- Pneumonia in children. Diagnostics and treatment

Содержание
- 2. Plan of the lecture 1. Definition pneumonia 2. Etiology 3. Pneumonia pathogenesis 4. Classification of pneumonia
- 3. Pneumonia is a group of acute focal infectious inflammatory diseases varied in etiology, pathogenesis and morphologic
- 4. Predisposed anatomy-physiologic peculiarities in children to pneumonia Trachea and big bronchi are short and wide –
- 5. Predisposing premorbid factors for pneumonia Premature newborns Severe perinatal pathology: prenatal hypoxia, asphyxia, intrapartum trauma Vomiting
- 6. Pneumonia etiology Streptococcus Pneumonia ( 60-80% cases of community acquired pneumonia Hemophilus influenzae Moraxella Catarrhalis In
- 7. All microorganisms from sputum are divided into 3 groups pathogenic provisional pathogenic nonpathogenic
- 8. Pathogenic are microorganisms with complementary receptors to surface cell receptors in respiratory tract. It gives them
- 9. Diagnostic criteria of bacterial pneumonia Anamnestic data Hospital acquired pneumonia is developed in 48 hours after
- 10. Pneumonia classification in children
- 11. Focal pneumonia (30-40% of pneumonia) It frequently starts from bronchi – bronchopneumonia Frequently developed after ARD
- 12. Focal-confluent pneumonia Several segments are affected or the whole lobe with focal pulmonary destruction. Intoxication is
- 13. Segmental Pneumonia Pneumonia affects one or several segments. Moist rales are not typical or they disappear
- 14. Interstitial pneumonia (1% of all pneumonia) Acute inflammation of interstitium and less manifested affection of broncho
- 15. Croupous pneumonia Classic example of community acquired pneumonia. It is lobe or segment affection with pleura
- 16. Respiratory Failure –is a condition of disturbed gaseous blood composition due to lung function failure or
- 17. Clinical classification of respiratory failure Grade I Dyspnea after loading, in rest dyspnea is absent. Accessory
- 18. Main principles of pneumonia treatment Treatment must be opportune and integrated Etiotropic therapy directed for eradication
- 19. Indications for hospitalization Infants Respiratory failure, necessity of oxygen therapy, manifested intoxication Dehydration, impossibility of oral
- 20. Pay attention for Respiratory rate ( main index). In children 2-12 mo old RR> 50/min and
- 21. It’s important Air humidification in room where child is present Clothes must be suitable, surrounding temperature
- 22. Etiotropic therapy Foundation of etiotropic treatment is empiric start antibiotic therapy with following its correction Empiric
- 23. Main groups of antimicrobial drugs Beta-lactams 1. Penicillines 2. Cephalosporines 3. Monobactams (Aztreonam) 4. Carbapenems (Imipenem,
- 24. Main statements of antibiotic therapy Antibiotic administration must peroral in community acquired uncomplicated pneumonia In case
- 25. Efficacy criteria of antibiotic therapy in pneumonia Efficacy assessment is performed in uncomplicated pneumonia 24-48 hours
- 26. Effects of antibiotic therapy Complete effect- temperature decreasing less than 38C 24-48 hours later in uncomplicated
- 27. Side effects of antibiotic medication
- 28. Pathogenic treatment Respiratory supplementation according to respiratory failure Desintoxication. If indications are present intravenous infusion is
- 29. Segmental structure of lungs (scheme)
- 30. Questions To indicate etiologic and pathophysiologic factors at pneumonia in children To classify pneumonia, respiratory failure,
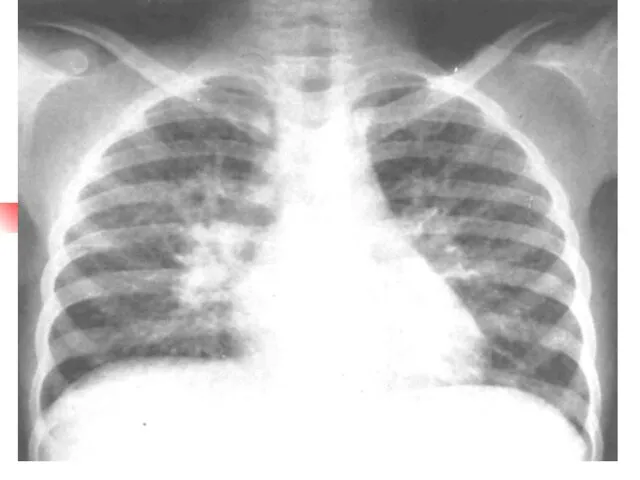
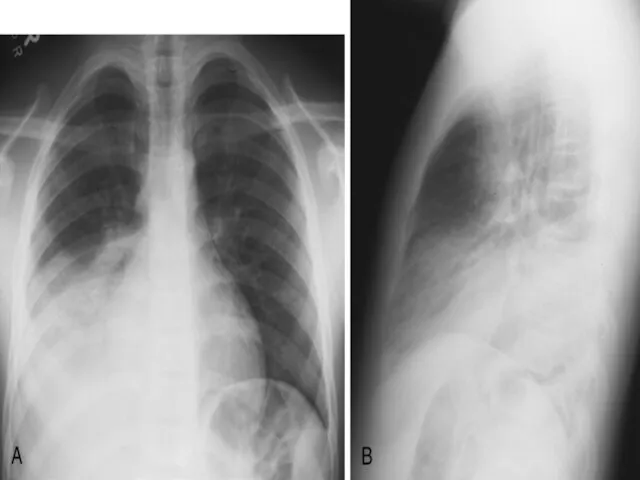
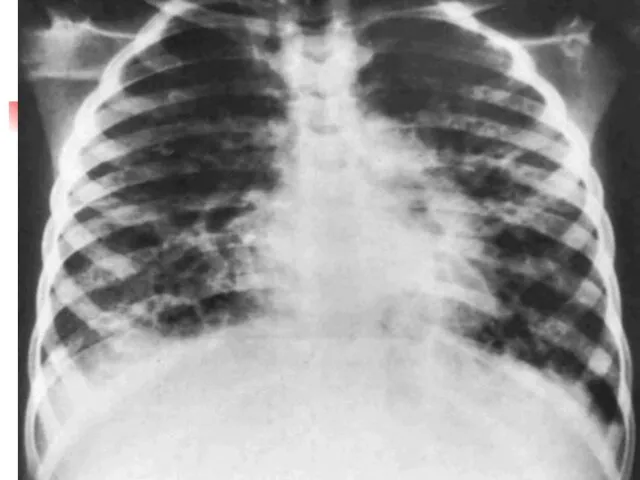
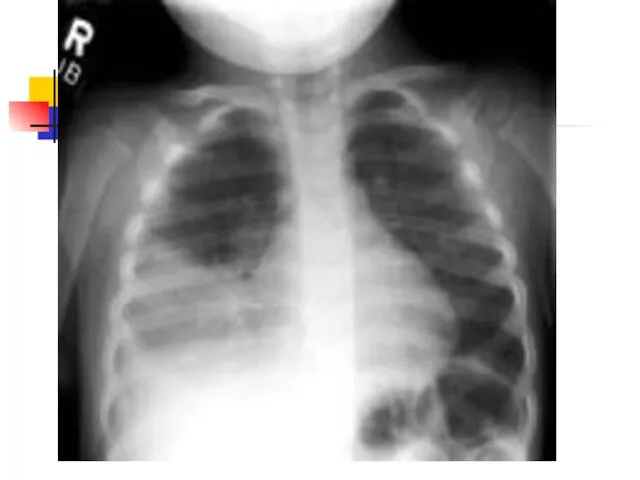
- 31. Pneumonia complication- pneumothorax
- 40. Скачать презентацию
Plan of the lecture
1. Definition pneumonia
2. Etiology
3. Pneumonia pathogenesis
4. Classification of
Plan of the lecture
1. Definition pneumonia
2. Etiology
3. Pneumonia pathogenesis
4. Classification of
Pneumonia is a group of acute focal infectious inflammatory diseases varied
Pneumonia is a group of acute focal infectious inflammatory diseases varied
Predisposed anatomy-physiologic peculiarities in children to pneumonia
Trachea and big bronchi
Predisposed anatomy-physiologic peculiarities in children to pneumonia
Trachea and big bronchi
Predisposing premorbid factors for pneumonia
Premature newborns
Severe perinatal pathology: prenatal hypoxia,
Predisposing premorbid factors for pneumonia
Premature newborns
Severe perinatal pathology: prenatal hypoxia,
Pneumonia etiology
Streptococcus Pneumonia ( 60-80% cases of community acquired pneumonia
Hemophilus influenzae
Moraxella
Pneumonia etiology
Streptococcus Pneumonia ( 60-80% cases of community acquired pneumonia
Hemophilus influenzae
Moraxella
All microorganisms from sputum are divided into 3 groups
pathogenic
provisional pathogenic
nonpathogenic
All microorganisms from sputum are divided into 3 groups
pathogenic
provisional pathogenic
nonpathogenic
Pathogenic are microorganisms with complementary receptors to surface cell receptors in
Pathogenic are microorganisms with complementary receptors to surface cell receptors in
Diagnostic criteria of bacterial pneumonia
Anamnestic data
Hospital acquired pneumonia is developed in
Diagnostic criteria of bacterial pneumonia
Anamnestic data
Hospital acquired pneumonia is developed in
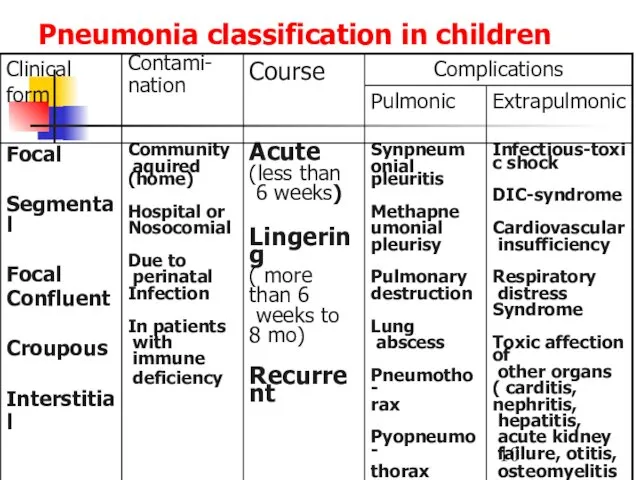
Pneumonia classification in children
Pneumonia classification in children
Focal pneumonia (30-40% of pneumonia)
It frequently starts from bronchi – bronchopneumonia
Frequently
Focal pneumonia (30-40% of pneumonia)
It frequently starts from bronchi – bronchopneumonia
Frequently
Focal-confluent pneumonia
Several segments are affected or the whole lobe with focal
Focal-confluent pneumonia
Several segments are affected or the whole lobe with focal
Segmental Pneumonia
Pneumonia affects one or several segments. Moist rales are not
Segmental Pneumonia
Pneumonia affects one or several segments. Moist rales are not
Interstitial pneumonia (1% of all pneumonia)
Acute inflammation of interstitium and less
Interstitial pneumonia (1% of all pneumonia)
Acute inflammation of interstitium and less
Croupous pneumonia
Classic example of community acquired pneumonia. It is lobe
or
Croupous pneumonia
Classic example of community acquired pneumonia. It is lobe
or
Respiratory Failure –is a condition of disturbed gaseous blood composition due
Respiratory Failure –is a condition of disturbed gaseous blood composition due
Clinical classification of respiratory failure
Grade I
Dyspnea after loading, in rest
Clinical classification of respiratory failure
Grade I
Dyspnea after loading, in rest
Main principles of pneumonia treatment
Treatment must be opportune and integrated
Etiotropic
Main principles of pneumonia treatment
Treatment must be opportune and integrated
Etiotropic
Indications for hospitalization
Infants
Respiratory failure, necessity of oxygen therapy, manifested intoxication
Dehydration,
Indications for hospitalization
Infants
Respiratory failure, necessity of oxygen therapy, manifested intoxication
Dehydration,

Pay attention for
Respiratory rate ( main index). In children 2-12
Pay attention for
Respiratory rate ( main index). In children 2-12
It’s important
Air humidification in room where child is present
Clothes must be
It’s important
Air humidification in room where child is present
Clothes must be
Etiotropic therapy
Foundation of etiotropic treatment is empiric start antibiotic therapy with
Etiotropic therapy
Foundation of etiotropic treatment is empiric start antibiotic therapy with
Main groups of antimicrobial drugs
Beta-lactams
1. Penicillines
2. Cephalosporines
3. Monobactams (Aztreonam)
4. Carbapenems (Imipenem,
Main groups of antimicrobial drugs
Beta-lactams
1. Penicillines
2. Cephalosporines
3. Monobactams (Aztreonam)
4. Carbapenems (Imipenem,
Main statements of antibiotic therapy
Antibiotic administration must peroral in community acquired
Main statements of antibiotic therapy
Antibiotic administration must peroral in community acquired
Efficacy criteria of antibiotic therapy in pneumonia
Efficacy assessment is performed in
Efficacy criteria of antibiotic therapy in pneumonia
Efficacy assessment is performed in
Effects of antibiotic therapy
Complete effect- temperature decreasing less than 38C 24-48
Effects of antibiotic therapy
Complete effect- temperature decreasing less than 38C 24-48
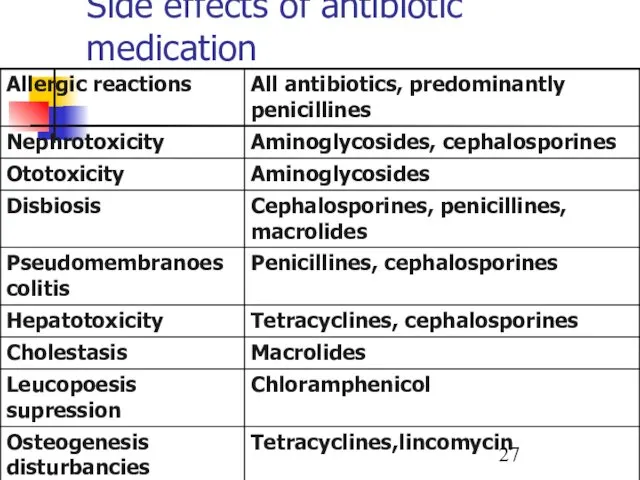
Side effects of antibiotic medication
Side effects of antibiotic medication
Pathogenic treatment
Respiratory supplementation according to respiratory failure
Desintoxication. If indications are
Pathogenic treatment
Respiratory supplementation according to respiratory failure
Desintoxication. If indications are
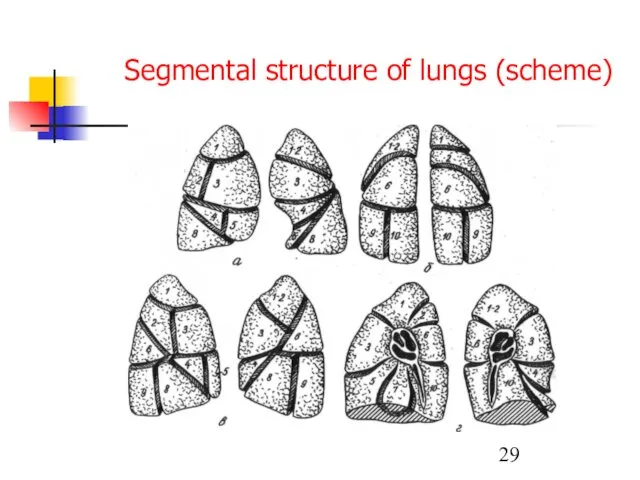
Segmental structure of lungs (scheme)
Segmental structure of lungs (scheme)
Questions
To indicate etiologic and pathophysiologic factors at pneumonia in children
To classify
Questions
To indicate etiologic and pathophysiologic factors at pneumonia in children
To classify
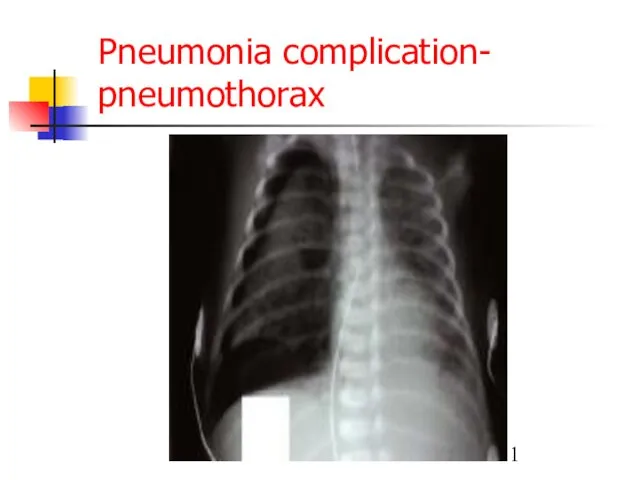
Pneumonia complication- pneumothorax
Pneumonia complication- pneumothorax



 АФО иммунной системы у детей. Методы оценки иммунной системы. Аллергодиагностика у детей. Бронхиальная астма
АФО иммунной системы у детей. Методы оценки иммунной системы. Аллергодиагностика у детей. Бронхиальная астма Респираторный дистресс-синдром
Респираторный дистресс-синдром Железодефицитная анемия и беременность
Железодефицитная анемия и беременность ИБС. Стенокардия
ИБС. Стенокардия Инфильтративный туберкулез легких
Инфильтративный туберкулез легких Жедел бүйрек жетіспеушілігінің клиникалық көріністері
Жедел бүйрек жетіспеушілігінің клиникалық көріністері Парентеральное питание
Парентеральное питание Универсальный алгоритм оказания первой помощи
Универсальный алгоритм оказания первой помощи Гострі пневмонії у дітей. Етіологія, патогенез. Класифікація. Клінічні форми. Лікування гострих пневмоній у дітей
Гострі пневмонії у дітей. Етіологія, патогенез. Класифікація. Клінічні форми. Лікування гострих пневмоній у дітей Заболевания губ у детей
Заболевания губ у детей Репродуктивная система мужчины и женщины в зрелом возрасте
Репродуктивная система мужчины и женщины в зрелом возрасте Зубо-щелепні деформації
Зубо-щелепні деформації Неотложные соматические состояния у тяжелых нетранспортабельных больных
Неотложные соматические состояния у тяжелых нетранспортабельных больных Вирусы. Бактериофаги. ВИЧ-инфекция
Вирусы. Бактериофаги. ВИЧ-инфекция Классификация дизонтогенеза. Поврежденное развитие
Классификация дизонтогенеза. Поврежденное развитие Косметичні засоби
Косметичні засоби Инструментальные методы исследования в гинекологии
Инструментальные методы исследования в гинекологии Гельминтоздар
Гельминтоздар Когнитивно-поведенческое направление психотерапии
Когнитивно-поведенческое направление психотерапии Беременность и язвенная болезнь
Беременность и язвенная болезнь Первичная и вторичная профилактика депрессий у лиц пожилого возраста на базе геронтологического центра
Первичная и вторичная профилактика депрессий у лиц пожилого возраста на базе геронтологического центра Лимфоидная система, как основа приобретенного антигенспецифического иммунитета
Лимфоидная система, как основа приобретенного антигенспецифического иммунитета Аутоиммунные заболевания
Аутоиммунные заболевания Регенерация. Виды репаративной регенерации
Регенерация. Виды репаративной регенерации Национальный календарь прививок
Национальный календарь прививок Нейроинфекции. Виды нейроинфекций
Нейроинфекции. Виды нейроинфекций Минимальды өзгеріс ауруларының емі
Минимальды өзгеріс ауруларының емі Colonic Polyps
Colonic Polyps