- The diseases with tonsilitis. Diphtheria and infectious mononucleosis/

Содержание
- 2. DIPHTHERIA An acute, contagious disease caused by Corynebacterium diphtheriae, characterized by the formation of a fibrinous
- 3. Etiology Three biotypes of C. diphtheriae exist (mitis, intermedius, and gravis) Only toxinogenic isolates produce exotoxin
- 4. Epidemiology Humans are the only known reservoir for C. diphtheriae Spread is chiefly by the secretions
- 5. Pathogenesis the microorganisms lodge in the tonsil or nasopharynx, and multiply toxinogenic C. diphtheriae with produce
- 6. exotoxin, carried by the blood damages cells in distant organs, creating pathologic lesions in the respiratory
- 7. Symptoms and Signs The incubation period ranges between 1 and 4 days Initially, the patient with
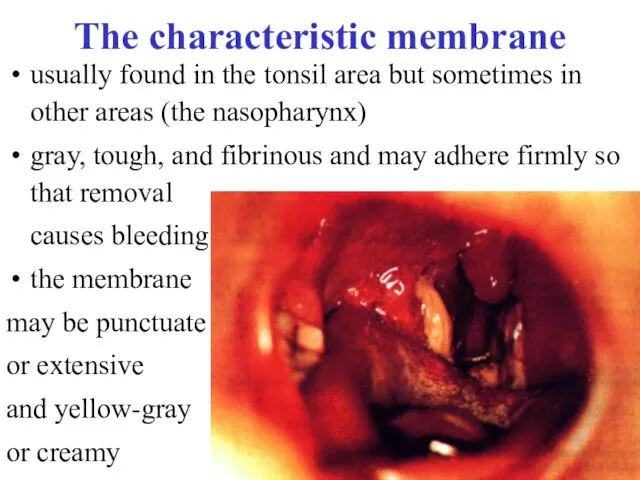
- 8. The characteristic membrane usually found in the tonsil area but sometimes in other areas (the nasopharynx)
- 9. When disease progresses, dysphagia, toxemia, and prostration are prominent The cervical lymph glands are enlarged. Pharyngeal
- 10. In severe cases, exotoxin may diffuse into the neck tissue, producing severe edema (bull neck). The
- 11. Complications Severe complications are likely if antitoxin is not given promptly on the basis of clinical
- 12. Diagnosis The clinical appearance of the membrane suggests the diagnosis, pending confirmation by culture Gram stain
- 13. Material for culture should be obtained from below the membrane, or a portion of membrane itself
- 14. Treatment Diphtheria antitoxin must be given early, since the antitoxin neutralizes only toxin not yet bound
- 15. Administered antitoxin After 20 minutes, you must meter papule too, and if it smaller then 10
- 16. The dose of the antitoxin ranging from 20,000 to 100,000 U, is determined empirically symptomatic diphtheritic
- 17. Antimicrobial treatment is required to eradicate the organism and prevent spread; it is not a substitute
- 18. Prophylaxis Active immunization with diphtheria-tetanus-pertussis (DTP) vaccine should be routinely given to all children and all
- 19. Management of an Outbreak All symptomatic patients should be isolated Contact precautions (private room, use of
- 20. INFECTIOUS MONONUCLEOSIS is an acute disease which, characterized by fever, pharyngitis, and lymphadenopathy and cause Epstein-Barr
- 21. Etiology and Pathophysiology Epstein-Barr virus (EBV) is a herpesvirus with a host range limited primarily to
- 22. Epidemiology EBV is relatively labile and is not very contagious In most cases, the incubation period
- 23. Symptoms and Signs A tetrad of symptoms: fever, pharyngitis, and lymphadenopathy is common; however, patients may
- 24. Lymphadenopathy may involve any group of nodes but is usually symmetric; anterior and posterior cervical adenopathy
- 25. Complications Neurosis complications include encephalitis, Guieain-Barre syndrome, peripheral neuropathy, aseptic meningitis, myelitis, cranial nerve palsies, and
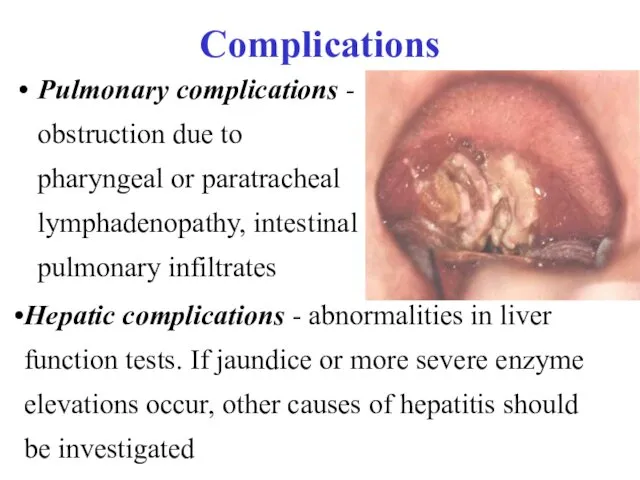
- 26. Complications Pulmonary complications - obstruction due to pharyngeal or paratracheal lymphadenopathy, intestinal pulmonary infiltrates Hepatic complications
- 27. Laboratory Findings and Diagnosis the clinical syndrome of infectious mononucleosis and its epidemiologic setting may be
- 28. resulting from reactive lymphocytes that are morphologically atypical to varying degrees (mononuclear)
- 29. Differential Diagnosis The pharyngitis, lymphadenopathy, and fever may be clinically indistinguishable from that caused by group
- 30. Prognosis Infectious mononucleosis is usually self-limited The duration of the illness varies; the acute phase lasts
- 31. Treatment Patients should be encouraged to rest during the acute phase because of the risk of
- 32. Varicella is an acute infectious disease, characterized by vesicular eruption with transparent liquid on skin and
- 33. Etiology and Epidemiology The Varicella virus contains DNA. Varicella and herpes zoster were proved to be
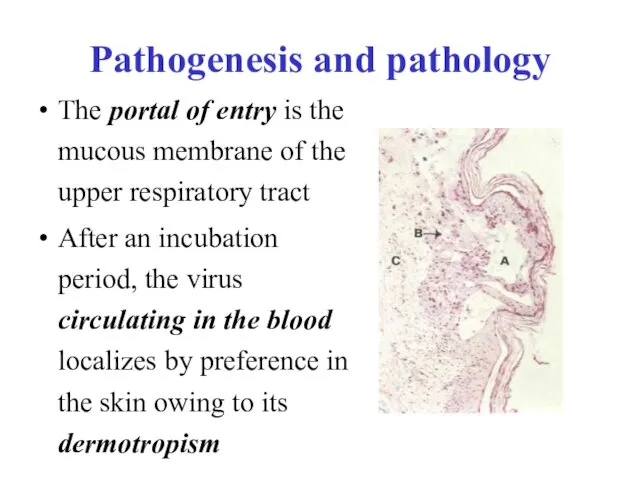
- 34. Pathogenesis and pathology The portal of entry is the mucous membrane of the upper respiratory tract
- 35. In very rare cases the lungs, liver, spleen, kidneys, pancreas, and other internal organs may be
- 36. Clinical manifestations The incubation period averages 11-21 days The outbreak of rash coincides with a rise
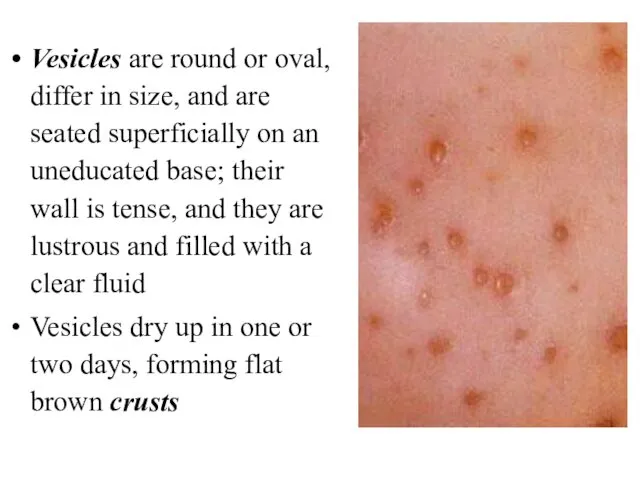
- 37. Vesicles are round or oval, differ in size, and are seated superficially on an uneducated base;
- 38. Atypical forms In the bullous form of varicella large flabby bullae develop (up to two or
- 39. Complications Complications are rare in Varicella: keratitis, laryngitis, abscesses, phlegmons, stomatitis, otitis, lymphadenitis and bronchopneumonia Individual
- 41. Скачать презентацию
DIPHTHERIA
An acute, contagious disease caused by Corynebacterium diphtheriae, characterized by the
DIPHTHERIA
An acute, contagious disease caused by Corynebacterium diphtheriae, characterized by the
Etiology
Three biotypes of C. diphtheriae exist (mitis, intermedius, and gravis)
Only toxinogenic
Etiology
Three biotypes of C. diphtheriae exist (mitis, intermedius, and gravis)
Only toxinogenic
Epidemiology
Humans are the only known reservoir for C. diphtheriae
Spread is
Epidemiology
Humans are the only known reservoir for C. diphtheriae
Spread is
Pathogenesis
the microorganisms lodge in the tonsil or nasopharynx, and multiply
Pathogenesis
the microorganisms lodge in the tonsil or nasopharynx, and multiply
exotoxin, carried by the blood damages cells in distant organs, creating
exotoxin, carried by the blood damages cells in distant organs, creating
Symptoms and Signs
The incubation period ranges between 1 and 4
Symptoms and Signs
The incubation period ranges between 1 and 4
The characteristic membrane
usually found in the tonsil area but sometimes in
The characteristic membrane
usually found in the tonsil area but sometimes in
When disease progresses, dysphagia, toxemia, and prostration are prominent
The cervical lymph
When disease progresses, dysphagia, toxemia, and prostration are prominent
The cervical lymph
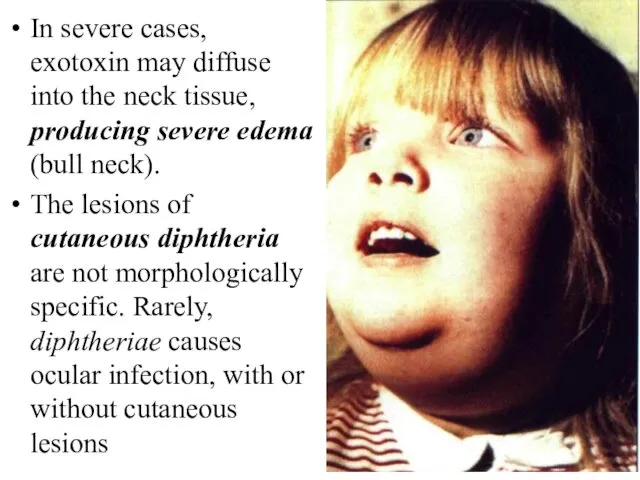
In severe cases, exotoxin may diffuse into the neck tissue, producing
In severe cases, exotoxin may diffuse into the neck tissue, producing
Complications
Severe complications are likely if antitoxin is not given promptly
Complications
Severe complications are likely if antitoxin is not given promptly
Diagnosis
The clinical appearance of the membrane suggests the diagnosis, pending
Diagnosis
The clinical appearance of the membrane suggests the diagnosis, pending
Material for culture should be obtained from below the membrane, or
Material for culture should be obtained from below the membrane, or
Treatment
Diphtheria antitoxin must be given early, since the antitoxin neutralizes
Treatment
Diphtheria antitoxin must be given early, since the antitoxin neutralizes
Administered antitoxin
After 20 minutes, you must meter papule too, and
Administered antitoxin
After 20 minutes, you must meter papule too, and
The dose of the antitoxin
ranging from 20,000 to 100,000 U, is
The dose of the antitoxin
ranging from 20,000 to 100,000 U, is
Antimicrobial treatment
is required to eradicate the organism and prevent spread;
Antimicrobial treatment
is required to eradicate the organism and prevent spread;
Prophylaxis
Active immunization with diphtheria-tetanus-pertussis (DTP) vaccine should be routinely given
Prophylaxis
Active immunization with diphtheria-tetanus-pertussis (DTP) vaccine should be routinely given
Management of an Outbreak
All symptomatic patients should be isolated
Contact precautions
Management of an Outbreak
All symptomatic patients should be isolated
Contact precautions
INFECTIOUS MONONUCLEOSIS
is an acute disease which, characterized by fever, pharyngitis,
INFECTIOUS MONONUCLEOSIS
is an acute disease which, characterized by fever, pharyngitis,
Etiology and Pathophysiology
Epstein-Barr virus (EBV) is a herpesvirus with a
Etiology and Pathophysiology
Epstein-Barr virus (EBV) is a herpesvirus with a
Epidemiology
EBV is relatively labile and is not very contagious
In most
Epidemiology
EBV is relatively labile and is not very contagious
In most
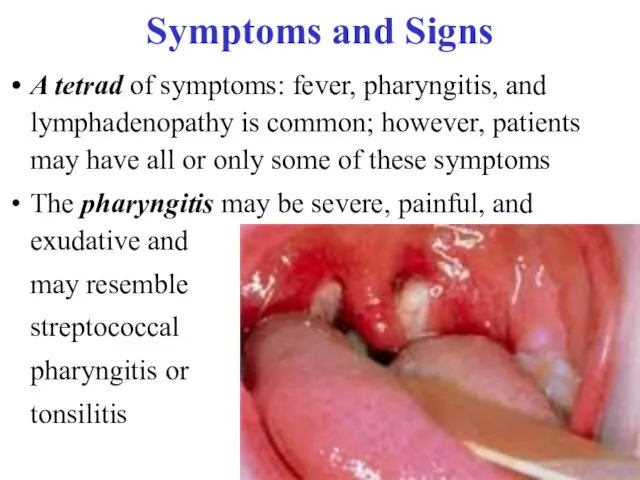
Symptoms and Signs
A tetrad of symptoms: fever, pharyngitis, and lymphadenopathy
Symptoms and Signs
A tetrad of symptoms: fever, pharyngitis, and lymphadenopathy
Lymphadenopathy may involve any group of nodes but is usually symmetric;
Lymphadenopathy may involve any group of nodes but is usually symmetric;
Complications
Neurosis complications include encephalitis, Guieain-Barre syndrome, peripheral neuropathy, aseptic meningitis,
Complications
Neurosis complications include encephalitis, Guieain-Barre syndrome, peripheral neuropathy, aseptic meningitis,
Complications
Pulmonary complications - obstruction due to pharyngeal or paratracheal lymphadenopathy,
Complications
Pulmonary complications - obstruction due to pharyngeal or paratracheal lymphadenopathy,
Laboratory Findings and Diagnosis
the clinical syndrome of infectious mononucleosis and
Laboratory Findings and Diagnosis
the clinical syndrome of infectious mononucleosis and
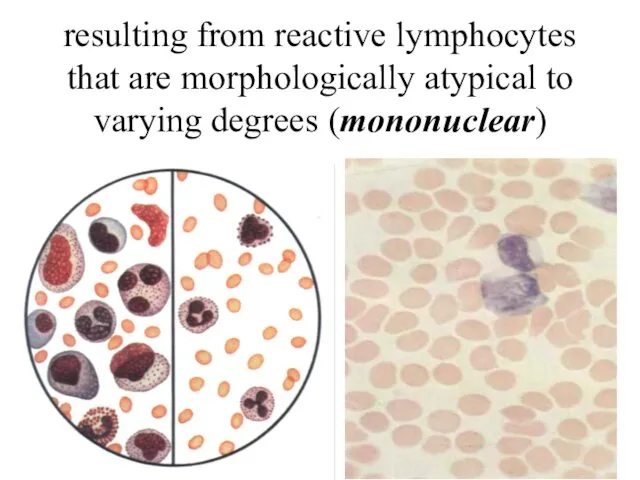
resulting from reactive lymphocytes that are morphologically atypical to varying degrees
resulting from reactive lymphocytes that are morphologically atypical to varying degrees
Differential Diagnosis
The pharyngitis, lymphadenopathy, and fever may be clinically indistinguishable
Differential Diagnosis
The pharyngitis, lymphadenopathy, and fever may be clinically indistinguishable
Prognosis
Infectious mononucleosis is usually self-limited
The duration of the illness varies;
Prognosis
Infectious mononucleosis is usually self-limited
The duration of the illness varies;
Treatment
Patients should be encouraged to rest during the acute phase
Treatment
Patients should be encouraged to rest during the acute phase
Varicella
is an acute infectious disease, characterized by vesicular eruption with transparent
Varicella
is an acute infectious disease, characterized by vesicular eruption with transparent
Etiology and Epidemiology
The Varicella virus contains DNA. Varicella and herpes zoster
Etiology and Epidemiology
The Varicella virus contains DNA. Varicella and herpes zoster
Pathogenesis and pathology
The portal of entry is the mucous membrane of
Pathogenesis and pathology
The portal of entry is the mucous membrane of
In very rare cases the lungs, liver, spleen, kidneys, pancreas, and
In very rare cases the lungs, liver, spleen, kidneys, pancreas, and
Clinical manifestations
The incubation period averages 11-21 days
The outbreak of rash coincides
Clinical manifestations
The incubation period averages 11-21 days
The outbreak of rash coincides
Vesicles are round or oval, differ in size, and are seated
Vesicles are round or oval, differ in size, and are seated
Atypical forms
In the bullous form of varicella large flabby bullae develop
Atypical forms
In the bullous form of varicella large flabby bullae develop
Complications
Complications are rare in Varicella: keratitis, laryngitis, abscesses, phlegmons, stomatitis, otitis,
Complications
Complications are rare in Varicella: keratitis, laryngitis, abscesses, phlegmons, stomatitis, otitis,
 Микотоксины. Действие микотоксинов в истории
Микотоксины. Действие микотоксинов в истории Общие принципы лечения абсцессов и флегмон лица и шеи. Физиотерапия и реабилитация больных
Общие принципы лечения абсцессов и флегмон лица и шеи. Физиотерапия и реабилитация больных Диспансерное наблюдение за детьми с хроническими заболеваниями
Диспансерное наблюдение за детьми с хроническими заболеваниями Хронические расстройства питания у детей
Хронические расстройства питания у детей Наследственные заболевания человека
Наследственные заболевания человека Геморрагический шок
Геморрагический шок Гипогликемическая и гипергликемическая комы
Гипогликемическая и гипергликемическая комы Пути введения лекарственных средств
Пути введения лекарственных средств Обзор и принципы реанимации новорожденных
Обзор и принципы реанимации новорожденных Современные алгоритмы лечения сахарного диабета 2 типа
Современные алгоритмы лечения сахарного диабета 2 типа Нейропсихологическая диагностика
Нейропсихологическая диагностика Общая характеристика группы инфекционных болезней с воздушнокапельным механизмом передачи. Грипп
Общая характеристика группы инфекционных болезней с воздушнокапельным механизмом передачи. Грипп Вагинальные инфекции при беременности
Вагинальные инфекции при беременности Federal State Educational Institution of Higher Education
Federal State Educational Institution of Higher Education Синдром наличия жидкости и газа в плевральной полости. Плевриты
Синдром наличия жидкости и газа в плевральной полости. Плевриты Холера. Эпидемиология
Холера. Эпидемиология Хронический пылевой бронхит
Хронический пылевой бронхит Легочное сердце
Легочное сердце Инфекционный мононуклеоз у детей
Инфекционный мононуклеоз у детей Понятие гиподинамии, гипердинамии
Понятие гиподинамии, гипердинамии Действия ассистента, осуществляемые до прихода врача-стоматолога, после прихода врача-стоматолога и после окончания лечения
Действия ассистента, осуществляемые до прихода врача-стоматолога, после прихода врача-стоматолога и после окончания лечения Митральные пороки сердца
Митральные пороки сердца Критерии и качества стоматологических материалов. Система международных и национальных стандартов
Критерии и качества стоматологических материалов. Система международных и национальных стандартов Введение в венерологию. История развития венерологии. Инфекции, передающиеся половым путем
Введение в венерологию. История развития венерологии. Инфекции, передающиеся половым путем Доказательная профилактика. Скрининговые программы
Доказательная профилактика. Скрининговые программы Endocrine system
Endocrine system Современные подходы к лечению эндометриоидных кист яичников
Современные подходы к лечению эндометриоидных кист яичников Дисфункционалдық жатырдан қан кету
Дисфункционалдық жатырдан қан кету