- Valvular heart disease. Mitral valve

Содержание
- 37. Natural History of Mitral Regurgitation With acute mitral regurgitation, left atrial compliance is predominantly fixed; therefore
- 38. Chronic Mitral Regurgitation Patients with chronic mitral regurgitation will have a long latent period before becoming
- 39. Mitral Regurgitation hemodynamics In patients with significant mitral regurgitation, prominent v-waves are seen on the left
- 40. Symptoms Fatigue & weakness – due to ? CO – predominant complaint Exertional dyspnea & cough
- 41. Sings Atrial fibrillation Cardiomegally Apical pansystolic murmur +/- thrill Soft S1, apical S3 Signs of pulmonary
- 42. escardio.org 2017
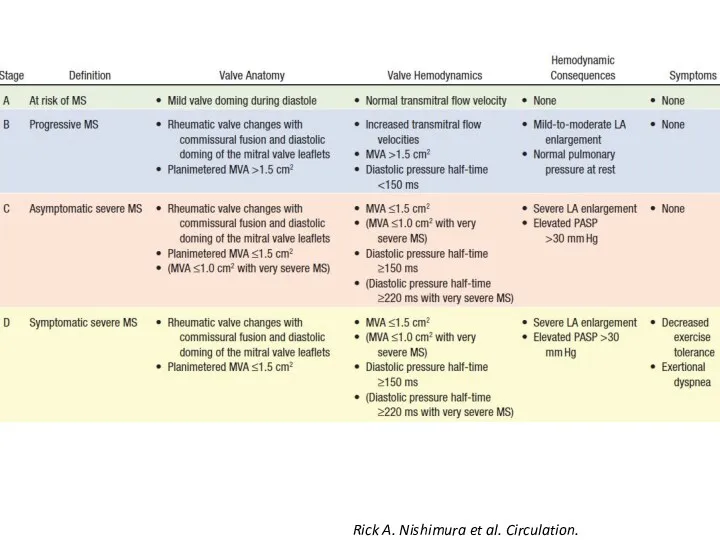
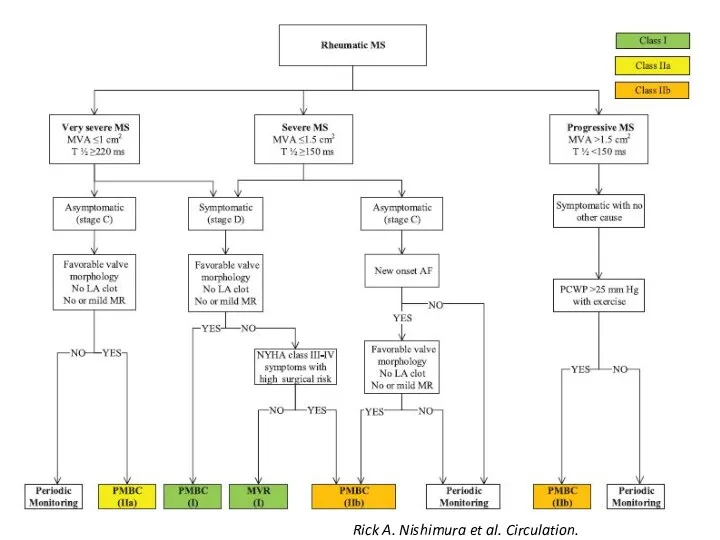
- 43. Rick A. Nishimura et al. Circulation. 2014;129:2440-2492
- 45. Type IIIb (restricted leaflet closing) ▪ Regional/global LV dysfunction ▪ LV & Papillary muscles geometry changes
- 46. MitraClip device
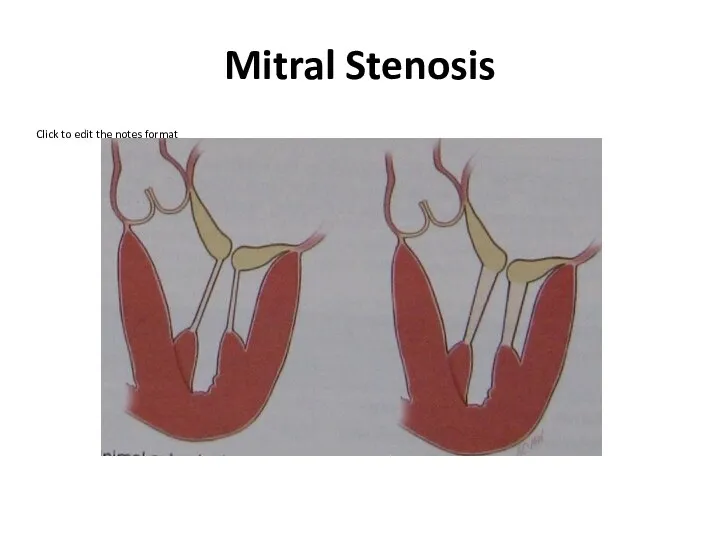
- 49. Mitral Stenosis
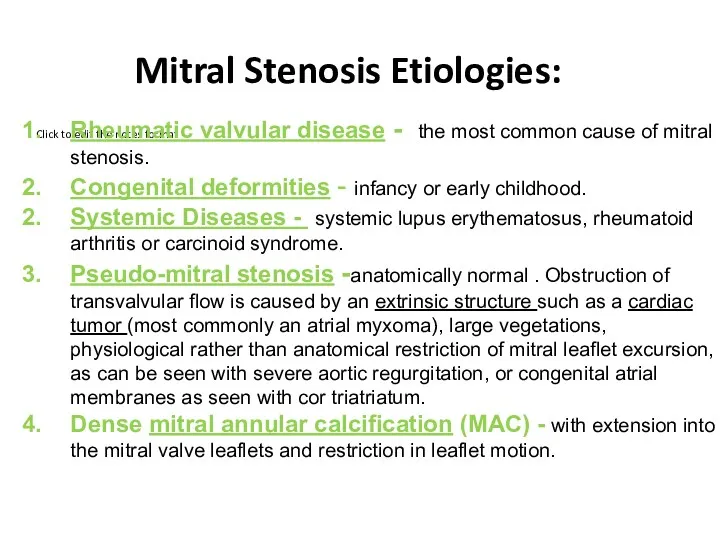
- 50. Mitral Stenosis Etiologies: Rheumatic valvular disease - the most common cause of mitral stenosis. Congenital deformities
- 51. Rheumatic Valvular Disease Rheumatic fever is a collagen vascular disorder which occurs following group A beta-hemolytic
- 52. Rheumatic Mitral Stenosis
- 53. Acute Rheumatic Fever: Modified Jones’ criteria Major Carditis (Myocarditis, pericarditis, valvulitis) Polyarthritis Sydenham’s chorea Subcutaneous nodules
- 54. Acute Rheumatic Fever: Presentation
- 55. Acute Rheumatic Fever: Some clinical signs Erythema marginatum
- 56. Acute Phase Chronic Phase valve leaflet inflammation can result in transient regurgitant murmurs and mid diastolic
- 57. Mitral Valve Stenosis: Sings Palpation: Small volume pulse Tapping apex-palpable S1 Palpable S2 Atrial fibrillation Signs
- 58. Hemodynamics of MS Left ventricular pressure rises above left atrial pressure in early systole causing the
- 59. Mitral Valve Stenosis HEMODYNAMICS
- 60. What is the impact of chronic elevation in left atrial pressures on the remainder of the
- 61. With mitral stenosis, there is impedance to left atrial emptying. Left atrial pressure rises to maintain
- 62. With ongoing passive congestion, reactive vasoconstriction occurs in the pre-capillary beds (“pre-capillary block") causing additional increases
- 63. Precapillary Block Fatigue Exhaustion Weakness Tiredness Right-sided failure Edema, hepatomegaly Tricuspid insufficiency Cyanosis(peripheral) Large heart Mild
- 64. With ongoing passive congestion, reactive vasoconstriction occurs in the pre-capillary beds (“pre-capillary block") causing additional increases
- 65. Mitral Valve Stenosis: Symptoms Dyspnea and cough (pulmonary vascular congestion and pulmonary hypertension) Orthopnea (related to
- 66. Auscultatory findings With a structurally normal mitral valve, there is no significant LA to LV diastolic
- 67. With mild mitral stenosis, left atrial pressure is elevated creating a LA to LV pressure gradient
- 68. As mitral stenosis increases in severity, left atrial pressure continues to rise to a point where
- 69. S1 S2 OS S1 First heart sound (S1) is loud and snapping Opening snap (OS) Low
- 70. Mitral Valve Stenosis: Pathophysiology Normal valve area: 4-6 cm2 Mild mitral stenosis: MVA 1.5-2.5 cm2 Minimal
- 71. Chest XR
- 72. Type IIIa (restricted leaflet opening) Domelike anterior leaflet movement, restriction of posterior leaflet subvalvular fusions
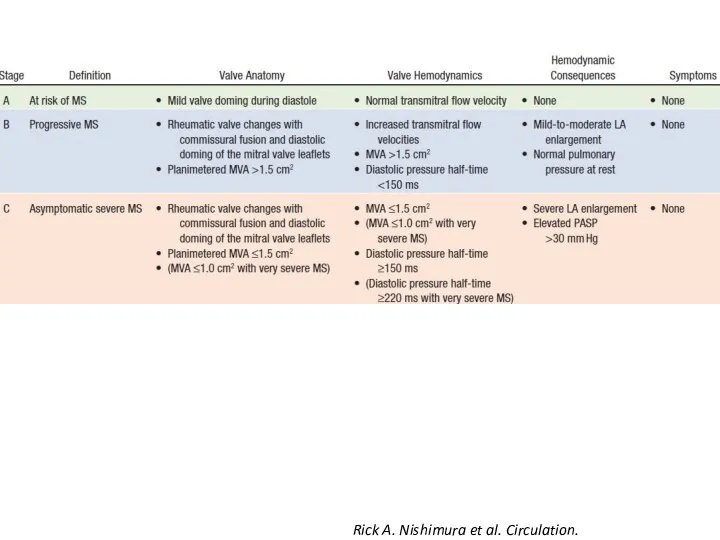
- 73. Rick A. Nishimura et al. Circulation. 2014;129:2440-2492
- 74. Rick A. Nishimura et al. Circulation. 2014;129:2440-2492
- 75. Rick A. Nishimura et al. Circulation. 2014;129:2440-2492
- 76. Rick A. Nishimura et al. Circulation. 2014;129:2440-2492
- 77. Percutaneous balloon valvuloplasty Carpentier A. “Reconstructive valve surgery” 2010
- 78. Percutaneous balloon valvuloplasty
- 79. Mitral Valve Repair Carpentier A. “Reconstructive valve surgery” 2010
- 81. Скачать презентацию

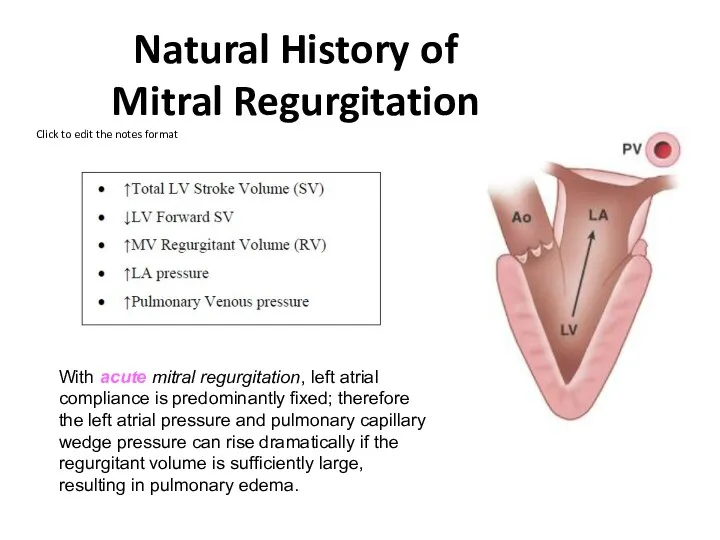
Natural History of
Mitral Regurgitation
With acute mitral regurgitation, left atrial compliance
Natural History of
Mitral Regurgitation
With acute mitral regurgitation, left atrial compliance
Chronic Mitral Regurgitation
Patients with chronic mitral regurgitation will have a long
Chronic Mitral Regurgitation
Patients with chronic mitral regurgitation will have a long
Mitral Regurgitation hemodynamics
In patients with significant mitral regurgitation, prominent v-waves are
Mitral Regurgitation hemodynamics
In patients with significant mitral regurgitation, prominent v-waves are
Symptoms
Fatigue & weakness – due to ? CO – predominant
Symptoms
Fatigue & weakness – due to ? CO – predominant
Sings
Atrial fibrillation
Cardiomegally
Apical pansystolic murmur +/- thrill
Soft S1, apical S3
Signs
Sings
Atrial fibrillation
Cardiomegally
Apical pansystolic murmur +/- thrill
Soft S1, apical S3
Signs
escardio.org
2017
escardio.org
2017
Rick A. Nishimura et al. Circulation. 2014;129:2440-2492
Rick A. Nishimura et al. Circulation. 2014;129:2440-2492
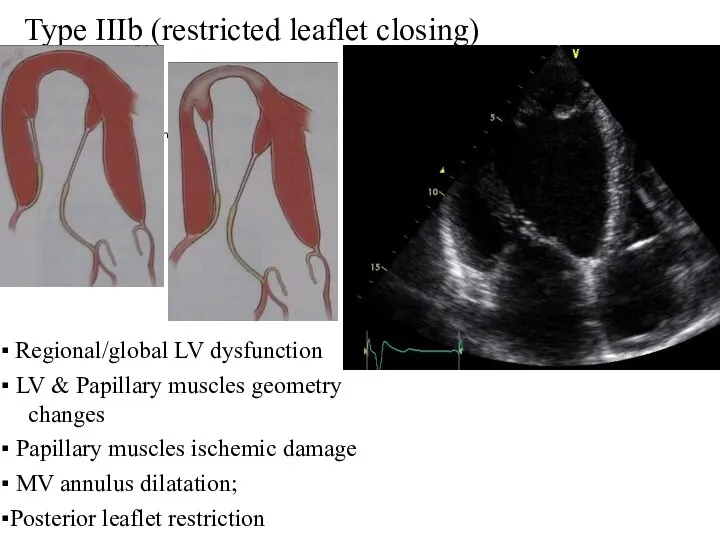
Type IIIb (restricted leaflet closing)
▪ Regional/global LV dysfunction
▪ LV & Papillary
Type IIIb (restricted leaflet closing)
▪ Regional/global LV dysfunction
▪ LV & Papillary
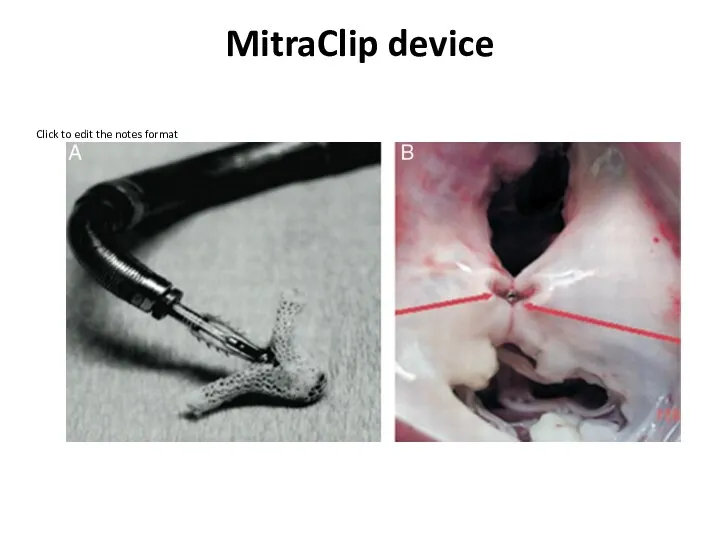
MitraClip device
MitraClip device
Mitral Stenosis
Mitral Stenosis
Mitral Stenosis Etiologies:
Rheumatic valvular disease - the most common cause of
Mitral Stenosis Etiologies:
Rheumatic valvular disease - the most common cause of
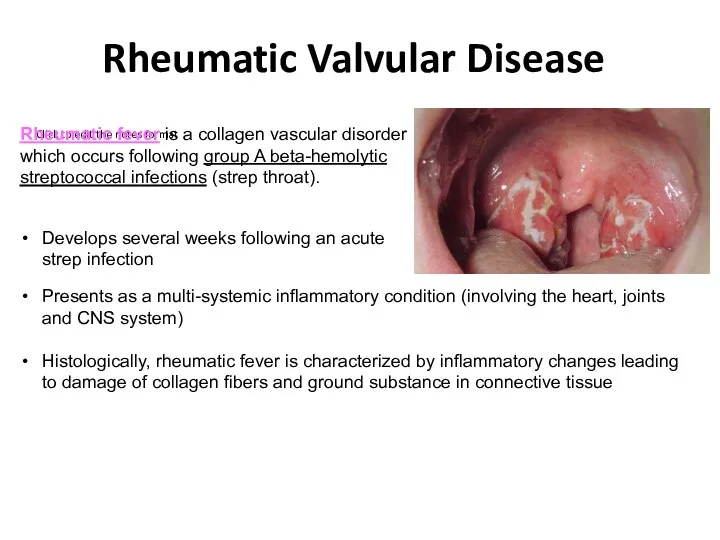
Rheumatic Valvular Disease
Rheumatic fever is a collagen vascular disorder which occurs
Rheumatic Valvular Disease
Rheumatic fever is a collagen vascular disorder which occurs
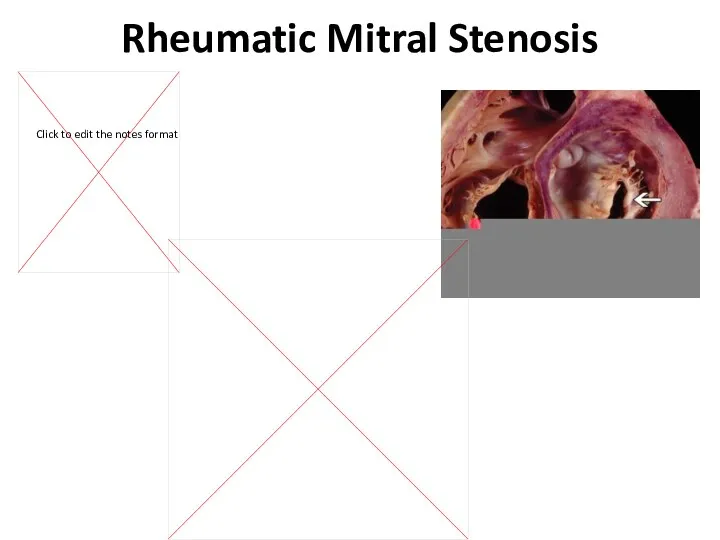
Rheumatic Mitral Stenosis
Rheumatic Mitral Stenosis
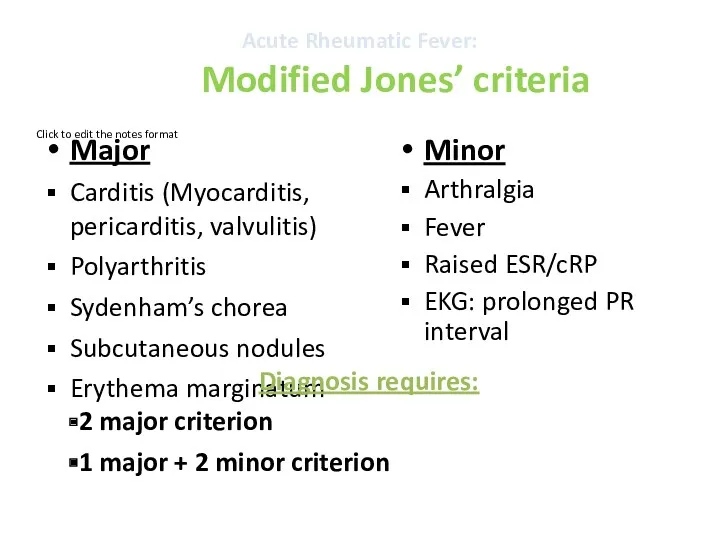
Acute Rheumatic Fever:
Modified Jones’ criteria
Major
Carditis (Myocarditis, pericarditis, valvulitis)
Polyarthritis
Sydenham’s chorea
Subcutaneous nodules
Erythema marginatum
Minor
Acute Rheumatic Fever:
Modified Jones’ criteria
Major
Carditis (Myocarditis, pericarditis, valvulitis)
Polyarthritis
Sydenham’s chorea
Subcutaneous nodules
Erythema marginatum
Minor
Acute Rheumatic Fever: Presentation
Acute Rheumatic Fever: Presentation
Acute Rheumatic Fever:
Some clinical signs
Erythema marginatum
Acute Rheumatic Fever:
Some clinical signs
Erythema marginatum
Acute
Phase
Chronic
Phase
valve leaflet inflammation can result in transient regurgitant murmurs and mid
Acute
Phase
Chronic
Phase
valve leaflet inflammation can result in transient regurgitant murmurs and mid
Mitral Valve Stenosis: Sings
Palpation:
Small volume pulse
Tapping apex-palpable S1
Palpable S2
Atrial fibrillation
Signs
Mitral Valve Stenosis: Sings
Palpation:
Small volume pulse
Tapping apex-palpable S1
Palpable S2
Atrial fibrillation
Signs
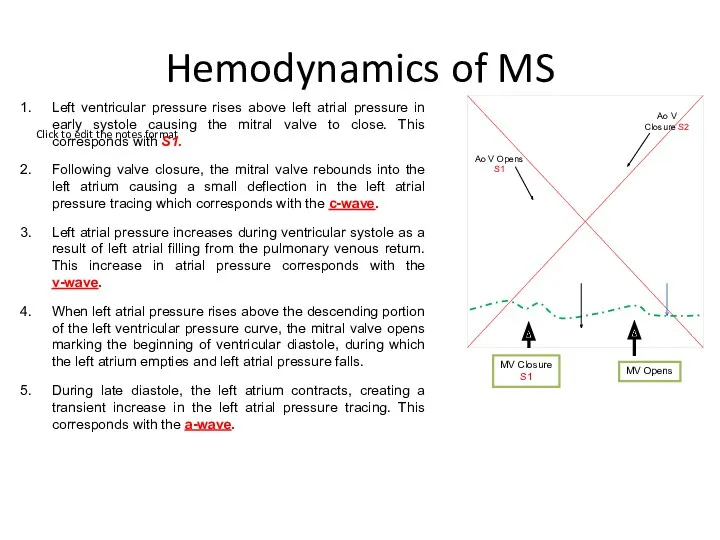
Hemodynamics of MS
Left ventricular pressure rises above left atrial pressure in
Hemodynamics of MS
Left ventricular pressure rises above left atrial pressure in
Mitral Valve Stenosis
HEMODYNAMICS
Mitral Valve Stenosis
HEMODYNAMICS
What is the impact of chronic elevation in left atrial pressures
What is the impact of chronic elevation in left atrial pressures
With mitral stenosis, there is impedance to left atrial emptying.
Left
With mitral stenosis, there is impedance to left atrial emptying.
Left
With ongoing passive congestion, reactive vasoconstriction occurs in the pre-capillary beds
With ongoing passive congestion, reactive vasoconstriction occurs in the pre-capillary beds
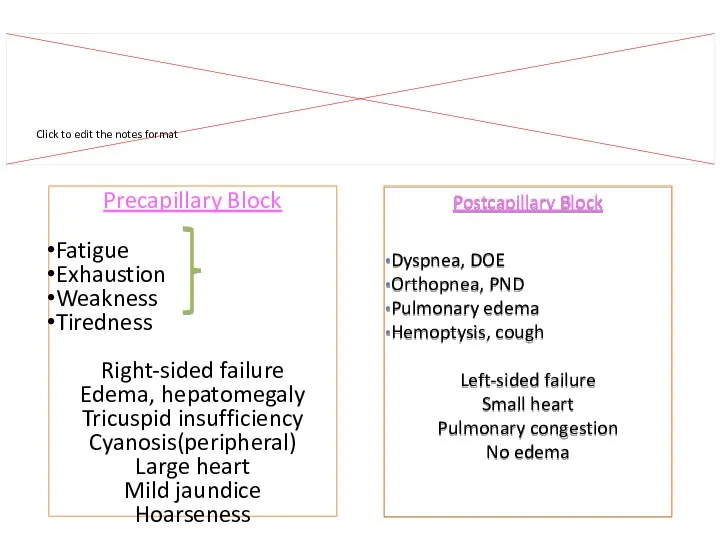
Precapillary Block
Fatigue
Exhaustion
Weakness
Tiredness
Right-sided failure
Edema, hepatomegaly
Tricuspid insufficiency
Cyanosis(peripheral)
Large heart
Mild jaundice
Hoarseness
Signs and symptoms of
Precapillary Block
Fatigue
Exhaustion
Weakness
Tiredness
Right-sided failure
Edema, hepatomegaly
Tricuspid insufficiency
Cyanosis(peripheral)
Large heart
Mild jaundice
Hoarseness
Signs and symptoms of
With ongoing passive congestion, reactive vasoconstriction occurs in the pre-capillary beds
With ongoing passive congestion, reactive vasoconstriction occurs in the pre-capillary beds
Mitral Valve Stenosis: Symptoms
Dyspnea and cough (pulmonary vascular congestion and pulmonary
Mitral Valve Stenosis: Symptoms
Dyspnea and cough (pulmonary vascular congestion and pulmonary
Auscultatory findings
With a structurally normal mitral valve, there is no
Auscultatory findings
With a structurally normal mitral valve, there is no
With mild mitral stenosis, left atrial pressure is elevated creating a
With mild mitral stenosis, left atrial pressure is elevated creating a
As mitral stenosis increases in severity, left atrial pressure continues to
As mitral stenosis increases in severity, left atrial pressure continues to
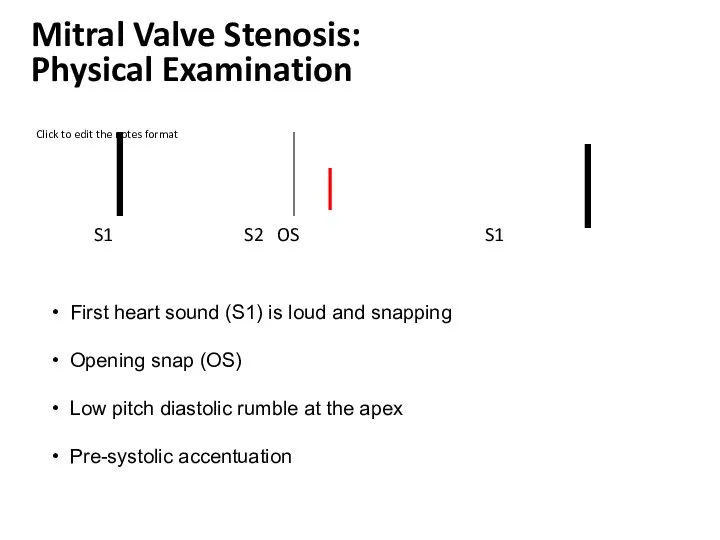
S1 S2 OS S1
First heart sound (S1) is loud and
S1 S2 OS S1
First heart sound (S1) is loud and
Mitral Valve Stenosis: Pathophysiology
Normal valve area: 4-6 cm2
Mild mitral stenosis:
MVA
Mitral Valve Stenosis: Pathophysiology
Normal valve area: 4-6 cm2
Mild mitral stenosis:
MVA
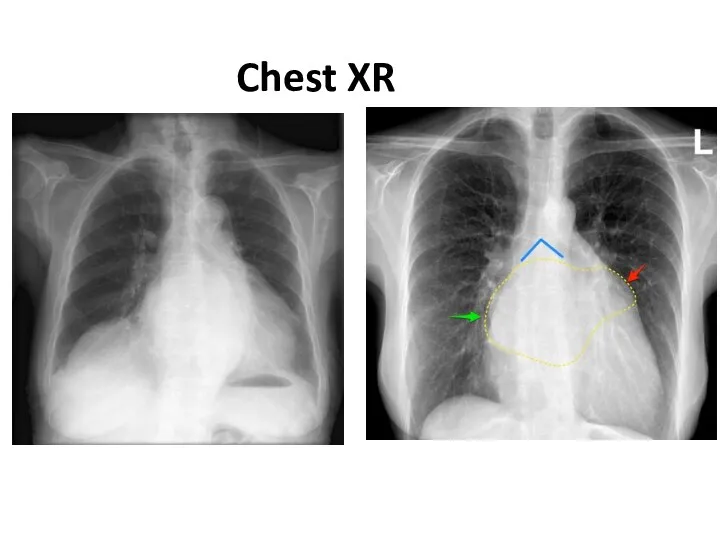
Chest XR
Chest XR
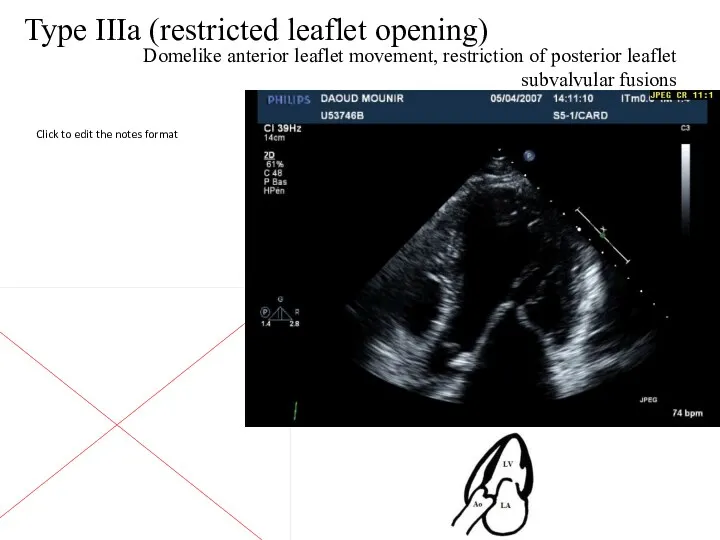
Type IIIa (restricted leaflet opening)
Domelike anterior leaflet movement, restriction of posterior
Type IIIa (restricted leaflet opening)
Domelike anterior leaflet movement, restriction of posterior
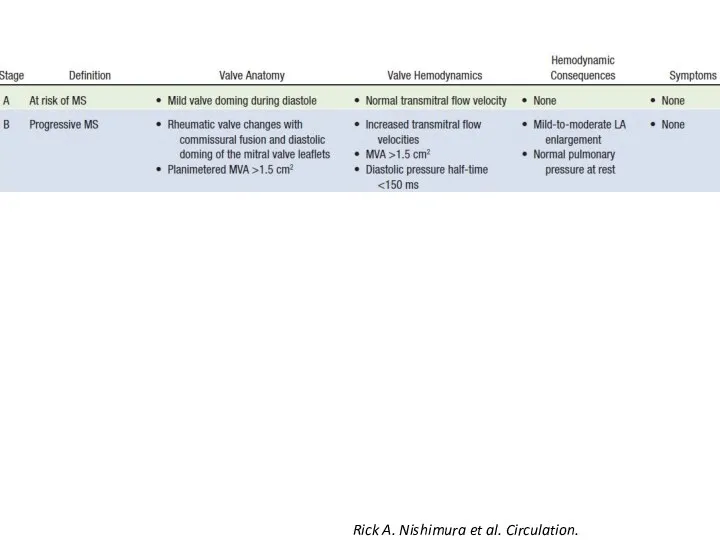
Rick A. Nishimura et al. Circulation. 2014;129:2440-2492
Rick A. Nishimura et al. Circulation. 2014;129:2440-2492
Rick A. Nishimura et al. Circulation. 2014;129:2440-2492
Rick A. Nishimura et al. Circulation. 2014;129:2440-2492
Rick A. Nishimura et al. Circulation. 2014;129:2440-2492
Rick A. Nishimura et al. Circulation. 2014;129:2440-2492
Rick A. Nishimura et al. Circulation. 2014;129:2440-2492
Rick A. Nishimura et al. Circulation. 2014;129:2440-2492
Percutaneous balloon valvuloplasty
Carpentier A. “Reconstructive valve surgery” 2010
Percutaneous balloon valvuloplasty
Carpentier A. “Reconstructive valve surgery” 2010
Percutaneous balloon valvuloplasty
Percutaneous balloon valvuloplasty
Mitral Valve Repair
Carpentier A. “Reconstructive valve surgery” 2010
Mitral Valve Repair
Carpentier A. “Reconstructive valve surgery” 2010
 Способы восстановления дефектов кожи
Способы восстановления дефектов кожи Ревматоидный артрит
Ревматоидный артрит Причины, клинические проявления проблем пациентов детского возраста при наследственных и врожденных заболеваниях
Причины, клинические проявления проблем пациентов детского возраста при наследственных и врожденных заболеваниях Апаттар медицинасын ұйымдастыру принциптері
Апаттар медицинасын ұйымдастыру принциптері Особенности ЭКГ у детей
Особенности ЭКГ у детей Анатомо-физиологические механизмы речи
Анатомо-физиологические механизмы речи Лучевые поражения в результате общего облучения
Лучевые поражения в результате общего облучения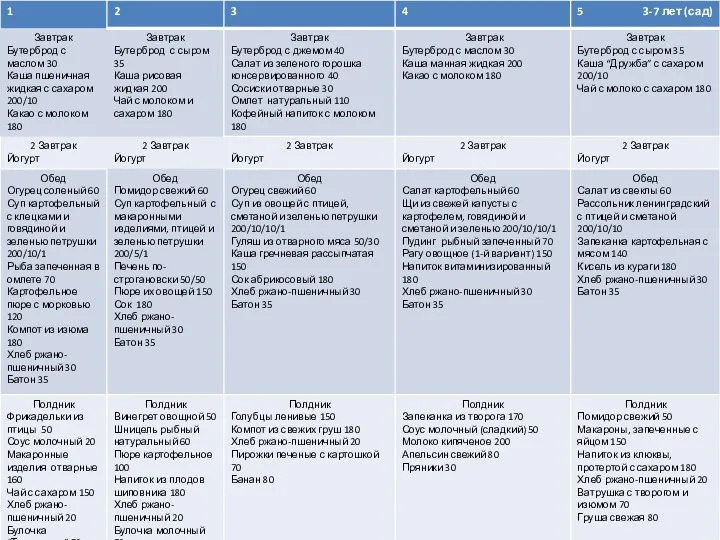 Меню 3-7 лет(сад)
Меню 3-7 лет(сад) Esophagus stomach
Esophagus stomach Клинико-фармакологические подходы к выбору лекарственных средств, применяемых для лечения сердечной недостаточности
Клинико-фармакологические подходы к выбору лекарственных средств, применяемых для лечения сердечной недостаточности Патология последа. Часть I
Патология последа. Часть I Микропрепараты. Патологическая анатомия
Микропрепараты. Патологическая анатомия Неходжкинские лимфомы у ВИЧ-инфицированных больных
Неходжкинские лимфомы у ВИЧ-инфицированных больных Этиология и патогенез туберкулеза
Этиология и патогенез туберкулеза Дифференциальная диагностика при гепато-лиенальном синдроме
Дифференциальная диагностика при гепато-лиенальном синдроме Роль общей лечебной сети в выявлении и профилактике туберкулеза
Роль общей лечебной сети в выявлении и профилактике туберкулеза Анемия и беременность
Анемия и беременность Ханс Бийлсма. Актуальные вопросы ревматологии
Ханс Бийлсма. Актуальные вопросы ревматологии Диагностика и лечение болезни Гиршпрунга у новорожденных
Диагностика и лечение болезни Гиршпрунга у новорожденных Врожденные аномалии
Врожденные аномалии Электроэнцефалография (қысқаша ЭЭГ)
Электроэнцефалография (қысқаша ЭЭГ) Сестринский процесс. Документация к сестринскому процессу. 2018 г
Сестринский процесс. Документация к сестринскому процессу. 2018 г Острые экзогенные интоксикации
Острые экзогенные интоксикации Хронические гепатиты у детей
Хронические гепатиты у детей Ісікке қарсы иммунитет. Вакцинды профилактика негіздері
Ісікке қарсы иммунитет. Вакцинды профилактика негіздері Рак шейки матки у беременных женщин
Рак шейки матки у беременных женщин Heart disease
Heart disease Аборт – экстренная контрацепция или убийство?
Аборт – экстренная контрацепция или убийство?