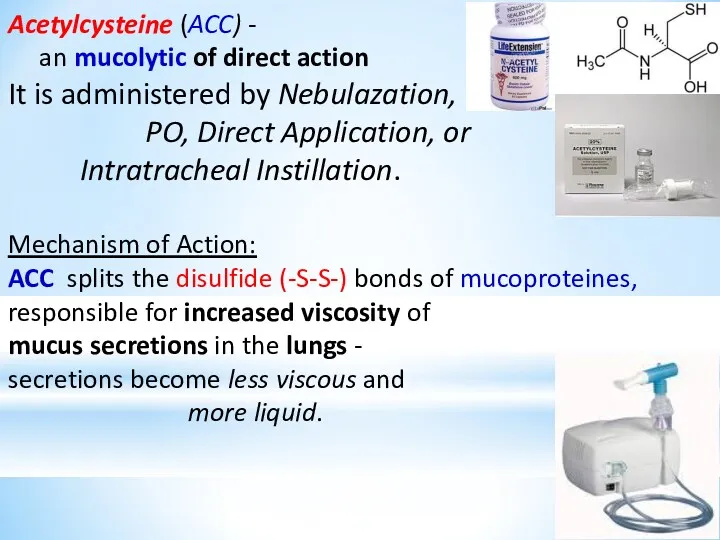
- 13. II. Mucolytic Drugs – convert sticky and viscous sputum to more liquid one and promote its
- 14. Acetylcysteine (ACC) - an mucolytic of direct action It is administered by Nebulazation, PO, Direct Application,
- 15. ACC is a Paracetamol antidote. The mechanism: ⮚ Restores hepatic stores of Glutatione – important in
- 16. Clinical uses of ACC: Acute and chronic broncho-pulmobary diseases Tracheostomy care Pulmonary complications of surgery Diagnostic
- 17. Bromhexine and Ambroxole – are Mucolytic and Expectorant Agents: Mechanism of Action: => Depolymerization of Mucoproteines
- 18. Potassium Iodide is an Expectorant and Antihyperthyroid Agent. It reduces viscosity of mucus by increasing respiratory
- 19. Sodium Bicarbonate - ? Viscosity of mucus ? Bronchial secretions Sodium Bicarbonate abuse have been associated
- 21. BRONCHODILATORS 1. Agents stimulating β2 – adrenoreceptors of bronchi: a) Selective β2-adrenomimetics (AMs): β2 -AMs of
- 22. 2. Methylxanthines – Spasmolytics of direct action: a) Theophylline preparations with short period of action: Theophylline
- 24. Salmeterol and Formoterol - have lipophilic properties Salbutamol and Fenoterol have minor length (11 Angstrem) and
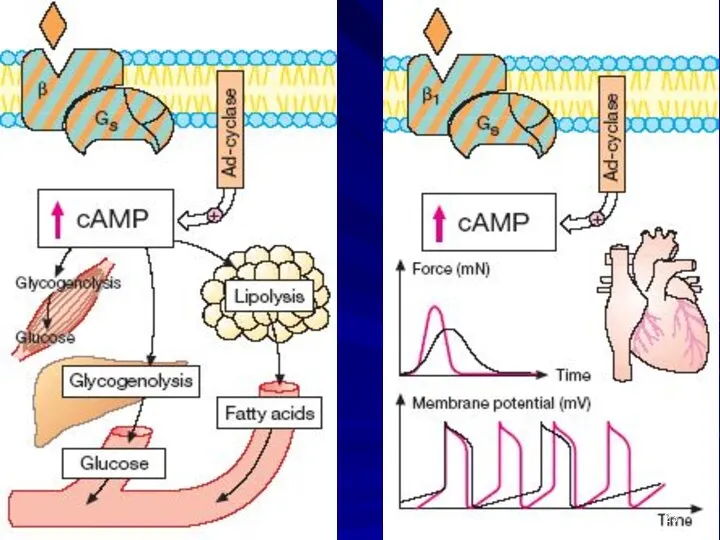
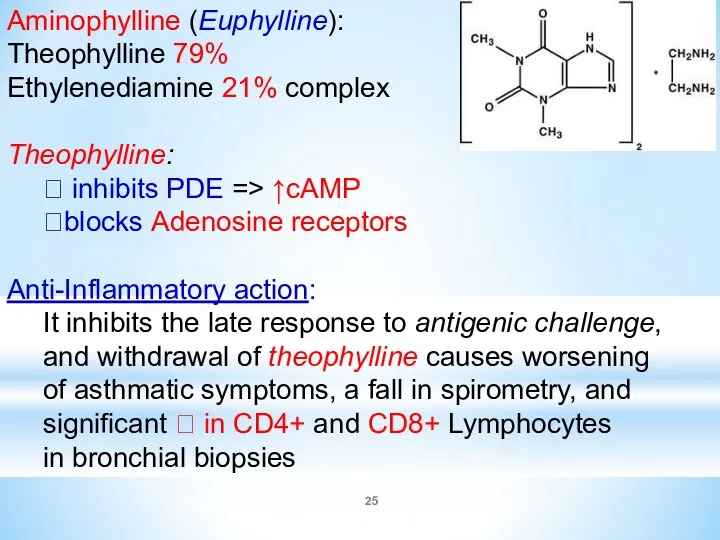
- 25. Aminophylline (Euphylline): Theophylline 79% Ethylenediamine 21% complex Theophylline: ⮞ inhibits PDE => ↑cAMP ⮞blocks Adenosine receptors
- 26. Clinical uses of Euphylline: ⮞ Asthma, including IV in Acute Severe Asthma ⮞ Chronic Obstructive Pulmonary
- 27. Drugs with Anti-Inflammatory Activity I. Steroid Anti-Inflammatory Drugs (SAIDs) – Glucocorticoids: 1. Natural – Hydrocortisone acetate
- 28. Mechanism of action of Glucocorticoids Steroid hormones are lipid soluble and cross cell membranes easily. Once
- 29. For Anti-inflammatory Action GCs produce: ∙ Inhibition of transcription of the genes for: COX-2, Cytokines (interleukins),
- 30. Pharmacological Effects of Glucocorticoids: ??Prostaglandin production due to decreased expression of COX-2; ? ?Generation of Cytokines
- 31. Glucocorticoids - do not relax airway smooth muscle directly but: ⮚ Stimulate the synthesis of enzymes
- 32. Glucocorticoids Beclometasone Butesonide Fluticasone - are given by inhalation with metered-dose inhaler, the full effect being
- 33. ADVERSE EFFECT OF GCs: Local Effects: Oropharyngeal Candidiasis – Thrush Systemic Effects: ?BP, Edema, CHF, Thromboembolism,
- 34. Cromolyn sodium (caps. 20 mg for inhalation) and Nedocromil (aerosol: 2 mg/dose) stabilize mast cells and
- 35. Ketotifen (tab. 1 mg), a cromolyn analog, is an antihistaminic (H1) with some cromolyn like action.
- 36. Montelukast (tab. 0.01 g) and Zafirlukast (Tab. 0.02 and 0.04 g): competitively inhibit cysteinyl Leukotriene receptors.
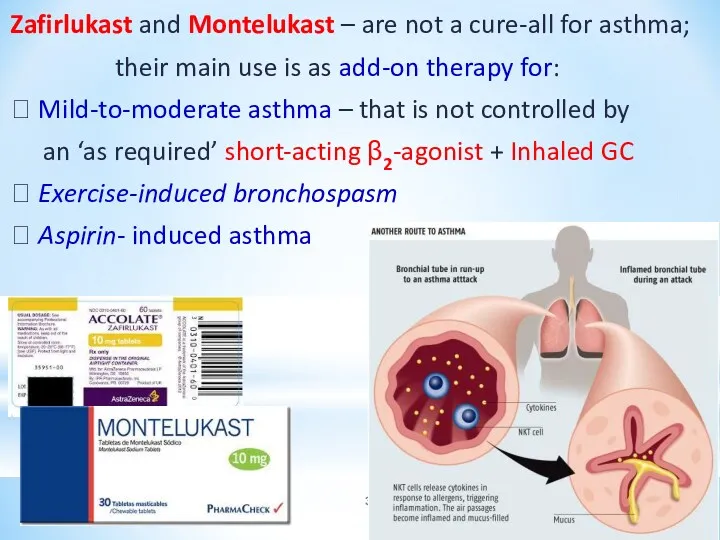
- 37. Zafirlukast and Montelukast – are not a cure-all for asthma; their main use is as add-on
- 39. Скачать презентацию
Respiratory Stimulants
1. Activating Respiratory Center Directly:
Caffeine
Bemegride – amp. 0.5%
Respiratory Stimulants
1. Activating Respiratory Center Directly:
Caffeine
Bemegride – amp. 0.5%
Mechanisms of Action of Caffeine
1). Blockade of Phosphodiesterase => ⇑ cAMP
Mechanisms of Action of Caffeine
1). Blockade of Phosphodiesterase => ⇑ cAMP
Cordiamin (Niketamide) amp. 1 ml, vial 30 ml –
an analeptic
Cordiamin (Niketamide) amp. 1 ml, vial 30 ml –
an analeptic
Carbogen – is a mixture of 93-95% O2 with
Carbon dioxide
Carbon dioxide
Clinical Uses of Breathing Stimulants
Acute Respiratory Failure :
► Asphyxia (Respiratory
Clinical Uses of Breathing Stimulants
Acute Respiratory Failure :
► Asphyxia (Respiratory
Antitussive Drugs
I. Central Cough Suppressants:
1. With opioid mechanism of action:
Antitussive Drugs
I. Central Cough Suppressants:
1. With opioid mechanism of action:
Codeine (Methylmorphine) - an opioid alkaloid
Analgesic properties –
agonist activity at
Codeine (Methylmorphine) - an opioid alkaloid
Analgesic properties –
agonist activity at
● Tablets Codeine: 0.015 g
with Sodium Bicarbonate
● Tablets “Codterpine”:
Codeine
● Tablets Codeine: 0.015 g
with Sodium Bicarbonate
● Tablets “Codterpine”:
Codeine
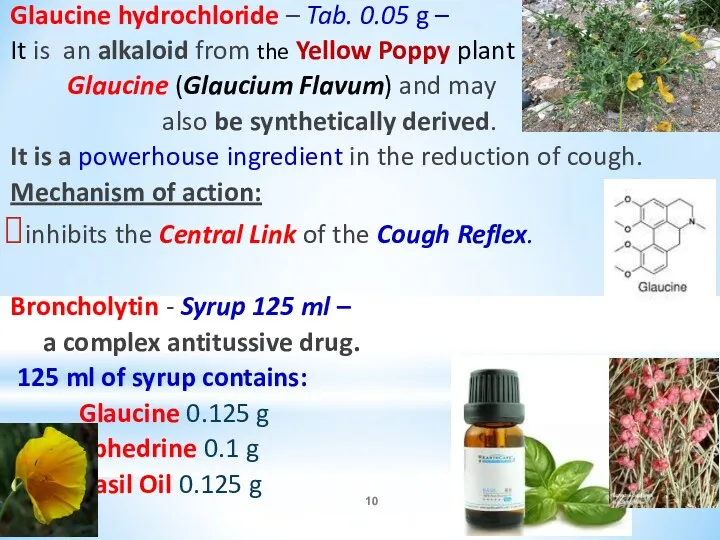
Glaucine hydrochloride – Tab. 0.05 g –
It is an alkaloid
Glaucine hydrochloride – Tab. 0.05 g –
It is an alkaloid
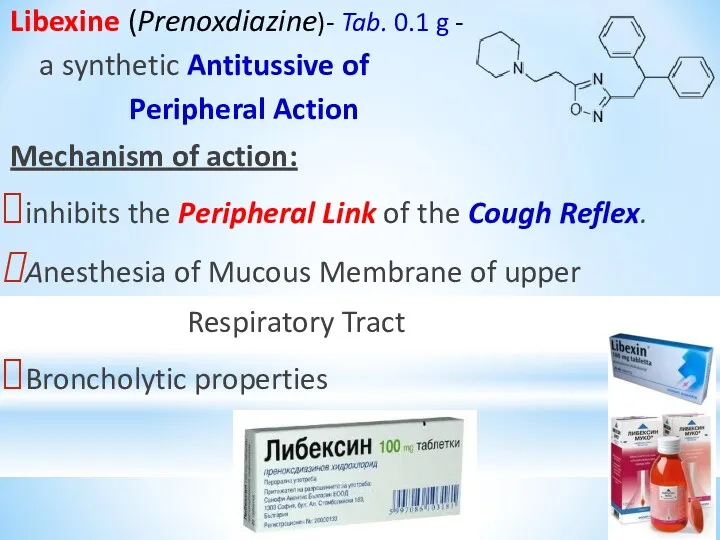
Libexine (Prenoxdiazine)- Tab. 0.1 g -
a synthetic Antitussive of
Libexine (Prenoxdiazine)- Tab. 0.1 g -
a synthetic Antitussive of
EXPECTORANTS
I. BRONCHOSECRETOR DRUGS:
1. Reflex type of action:
Thermopsis Grass Infusion: (0.6 –
EXPECTORANTS
I. BRONCHOSECRETOR DRUGS:
1. Reflex type of action:
Thermopsis Grass Infusion: (0.6 –
II. Mucolytic Drugs – convert sticky and viscous
sputum to more
II. Mucolytic Drugs – convert sticky and viscous
sputum to more
Acetylcysteine (ACC) -
an mucolytic of direct action
It is administered
Acetylcysteine (ACC) - an mucolytic of direct action It is administered
ACC is a Paracetamol antidote.
The mechanism:
⮚ Restores hepatic stores
ACC is a Paracetamol antidote.
The mechanism:
⮚ Restores hepatic stores
Clinical uses of ACC:
Acute and chronic broncho-pulmobary diseases
Tracheostomy care
Pulmonary complications of
Clinical uses of ACC:
Acute and chronic broncho-pulmobary diseases
Tracheostomy care
Pulmonary complications of
Bromhexine and Ambroxole –
are Mucolytic and Expectorant Agents:
Mechanism of Action:
=> Depolymerization
Bromhexine and Ambroxole –
are Mucolytic and Expectorant Agents:
Mechanism of Action:
=> Depolymerization
Potassium Iodide is an Expectorant and
Antihyperthyroid Agent.
It reduces viscosity
Potassium Iodide is an Expectorant and
Antihyperthyroid Agent.
It reduces viscosity
Sodium Bicarbonate -
? Viscosity of mucus
? Bronchial secretions
Sodium Bicarbonate abuse have
Sodium Bicarbonate -
? Viscosity of mucus
? Bronchial secretions
Sodium Bicarbonate abuse have
BRONCHODILATORS
1. Agents stimulating β2 – adrenoreceptors of bronchi:
a) Selective β2-adrenomimetics (AMs):
β2
BRONCHODILATORS
1. Agents stimulating β2 – adrenoreceptors of bronchi:
a) Selective β2-adrenomimetics (AMs):
β2
2. Methylxanthines – Spasmolytics of direct action:
a) Theophylline preparations with
a) Theophylline preparations with
Salmeterol and Formoterol - have lipophilic properties
Salbutamol and Fenoterol have
Salmeterol and Formoterol - have lipophilic properties
Salbutamol and Fenoterol have
Aminophylline (Euphylline):
Theophylline 79%
Ethylenediamine 21% complex
Theophylline:
⮞ inhibits PDE => ↑cAMP
⮞blocks
Aminophylline (Euphylline):
Theophylline 79%
Ethylenediamine 21% complex
Theophylline:
⮞ inhibits PDE => ↑cAMP
⮞blocks
Clinical uses of Euphylline:
⮞ Asthma, including IV in
Acute
Clinical uses of Euphylline:
⮞ Asthma, including IV in
Acute
Drugs with Anti-Inflammatory Activity
I. Steroid Anti-Inflammatory Drugs (SAIDs) – Glucocorticoids:
1. Natural
Drugs with Anti-Inflammatory Activity
I. Steroid Anti-Inflammatory Drugs (SAIDs) – Glucocorticoids:
1. Natural
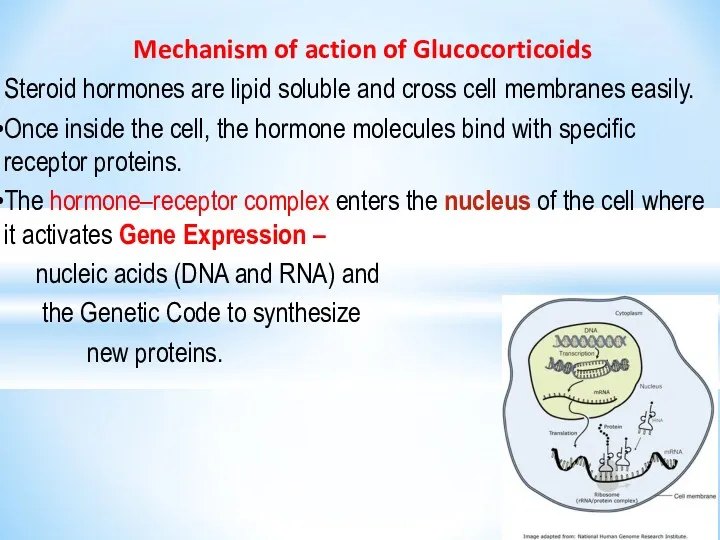
Mechanism of action of Glucocorticoids
Steroid hormones are lipid soluble
Mechanism of action of Glucocorticoids
Steroid hormones are lipid soluble
For Anti-inflammatory Action GCs produce:
∙ Inhibition of transcription of the genes
For Anti-inflammatory Action GCs produce:
∙ Inhibition of transcription of the genes
Pharmacological Effects of Glucocorticoids:
??Prostaglandin production due to decreased expression
of COX-2;
?
Pharmacological Effects of Glucocorticoids:
??Prostaglandin production due to decreased expression
of COX-2;
?
Glucocorticoids - do not relax airway smooth muscle directly but:
⮚ Stimulate
⮚ Stimulate
Glucocorticoids
Beclometasone
Butesonide
Fluticasone
- are given by inhalation with metered-dose
Glucocorticoids
Beclometasone
Butesonide
Fluticasone
- are given by inhalation with metered-dose
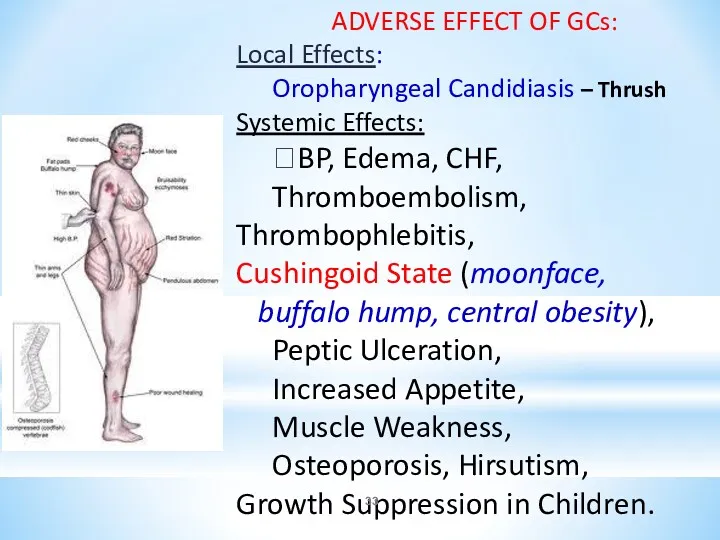
ADVERSE EFFECT OF GCs:
Local Effects:
Oropharyngeal Candidiasis – Thrush Systemic Effects:
?BP,
ADVERSE EFFECT OF GCs:
Local Effects:
Oropharyngeal Candidiasis – Thrush Systemic Effects:
?BP,
Cromolyn sodium (caps. 20 mg for inhalation) and Nedocromil (aerosol: 2
Cromolyn sodium (caps. 20 mg for inhalation) and Nedocromil (aerosol: 2
Ketotifen (tab. 1 mg), a cromolyn analog,
is an antihistaminic
Ketotifen (tab. 1 mg), a cromolyn analog,
is an antihistaminic
Montelukast (tab. 0.01 g) and
Zafirlukast (Tab. 0.02 and 0.04 g):
Montelukast (tab. 0.01 g) and
Zafirlukast (Tab. 0.02 and 0.04 g):
Zafirlukast and Montelukast – are not a cure-all for asthma;
their
Zafirlukast and Montelukast – are not a cure-all for asthma;
their
 Талассотерапия. Преимущества морского лечения
Талассотерапия. Преимущества морского лечения Көмейдің жедел және созылмалы стенозы. Кеңірдек стенозы. Коникотомия. Трехеостомия
Көмейдің жедел және созылмалы стенозы. Кеңірдек стенозы. Коникотомия. Трехеостомия ЭКГ при гипертрофии отделов сердца
ЭКГ при гипертрофии отделов сердца Особенности ухода за детьми грудного возраста
Особенности ухода за детьми грудного возраста Пластиночные протезы
Пластиночные протезы Патологические синдромы при рентгенологическом исследовании органов грудной клетки
Патологические синдромы при рентгенологическом исследовании органов грудной клетки ДВС-синдром (диссеминированное внутрисосудистое свёртывание) у беременных. Геморагический шок. Эмболия околоплодными водами
ДВС-синдром (диссеминированное внутрисосудистое свёртывание) у беременных. Геморагический шок. Эмболия околоплодными водами Уход за урологическими больными
Уход за урологическими больными Аппендицит. Острый аппендицит
Аппендицит. Острый аппендицит Методики коррекции заикания
Методики коррекции заикания Сага о плоскостопии
Сага о плоскостопии Дәрілік заттарды тіркеудің заманауи жүйесі
Дәрілік заттарды тіркеудің заманауи жүйесі Медицинское интервью и базовые коммуникационные навыки во взаимодействии врач-пациент
Медицинское интервью и базовые коммуникационные навыки во взаимодействии врач-пациент Анатомо-физиологические механизмы речи
Анатомо-физиологические механизмы речи Продукция коммерческого центра ЛАКРИМА
Продукция коммерческого центра ЛАКРИМА Международный день стоматолога
Международный день стоматолога Background and precancerous diseases of female genital. Malignant neoplasms of female genital organs
Background and precancerous diseases of female genital. Malignant neoplasms of female genital organs Патологоанатомическая диагностика болезней сердца у кошек в ветеринарной клинике
Патологоанатомическая диагностика болезней сердца у кошек в ветеринарной клинике Мониторинг лекарственных средств
Мониторинг лекарственных средств Тактика ведения беременных с экстрагенитальной патологией участковым терапевтом
Тактика ведения беременных с экстрагенитальной патологией участковым терапевтом Созылмалы қайталамалы автозды стоматит. Көптүрлі жалқықты эритема. Ауыз қуысындағы көрінісі
Созылмалы қайталамалы автозды стоматит. Көптүрлі жалқықты эритема. Ауыз қуысындағы көрінісі Профессиональные проблемы этики медицинских сестёр
Профессиональные проблемы этики медицинских сестёр Аллергические болезни слизистой полости рта у детей. Многоформная экссудативная эритема. Синдром Стивенса – Джонсона
Аллергические болезни слизистой полости рта у детей. Многоформная экссудативная эритема. Синдром Стивенса – Джонсона Операции на кровеносных сосудах
Операции на кровеносных сосудах Патофизиология периферического кровообращения
Патофизиология периферического кровообращения Коклюш у детей противоэпидемическая работа с детской поликлиникой
Коклюш у детей противоэпидемическая работа с детской поликлиникой Абсцесс
Абсцесс Pheochromocytomas
Pheochromocytomas