- Segmental Stability of The Cervical Spine

Содержание
- 2. Cervical Spine Muscles
- 3. Neck Flexors Superficial Sternocleidomastoid Scalenes Supra-hyoid muscles Infrahyoid musles Deep Longus Colli Longus Capitus Rectus Capitus
- 4. Deep neck flexors Deep Attach directly to the vertebrae Single segments Close to axis of rotation
- 5. Longus colli and capitus
- 6. Longus colli and capitus
- 7. Superficial Neck Flexors Predominantly Mobilisers Also lateral flexion and rotation Hyoid muscles also control hyoid movement
- 8. Superficial Neck Flexors
- 9. Scalenes
- 10. Lateral neck
- 11. Sternocleido-mastoid
- 12. Sternocleido-mastoid
- 14. Neck Extensors Deep Extensors Spinales Semispinalis Rotators Intertransversarii Interspinales Suboccipital extensors Multifidus Superficial Extensors Upper trapezius
- 15. The extensors
- 16. Sub-Occipital Extensors ( upper cervical spine) Rectus Capitus posterior major and minor Occiput to C1 and
- 17. Upper cervical extensors Bilaterally upper cervical extension . Mainly work to control excessive upper cervical flexion.
- 18. Deep neck extensors ( mid to low cervical spine) Eccentric action to control movement Proprioceptive role
- 19. Deep neck extensors Segmental control of extension mid to lower cervical spine Limit and control excessive
- 20. Mobility Muscles Splenius mastoid to C4-T3 Slenius cervicus TP C1-2 to Sp T4-6 Longissimus capitus Mastoid
- 21. Superficial Extensors Upper and lower cervical extension Not segmental Ipsilateral rotation and lateral flexion without segmental
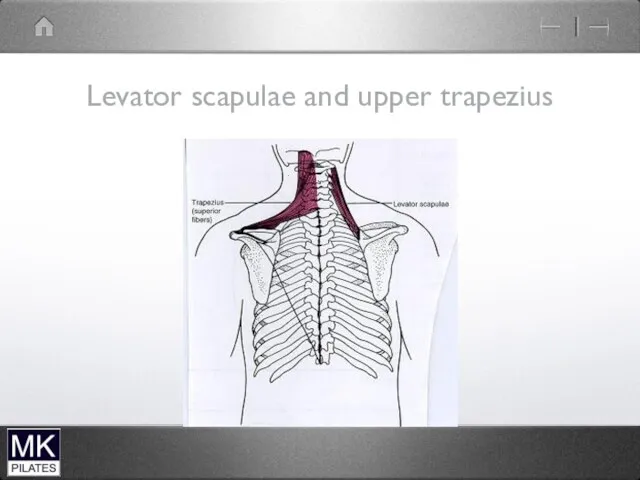
- 22. Upper Trapezius and levator Scapulae
- 23. Trapezius
- 24. Levator Scapulae and Upper Trapezius Mainly mobility of scapula Can also produce Neck extension and lateral
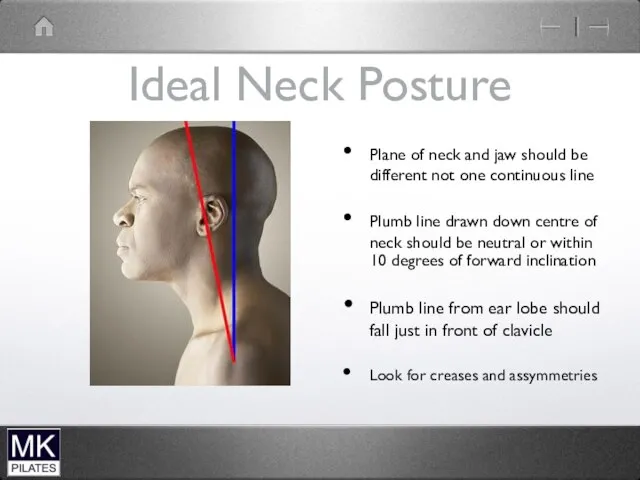
- 25. Ideal Neck Posture Plane of neck and jaw should be different not one continuous line Plumb
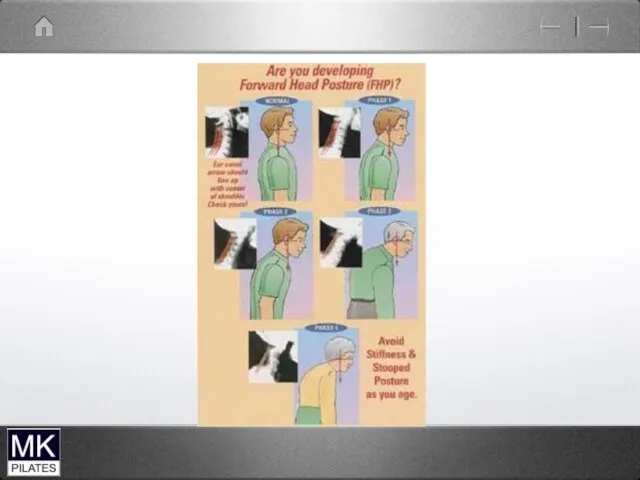
- 26. Common Posture types Chin Poke ( upper cervical spine) Forward head ( lower cervical spine) Forward
- 27. Work posture
- 28. Chin Poke upper cervical spine Short/overactive muscles -Sterno cleido mastoid-suboccipital extensors Weak /lengthened muscles -deep neck
- 29. Chin Poke
- 30. Forward Head lower cervical spine Short overactive muscles -scalenes Weak/lengthened muscles -Deep neck flexors - Deep
- 32. Forward Head Posture
- 35. Make best use of office space
- 36. Occupational therapy for patients can be used creatively to ease the A&C shortages
- 37. Correcting neck posture
- 38. Upper cervical Flexors
- 40. Cervical flexion test-supine Lead with chin…..dominant sterno-cleidomastoid Over flexion upper cervical spine …overactive scalenes Clenching of
- 42. The Shoulder Complex
- 43. 4 joints The glenohumeral joint The acromioclavicular joint The Sternoclavicular joint The Scapulothoracic articulation
- 46. Typical synovial joint
- 47. The glenohumeral joint Ball and socket synovial joint Large humeral head Small glenoid fossa Stability sacrificed
- 48. Humerus
- 49. Glenoid fossa (scapula)
- 50. The shoulder
- 51. Gleno-humeral movement Flexion Extension Internal (medial) Rotation External (lateral) Rotation Abduction Adduction
- 52. The Acromioclavicular joint Small plane joint The lateral end of the clavicle and the acromion process
- 53. Acomioclavicular joint
- 54. Acromioclavicular joint sprain Fall onto point of shoulder. Sprain or disruption of the acromio-clavicular ligaments Grade
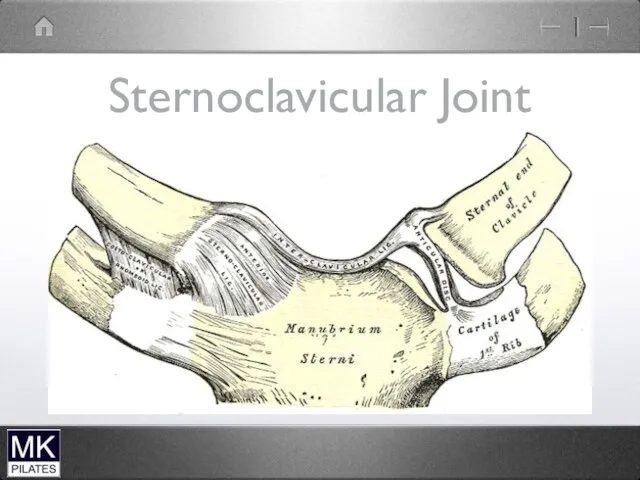
- 55. The Sternoclavicular joint Small fibrous plane joint Between the medial end of the clavicle and the
- 56. Sternoclavicular Joint
- 57. The Scapulothoracic articulation Not a true synovial joint Allows the scapula to glide around the thoracic
- 59. Scapulohumeral rhythm During 180 degrees of arm elevation 2:1 ratio of humeral to scapula movement -120
- 60. Scapulohumeral rhythm Phase 1 - 30 degrees GH abduction - minimal scapula movement Phase 2 and
- 63. Rotator cuff MRI
- 64. Impingement Syndrome Structures between the humerus and the acromion can become compressed and pinched during elevation
- 66. Biomechanical risk factors Internal rotation of the shoulder during elevation Secondary impingement due to reversed scapulohumeral
- 67. Bone spur
- 68. X-ray sub-acromial spur
- 70. Injections
- 71. Glenohumeral Instability Excessive translation of the large humeral head on the relatively small glenoid due to
- 72. Gleno-humeral dislocation
- 73. Frozen Shoulder Frozen shoulder is characterised by progressive pain and stiffness in the glenohumeral joint Can
- 74. Frozen Shoulder stages Stage 1 Progressive and severe pain. Little stiffness Stage 11 Plateau in pain
- 75. Fractured clavicle
- 76. Stabilisation for fractured clavicle
- 77. Fractured clavicle
- 79. Shoulder muscle stability
- 80. Role of The Scapula Provides base for muscle attachment Allows the glenoid to upwardly rotate therefore
- 81. Trunk to Humerus Latissimus Dorsi Pectoralis Major
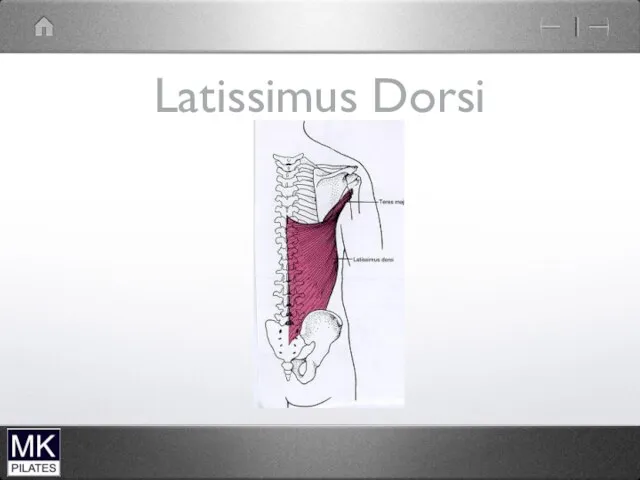
- 82. Latissimus Dorsi O- spinous processes of T6-12; iliac crest; 3 lower ribs and interdigitates with external
- 83. Pectoralis Major O- sternal end of clavicle; strenum; external oblique;rib cartilages 2-6 I- greater tubercle of
- 84. Latissimus Dorsi
- 85. Trunk to Shoulder Complex Pectoralis Minor Trapezius Levator Scapula Rhomboids Serratus Anterior
- 86. Pectoralis Minor O- Ribs 3-5 I- Coracoid process of scapular A- Downward rotation scapula; depresses shoulder;
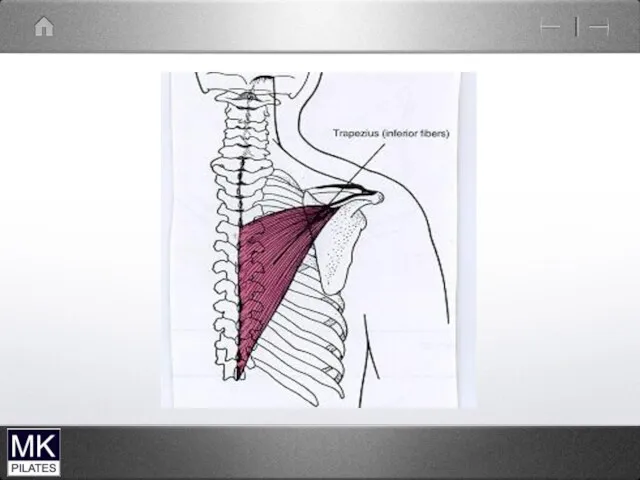
- 87. Trapezius Upper; Middle ;Lower. O- Occiput; spinous processes C7-12 I- lateral 1/3 of clavicle; acromion; spine
- 90. Levator Scapulae O- C1-4 I- vertebral border of scapula A- scapular elevation; scapular elevation
- 91. Rhomboids Major and Minor O- spinous processes C7 to T5 I- root of spine of scapula
- 92. Serratus Anterior O- Fleshy digitations from upper 9 ribs I- Medial border of scapula (interdigitates with
- 93. Scapula to Humerus Supraspinatus Infraspinatus Teres Minor Subscapularis Deltoid Coracobrachialis Teres Major Biceps (long head) Triceps(long
- 94. Teres Major O- post surface of inferior angle of scapular I- lesser tubercle of humerus A
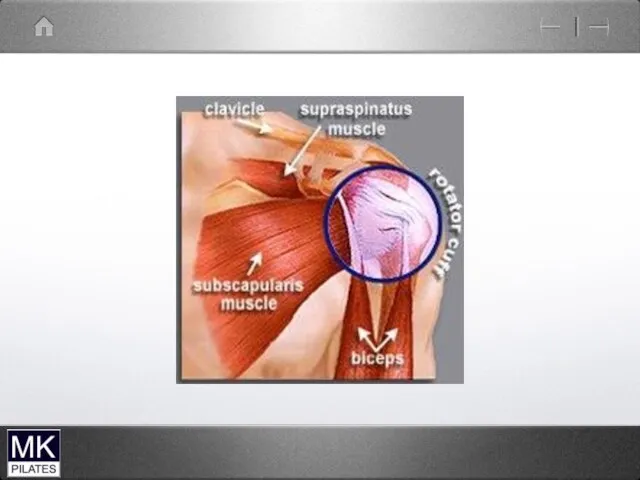
- 95. Rotator Cuff Supraspinatus Infraspinatus Teres Minor Subscapularis
- 96. Supraspinatus O- supraspinous fossa of scapula I- Greater tubercle of humerus A- GH Abduction prevents superior
- 97. Infraspinatus and Teres Minor O- infraspinous fossa scapula I- greater tubercle of humerus A- GH external
- 98. Subscapularis O- Subscapular fossa I- lesser tubercle of humerus A-GH internal rotation prevents anterior translation
- 101. Biceps
- 102. Levator scapulae and upper trapezius
- 103. Scapular stabilisers Serratus anterior protracts the scapula upward rotation of the glenoid Trapezius Upper and Middle
- 104. Scapula Mobility Muscles Levator Scapulae -scapula elevation -glenoid downward rotation Pectoralis minor -glenoid downward rotation -pseudo
- 105. Glenohumeral Stability Supraspinatus - abduction - resists anterior translation Infraspinatus and Teres Minor - external rotation
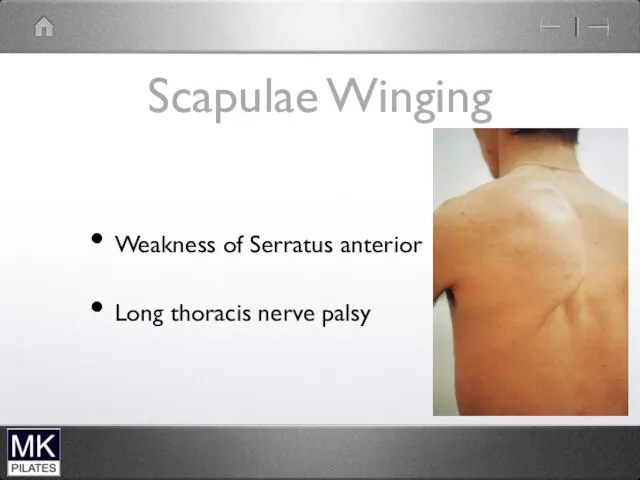
- 106. Scapulae Winging Weakness of Serratus anterior Long thoracis nerve palsy
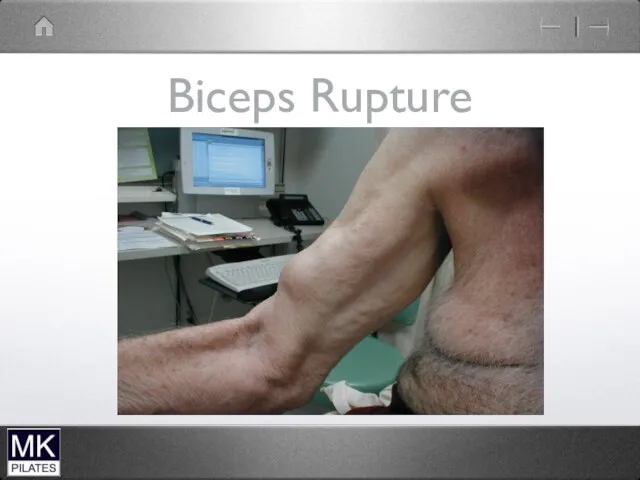
- 107. Biceps Rupture
- 116. The to do list gets longer
- 118. Скачать презентацию
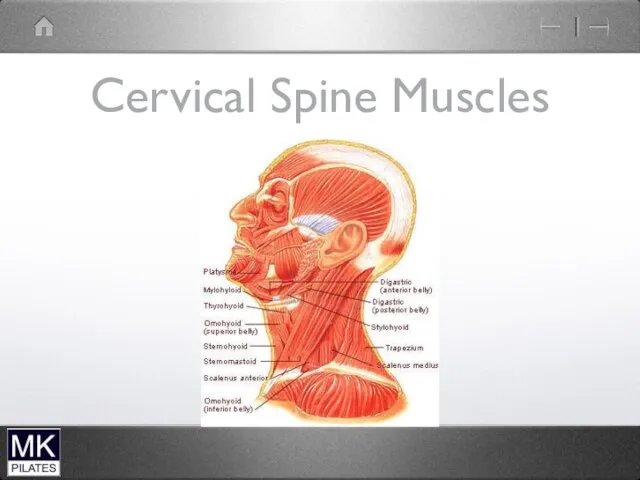
Cervical Spine Muscles
Cervical Spine Muscles
Neck Flexors
Superficial
Sternocleidomastoid
Scalenes
Supra-hyoid muscles
Infrahyoid musles
Deep
Longus Colli
Longus Capitus
Rectus Capitus Anterior
Rectus Capitus Lateralis
Neck Flexors
Superficial
Sternocleidomastoid
Scalenes
Supra-hyoid muscles
Infrahyoid musles
Deep
Longus Colli
Longus Capitus
Rectus Capitus Anterior
Rectus Capitus Lateralis
Deep neck flexors
Deep
Attach directly to the vertebrae
Single segments
Close to axis of
Deep neck flexors
Deep
Attach directly to the vertebrae
Single segments
Close to axis of
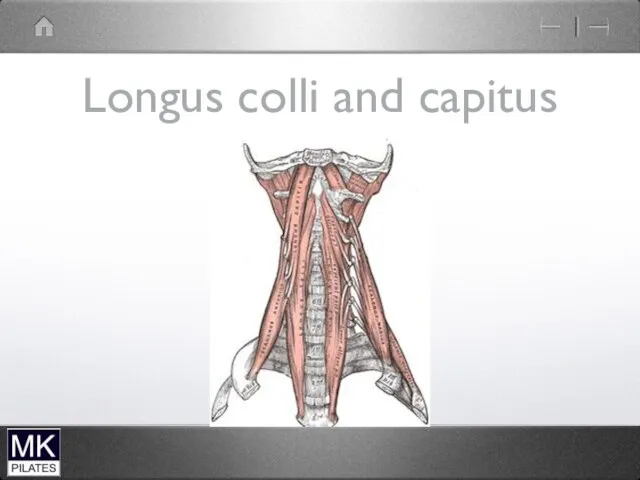
Longus colli and capitus
Longus colli and capitus
Longus colli and capitus
Longus colli and capitus
Superficial Neck Flexors
Predominantly Mobilisers
Also lateral flexion and rotation
Hyoid muscles also control
Superficial Neck Flexors
Predominantly Mobilisers
Also lateral flexion and rotation
Hyoid muscles also control
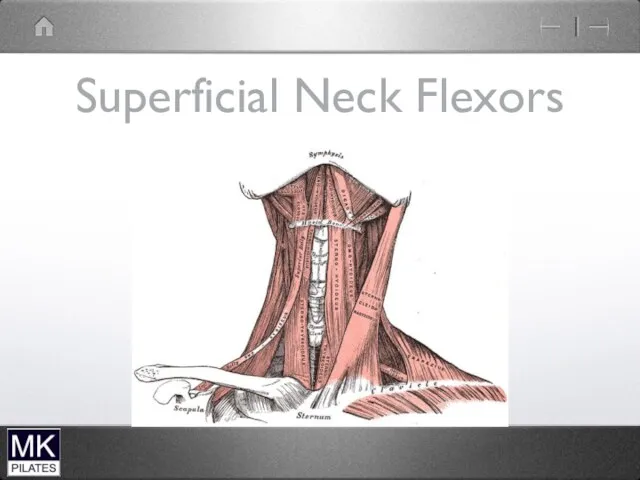
Superficial Neck Flexors
Superficial Neck Flexors
Scalenes
Scalenes
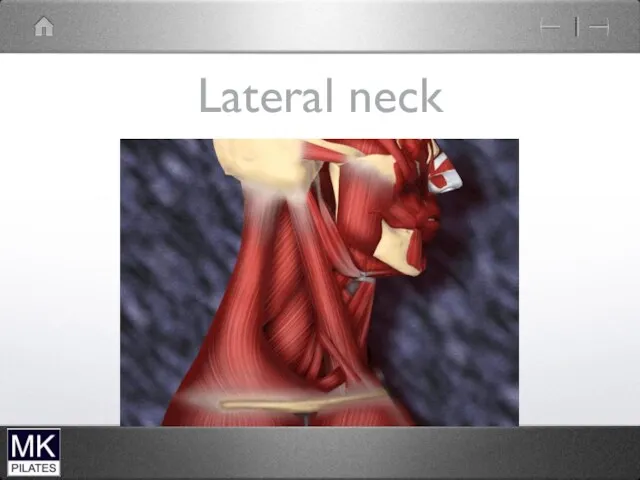
Lateral neck
Lateral neck
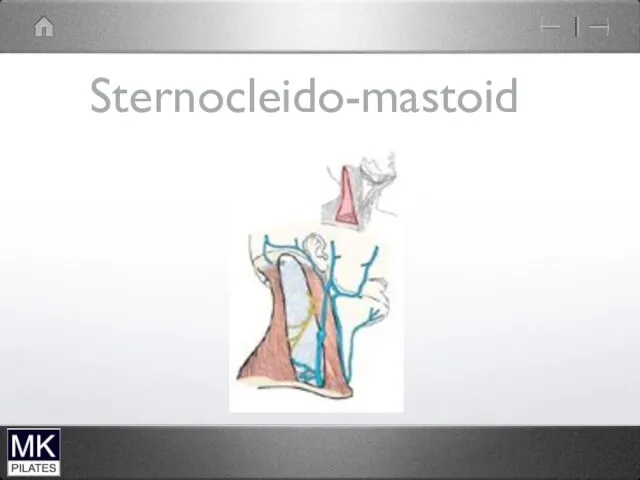
Sternocleido-mastoid
Sternocleido-mastoid
Sternocleido-mastoid
Sternocleido-mastoid

Neck Extensors
Deep Extensors
Spinales
Semispinalis
Rotators
Intertransversarii
Interspinales
Suboccipital extensors
Multifidus
Superficial Extensors
Upper trapezius
Levator scapulae
Splenius
Longisimus
Neck Extensors
Deep Extensors
Spinales
Semispinalis
Rotators
Intertransversarii
Interspinales
Suboccipital extensors
Multifidus
Superficial Extensors
Upper trapezius
Levator scapulae
Splenius
Longisimus
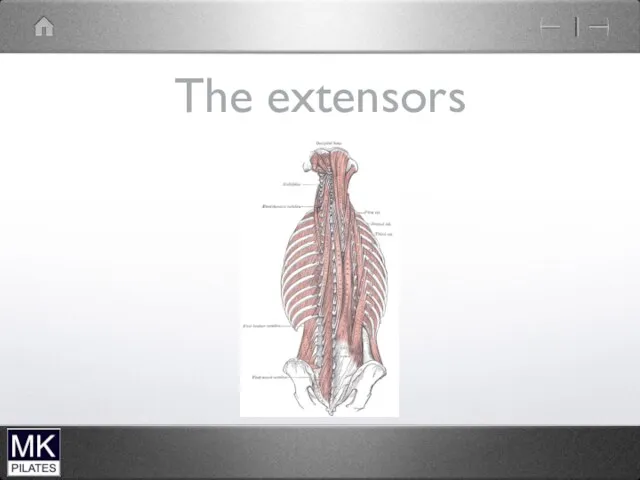
The extensors
The extensors
Sub-Occipital Extensors
( upper cervical spine)
Rectus Capitus posterior major and minor
Occiput
Sub-Occipital Extensors
( upper cervical spine)
Rectus Capitus posterior major and minor
Occiput
Upper cervical extensors
Bilaterally upper cervical extension . Mainly work to control
Upper cervical extensors
Bilaterally upper cervical extension . Mainly work to control
Deep neck extensors
( mid to low cervical spine)
Eccentric action to control
Deep neck extensors
( mid to low cervical spine)
Eccentric action to control
Deep neck extensors
Segmental control of extension mid to lower cervical spine
Limit
Deep neck extensors
Segmental control of extension mid to lower cervical spine
Limit
Mobility Muscles
Splenius mastoid to C4-T3
Slenius cervicus TP C1-2 to Sp T4-6
Longissimus
Mobility Muscles
Splenius mastoid to C4-T3
Slenius cervicus TP C1-2 to Sp T4-6
Longissimus
Superficial Extensors
Upper and lower cervical extension
Not segmental
Ipsilateral rotation and lateral
Superficial Extensors
Upper and lower cervical extension
Not segmental
Ipsilateral rotation and lateral
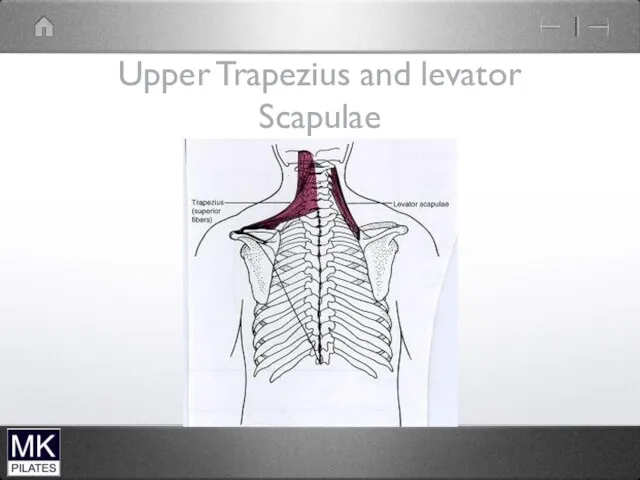
Upper Trapezius and levator Scapulae
Upper Trapezius and levator Scapulae
Trapezius
Trapezius
Levator Scapulae and Upper Trapezius
Mainly mobility of scapula
Can also produce Neck
Levator Scapulae and Upper Trapezius
Mainly mobility of scapula
Can also produce Neck
Ideal Neck Posture
Plane of neck and jaw should be different not
Ideal Neck Posture
Plane of neck and jaw should be different not
Common Posture types
Chin Poke ( upper cervical spine)
Forward head ( lower
Common Posture types
Chin Poke ( upper cervical spine)
Forward head ( lower
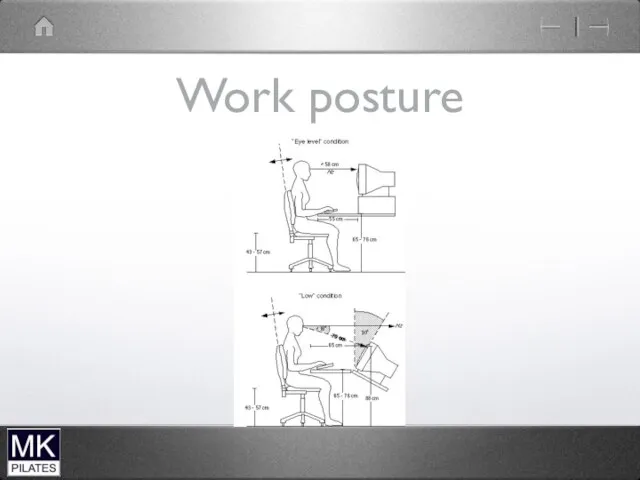
Work posture
Work posture
Chin Poke
upper cervical spine
Short/overactive muscles
-Sterno cleido mastoid-suboccipital extensors
Weak /lengthened muscles
-deep neck
Chin Poke
upper cervical spine
Short/overactive muscles
-Sterno cleido mastoid-suboccipital extensors
Weak /lengthened muscles
-deep neck
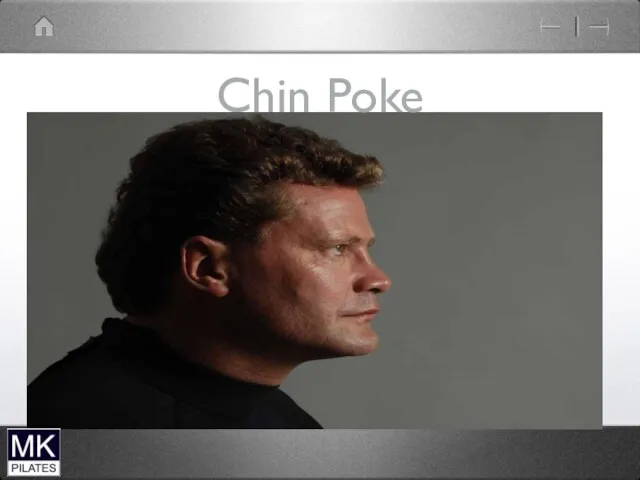
Chin Poke
Chin Poke
Forward Head
lower cervical spine
Short overactive muscles
-scalenes
Weak/lengthened muscles
-Deep neck flexors
- Deep neck
Forward Head
lower cervical spine
Short overactive muscles
-scalenes
Weak/lengthened muscles
-Deep neck flexors
- Deep neck
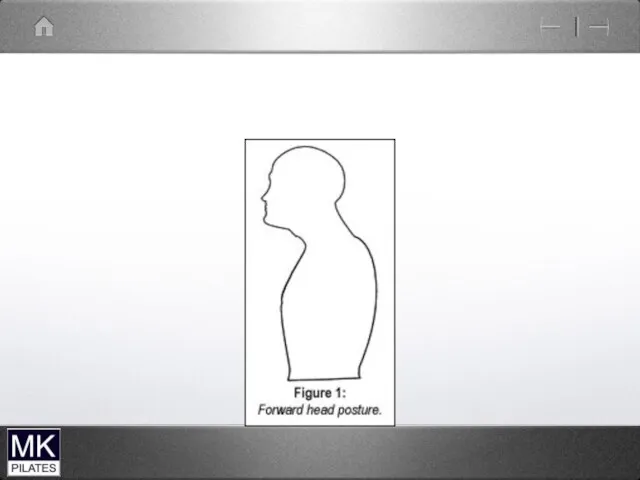
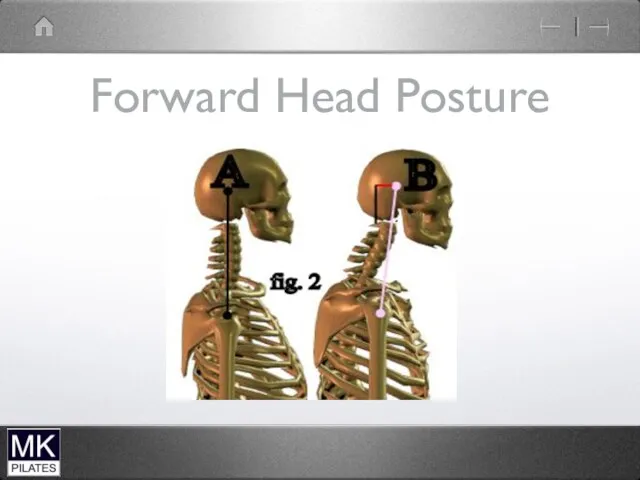
Forward Head Posture
Forward Head Posture


Make best use of office space
Make best use of office space
Occupational therapy for patients can be used creatively to ease the
Occupational therapy for patients can be used creatively to ease the
Correcting neck posture
Correcting neck posture
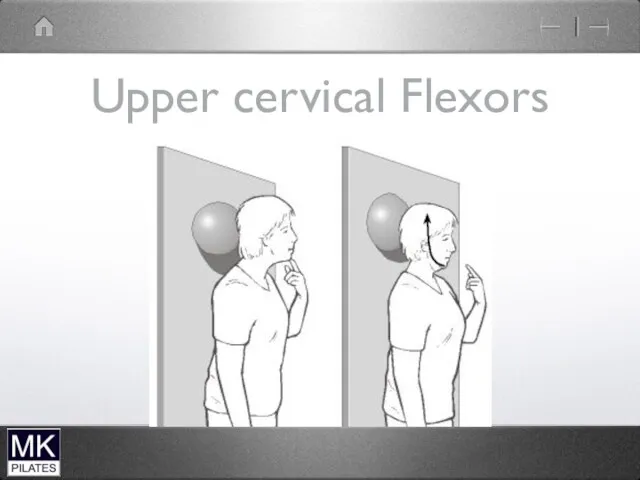
Upper cervical Flexors
Upper cervical Flexors

Cervical flexion test-supine
Lead with chin…..dominant sterno-cleidomastoid
Over flexion upper cervical spine …overactive
Cervical flexion test-supine
Lead with chin…..dominant sterno-cleidomastoid
Over flexion upper cervical spine …overactive

The Shoulder Complex
The Shoulder Complex
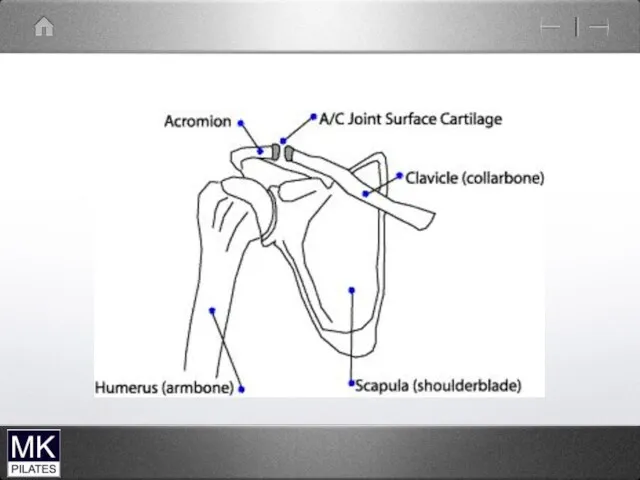
4 joints
The glenohumeral joint
The acromioclavicular joint
The Sternoclavicular joint
The Scapulothoracic articulation
4 joints
The glenohumeral joint
The acromioclavicular joint
The Sternoclavicular joint
The Scapulothoracic articulation
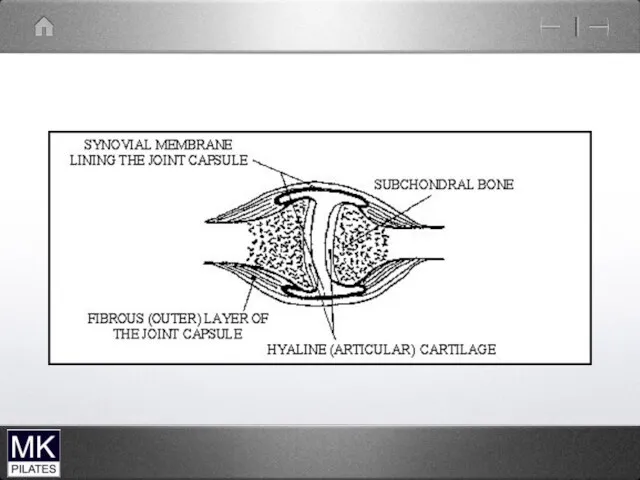
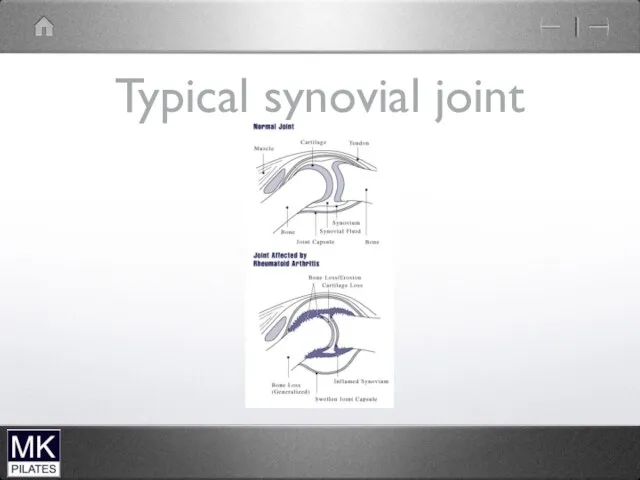
Typical synovial joint
Typical synovial joint
The glenohumeral joint
Ball and socket synovial joint
Large humeral head
Small glenoid fossa
Stability
The glenohumeral joint
Ball and socket synovial joint
Large humeral head
Small glenoid fossa
Stability
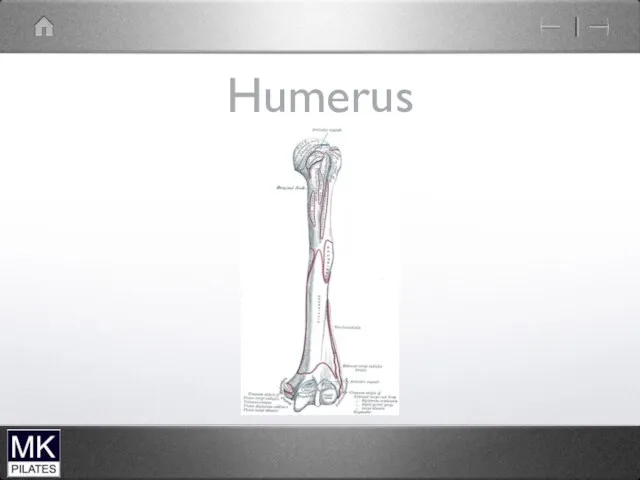
Humerus
Humerus
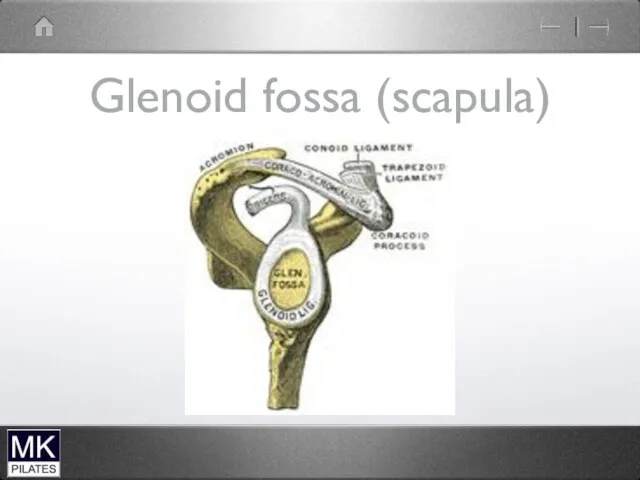
Glenoid fossa (scapula)
Glenoid fossa (scapula)
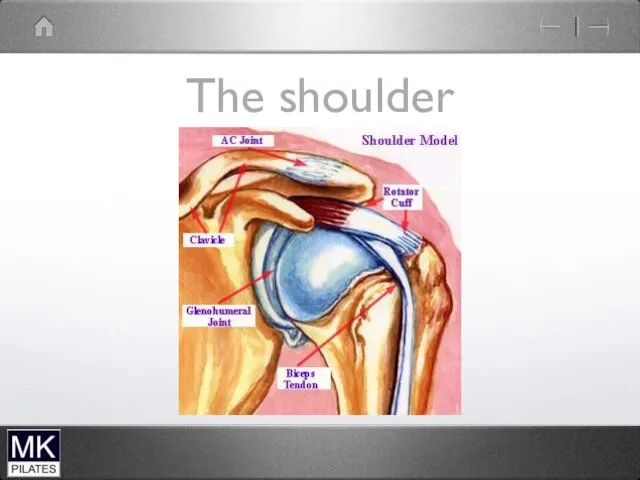
The shoulder
The shoulder
Gleno-humeral movement
Flexion
Extension
Internal (medial) Rotation
External (lateral) Rotation
Abduction
Adduction
Gleno-humeral movement
Flexion
Extension
Internal (medial) Rotation
External (lateral) Rotation
Abduction
Adduction
The Acromioclavicular joint
Small plane joint
The lateral end of the clavicle and
The Acromioclavicular joint
Small plane joint
The lateral end of the clavicle and
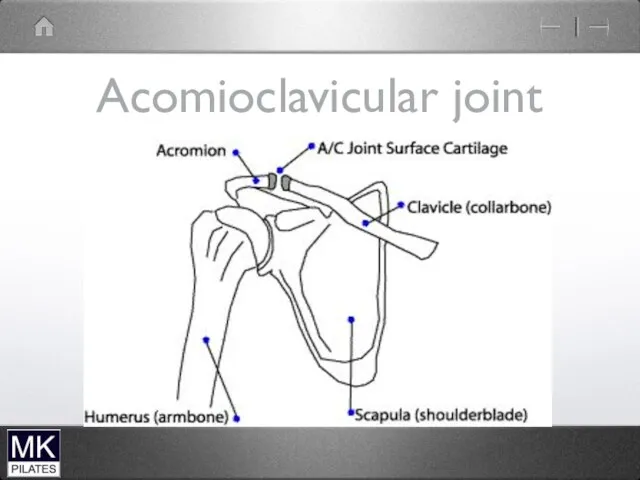
Acomioclavicular joint
Acomioclavicular joint
Acromioclavicular joint sprain
Fall onto point of shoulder.
Sprain or disruption of the
Acromioclavicular joint sprain
Fall onto point of shoulder.
Sprain or disruption of the
The Sternoclavicular joint
Small fibrous plane joint
Between the medial end of the
The Sternoclavicular joint
Small fibrous plane joint
Between the medial end of the
Sternoclavicular Joint
Sternoclavicular Joint
The Scapulothoracic articulation
Not a true synovial joint
Allows the scapula to glide
The Scapulothoracic articulation
Not a true synovial joint
Allows the scapula to glide

Scapulohumeral rhythm
During 180 degrees of arm elevation
2:1 ratio of humeral to
Scapulohumeral rhythm
During 180 degrees of arm elevation
2:1 ratio of humeral to
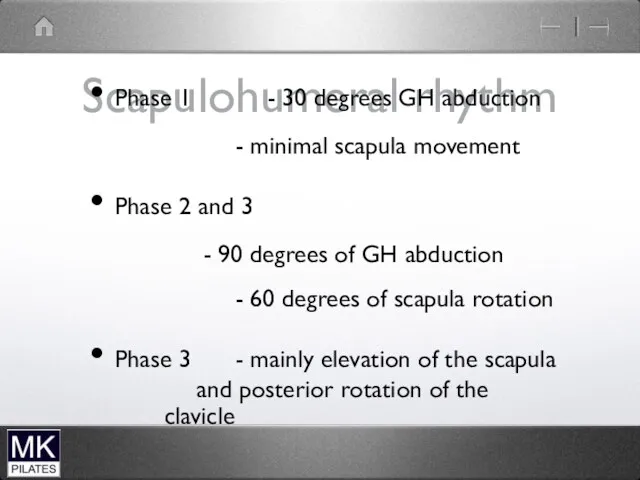
Scapulohumeral rhythm
Phase 1 - 30 degrees GH abduction
- minimal scapula
Scapulohumeral rhythm
Phase 1 - 30 degrees GH abduction
- minimal scapula

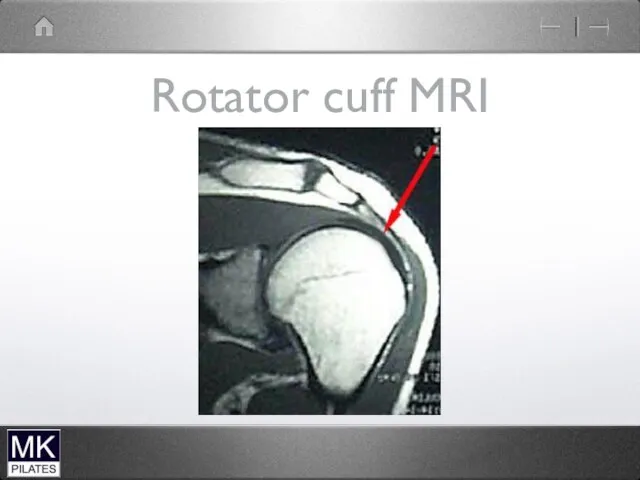
Rotator cuff MRI
Rotator cuff MRI
Impingement Syndrome
Structures between the humerus and the acromion can become compressed
Impingement Syndrome
Structures between the humerus and the acromion can become compressed

Biomechanical risk factors
Internal rotation of the shoulder during elevation
Secondary impingement due
Biomechanical risk factors
Internal rotation of the shoulder during elevation
Secondary impingement due
Bone spur
Bone spur
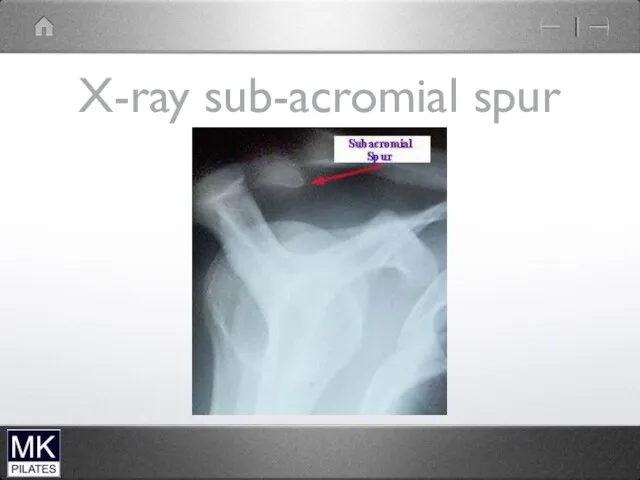
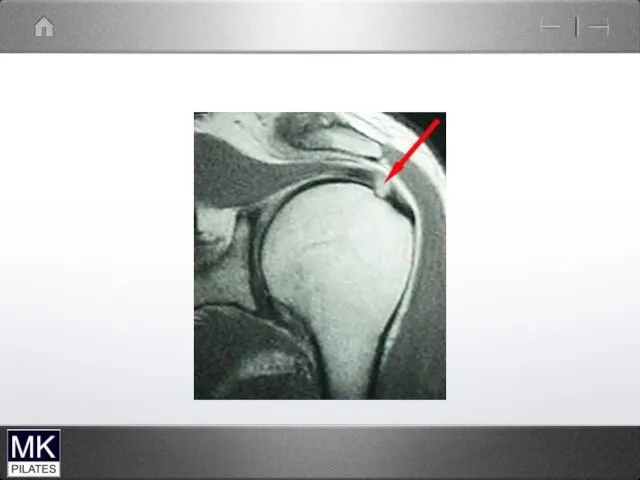
X-ray sub-acromial spur
X-ray sub-acromial spur
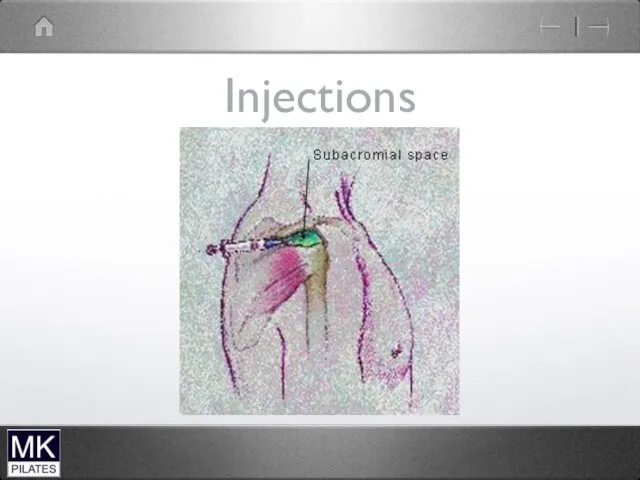
Injections
Injections
Glenohumeral Instability
Excessive translation of the large humeral head on the relatively
Glenohumeral Instability
Excessive translation of the large humeral head on the relatively
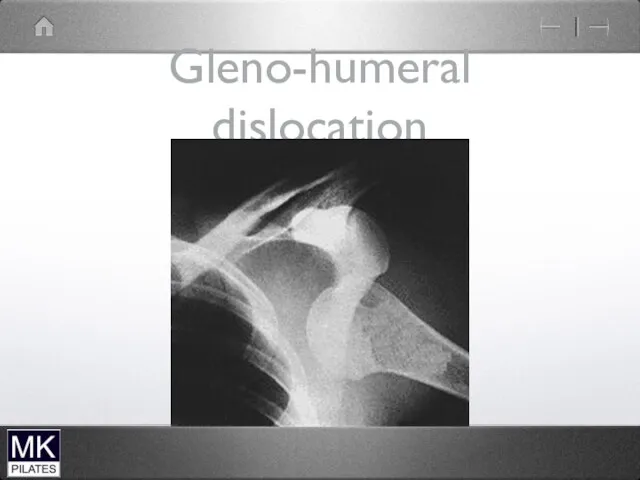
Gleno-humeral dislocation
Gleno-humeral dislocation
Frozen Shoulder
Frozen shoulder is characterised by progressive pain and stiffness in
Frozen Shoulder
Frozen shoulder is characterised by progressive pain and stiffness in
Frozen Shoulder stages
Stage 1 Progressive and severe pain. Little stiffness
Stage 11
Frozen Shoulder stages
Stage 1 Progressive and severe pain. Little stiffness
Stage 11
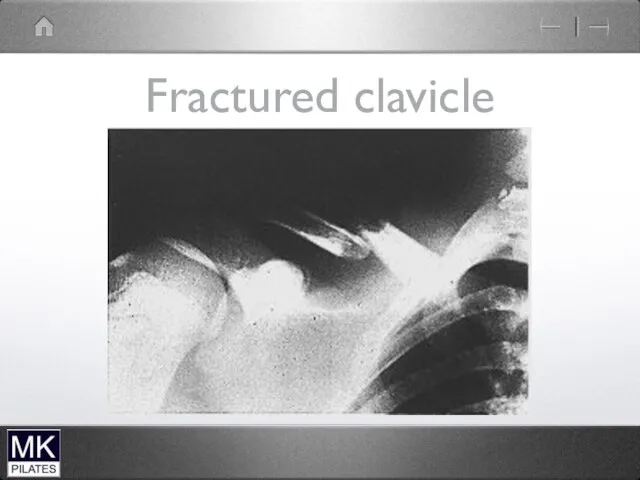
Fractured clavicle
Fractured clavicle
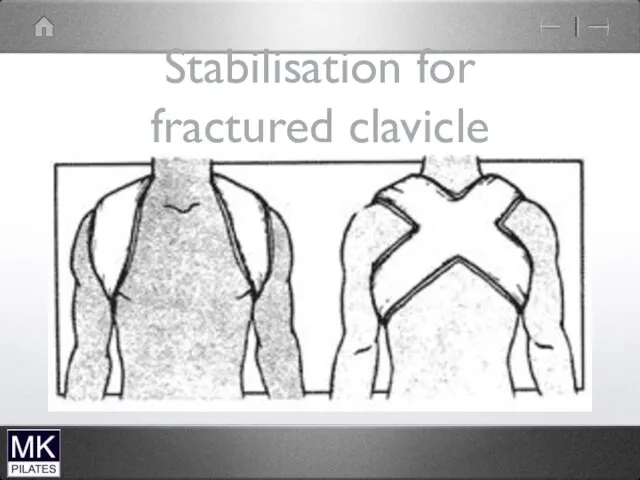
Stabilisation for fractured clavicle
Stabilisation for fractured clavicle
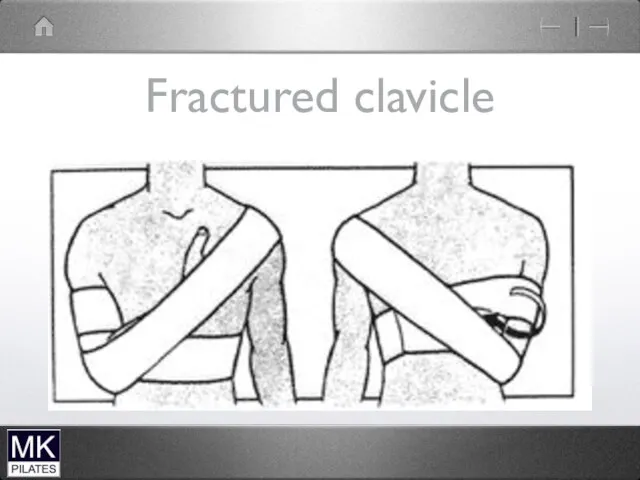
Fractured clavicle
Fractured clavicle

Shoulder muscle stability
Shoulder muscle stability
Role of The Scapula
Provides base for muscle attachment
Allows the glenoid to
Role of The Scapula
Provides base for muscle attachment
Allows the glenoid to
Trunk to Humerus
Latissimus Dorsi
Pectoralis Major
Trunk to Humerus
Latissimus Dorsi
Pectoralis Major
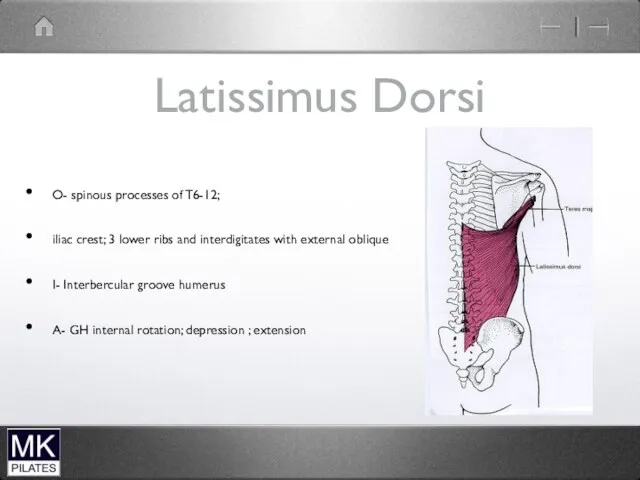
Latissimus Dorsi
O- spinous processes of T6-12;
iliac crest; 3 lower ribs
Latissimus Dorsi
O- spinous processes of T6-12;
iliac crest; 3 lower ribs
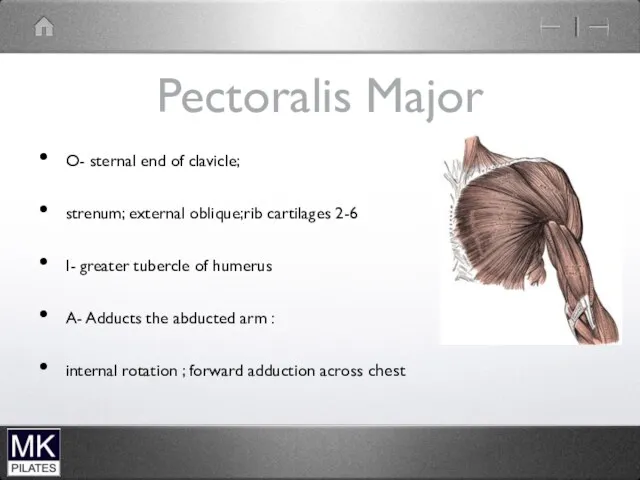
Pectoralis Major
O- sternal end of clavicle;
strenum; external oblique;rib cartilages 2-6
I-
Pectoralis Major
O- sternal end of clavicle;
strenum; external oblique;rib cartilages 2-6
I-
Latissimus Dorsi
Latissimus Dorsi
Trunk to Shoulder Complex
Pectoralis Minor
Trapezius
Levator Scapula
Rhomboids
Serratus Anterior
Trunk to Shoulder Complex
Pectoralis Minor
Trapezius
Levator Scapula
Rhomboids
Serratus Anterior
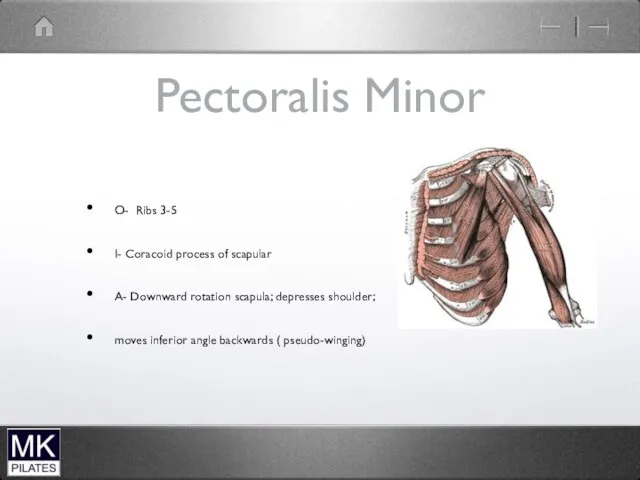
Pectoralis Minor
O- Ribs 3-5
I- Coracoid process of scapular
A- Downward rotation scapula;
Pectoralis Minor
O- Ribs 3-5
I- Coracoid process of scapular
A- Downward rotation scapula;
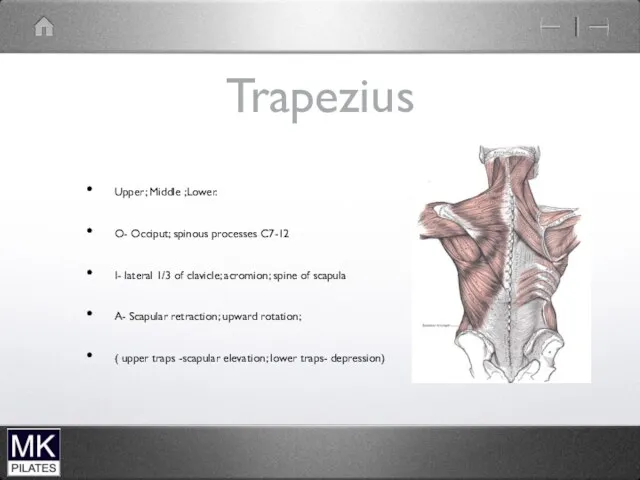
Trapezius
Upper; Middle ;Lower.
O- Occiput; spinous processes C7-12
I- lateral 1/3 of clavicle;
Trapezius
Upper; Middle ;Lower.
O- Occiput; spinous processes C7-12
I- lateral 1/3 of clavicle;

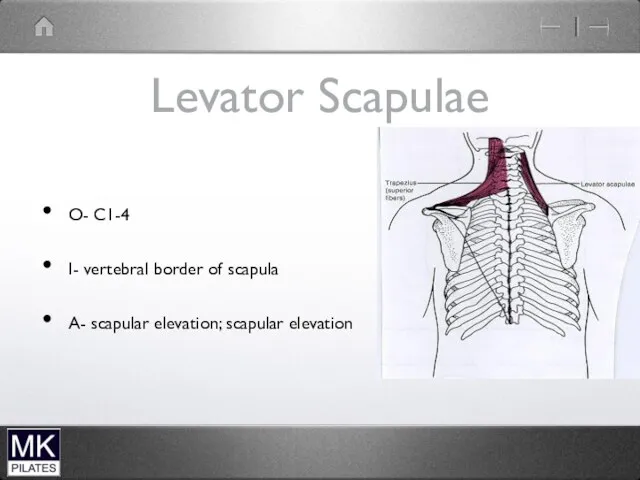
Levator Scapulae
O- C1-4
I- vertebral border of scapula
A- scapular elevation; scapular
Levator Scapulae
O- C1-4
I- vertebral border of scapula
A- scapular elevation; scapular
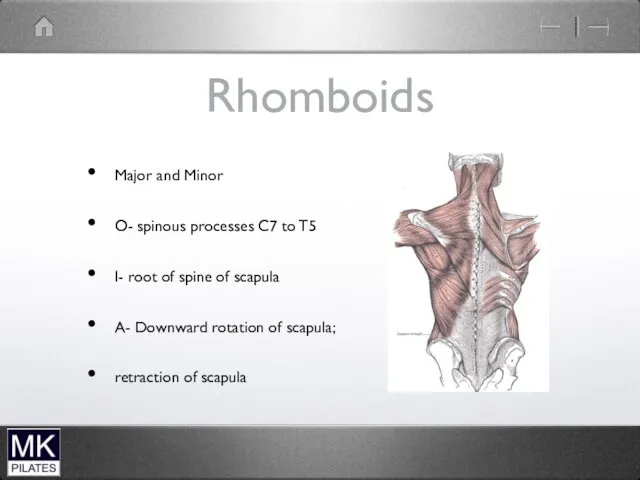
Rhomboids
Major and Minor
O- spinous processes C7 to T5
I- root of
Rhomboids
Major and Minor
O- spinous processes C7 to T5
I- root of
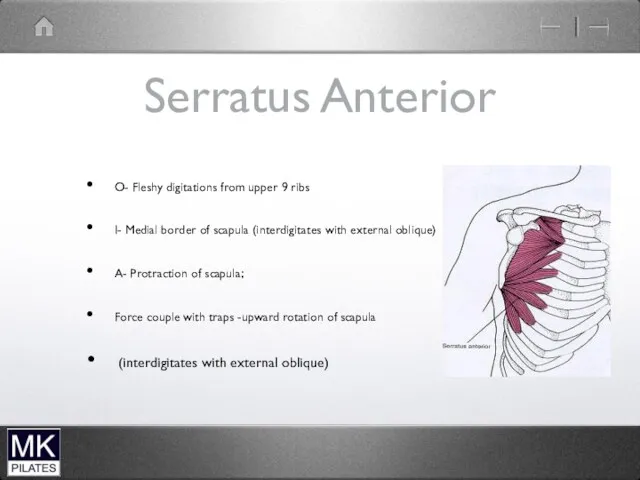
Serratus Anterior
O- Fleshy digitations from upper 9 ribs
I- Medial border of
Serratus Anterior
O- Fleshy digitations from upper 9 ribs
I- Medial border of
Scapula to Humerus
Supraspinatus
Infraspinatus
Teres Minor
Subscapularis
Deltoid
Coracobrachialis
Teres Major
Biceps (long head)
Triceps(long head)
Scapula to Humerus
Supraspinatus
Infraspinatus
Teres Minor
Subscapularis
Deltoid
Coracobrachialis
Teres Major
Biceps (long head)
Triceps(long head)
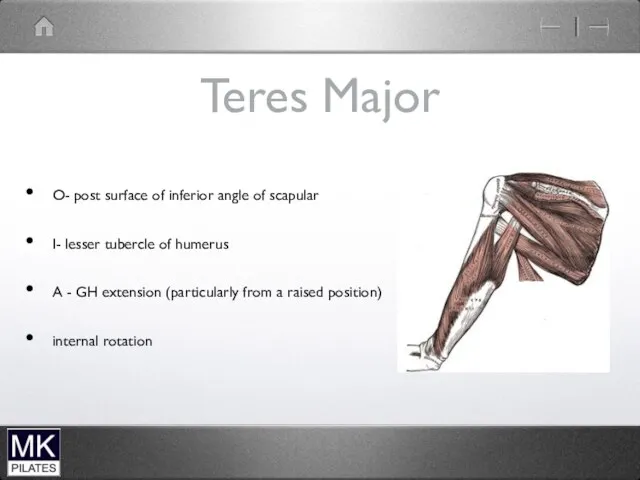
Teres Major
O- post surface of inferior angle of scapular
I- lesser tubercle
Teres Major
O- post surface of inferior angle of scapular
I- lesser tubercle
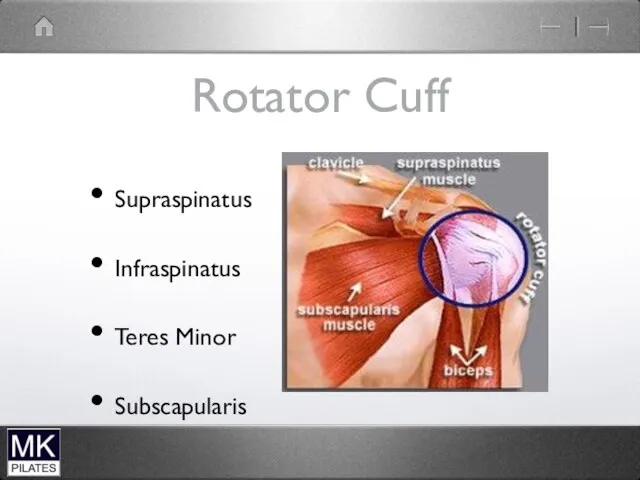
Rotator Cuff
Supraspinatus
Infraspinatus
Teres Minor
Subscapularis
Rotator Cuff
Supraspinatus
Infraspinatus
Teres Minor
Subscapularis
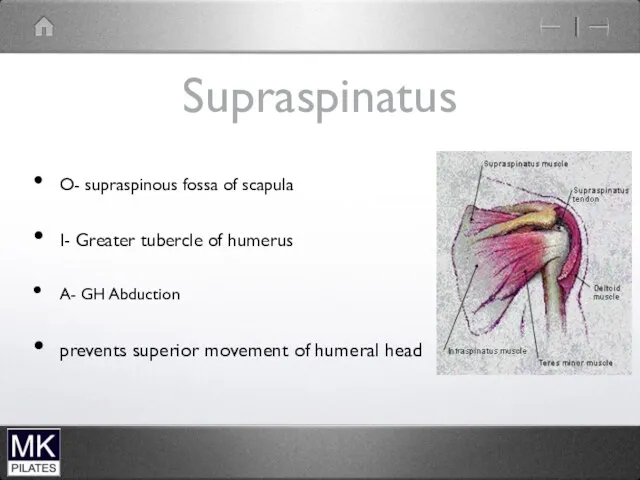
Supraspinatus
O- supraspinous fossa of scapula
I- Greater tubercle of humerus
A- GH Abduction
prevents
Supraspinatus
O- supraspinous fossa of scapula
I- Greater tubercle of humerus
A- GH Abduction
prevents
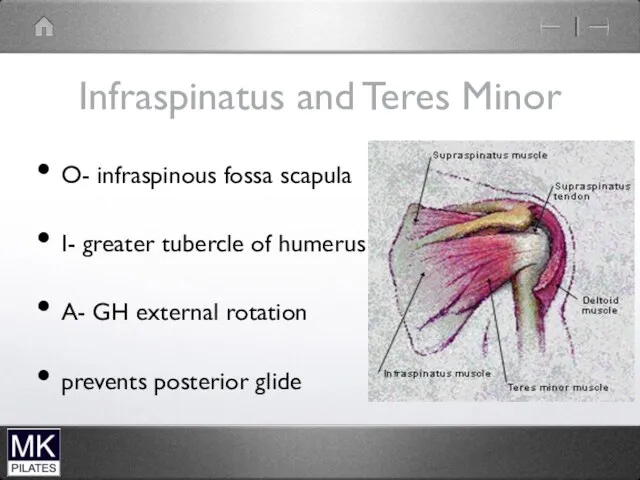
Infraspinatus and Teres Minor
O- infraspinous fossa scapula
I- greater tubercle of humerus
A-
Infraspinatus and Teres Minor
O- infraspinous fossa scapula
I- greater tubercle of humerus
A-
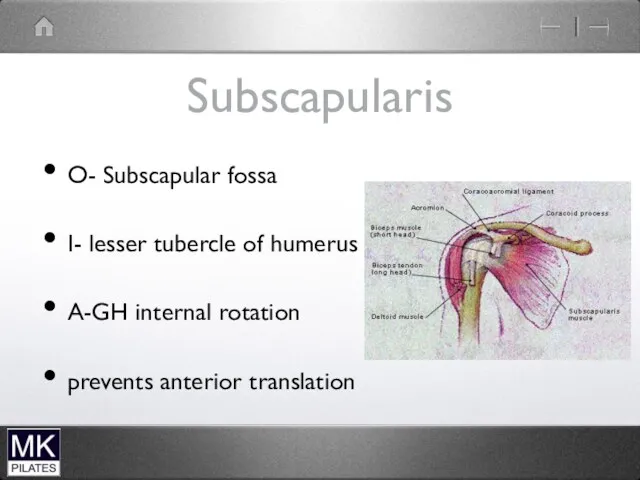
Subscapularis
O- Subscapular fossa
I- lesser tubercle of humerus
A-GH internal rotation
prevents anterior translation
Subscapularis
O- Subscapular fossa
I- lesser tubercle of humerus
A-GH internal rotation
prevents anterior translation


Biceps
Biceps
Levator scapulae and upper trapezius
Levator scapulae and upper trapezius
Scapular stabilisers
Serratus anterior
protracts the scapula
upward rotation of the glenoid
Trapezius
Upper and Middle
Scapular stabilisers
Serratus anterior
protracts the scapula
upward rotation of the glenoid
Trapezius
Upper and Middle
Scapula Mobility Muscles
Levator Scapulae -scapula elevation
-glenoid downward rotation
Pectoralis minor -glenoid downward
Scapula Mobility Muscles
Levator Scapulae -scapula elevation
-glenoid downward rotation
Pectoralis minor -glenoid downward
Glenohumeral Stability
Supraspinatus - abduction
- resists anterior translation
Infraspinatus and Teres Minor
- external
Glenohumeral Stability
Supraspinatus - abduction
- resists anterior translation
Infraspinatus and Teres Minor
- external
Scapulae Winging
Weakness of Serratus anterior
Long thoracis nerve palsy
Scapulae Winging
Weakness of Serratus anterior
Long thoracis nerve palsy
Biceps Rupture
Biceps Rupture





The to do list gets longer
The to do list gets longer
 Подходы в диагностике и лечении болезней перикарда
Подходы в диагностике и лечении болезней перикарда Умирание, смерть и трупные изменения
Умирание, смерть и трупные изменения Нейродегенеративные заболевания
Нейродегенеративные заболевания Жүйке жүйесі
Жүйке жүйесі Патофизиология обмена веществ
Патофизиология обмена веществ Жаңа туған нәрестенің физиологиясы және патологиясы
Жаңа туған нәрестенің физиологиясы және патологиясы Лечение в санаториях Белокурихи
Лечение в санаториях Белокурихи Диспансеризация и диспансерное наблюдение
Диспансеризация и диспансерное наблюдение Отходы медицинских учреждений
Отходы медицинских учреждений Вирусные инфекции кожи и слизистых оболочек
Вирусные инфекции кожи и слизистых оболочек Инфекционная безопасность пациентов ОРИТ
Инфекционная безопасность пациентов ОРИТ Биполярное расстройство I типа
Биполярное расстройство I типа Мировые стандарты оказания неотложной медицинской помощи
Мировые стандарты оказания неотложной медицинской помощи Асептика. Определение асептики
Асептика. Определение асептики Свойства рыбы. Рубрика Какая рыба полезнее?
Свойства рыбы. Рубрика Какая рыба полезнее? Олигофрения: классификация, профилактика, пути коррекции
Олигофрения: классификация, профилактика, пути коррекции Дәлелді медицина бойынша қоғам пікірі. Біздің елде және тмд елдеріндегі дәлелді медицина орталықтары
Дәлелді медицина бойынша қоғам пікірі. Біздің елде және тмд елдеріндегі дәлелді медицина орталықтары Дифференциальный диагноз нефротического синдрома
Дифференциальный диагноз нефротического синдрома Режимы аппаратной (механической) вентиляции лёгких
Режимы аппаратной (механической) вентиляции лёгких Генные заболевания
Генные заболевания ВИЧ-инфекция
ВИЧ-инфекция Гнозис и его расстройства
Гнозис и его расстройства Острые респираторные заболевания у детей
Острые респираторные заболевания у детей Методы исследования сердечно-сосудистой системы
Методы исследования сердечно-сосудистой системы Острая ревматическая лихорадка и тактика ведения больных с ревматическими пороками сердца
Острая ревматическая лихорадка и тактика ведения больных с ревматическими пороками сердца Эндодонтическая система K3 Endo (Kerr)
Эндодонтическая система K3 Endo (Kerr) Гнойно-воспалительные заболевания мягких тканей. Медиастинит
Гнойно-воспалительные заболевания мягких тканей. Медиастинит Қан қозғалысының гемодинамикалық заңдылықтары. Қанның реологиялық қасиеттері
Қан қозғалысының гемодинамикалық заңдылықтары. Қанның реологиялық қасиеттері