- What is acute coronary syndrome?

Содержание
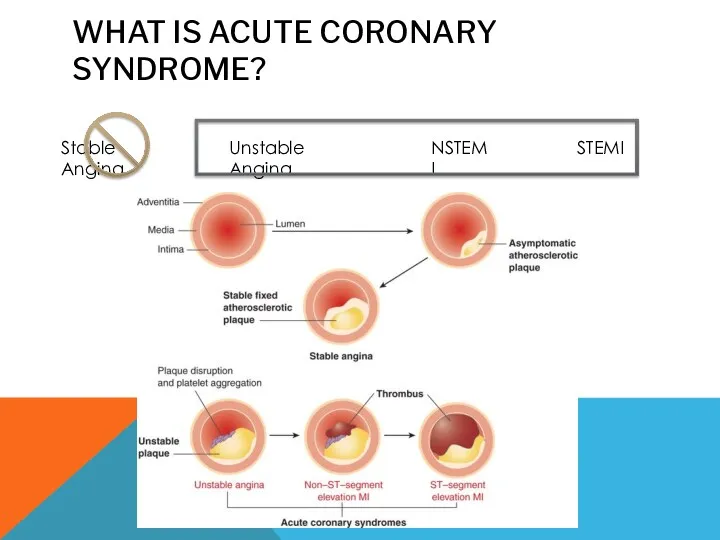
- 2. WHAT IS ACUTE CORONARY SYNDROME? Stable Angina Unstable Angina NSTEMI STEMI
- 3. DEFINITIONS Unstable angina: An unprovoked or prolonged episode of chest pain raising suspicion of acute myocardial
- 4. Atherosclerosis Epithelial injury Migration of monocytes/macrophages LDL lipids consumed ? foam cells Growth factors ? smooth
- 5. RISK FACTORS Increasing age Gender (male) Family History Hypertension Diabetes Smoking Obesity Diet Lack of exercise
- 6. CLINICAL FEATURES Dyspnoea Heart murmurs Palpitations Chest pain Nausea Acute confusion Pallor Hypotension or hypertension Sweaty
- 7. UA: platelet adhesion NSTEMI: platelet aggregation DISTINGUISHING FEATURES STEMI: complete occlusion SA: plaque formation At rest
- 8. RISK FACTORS MODIFIABLE Smoking Obesity Diet Lack of exercise High serum cholesterol Hypertension Diabetes NON-MODIFIABLE Increasing
- 9. DIFFERENTIAL DIAGNOSIS
- 10. WHAT DO YOU WANT TO ASK HIM/HER? 30minute history of central ‘crushing’ chest pain radiating to
- 11. INVESTIGATIONS * ST elevation is >1mm in limb leads and >2mm in chest leads
- 12. IMPORTANT ECG FINDINGS
- 13. WHERE IS THE PROBLEM?
- 14. COMMON ACS MANAGEMENT Morphine (5-10mg slow IV injection) Oxygen (titrate sats to need) Nitrates - GTN
- 15. LMWH i.e. Enoxaparin 1mg/kg BD or Fondaparinux 2.5mg OD Clopidogrel 300mg loading dose Beta blocker -
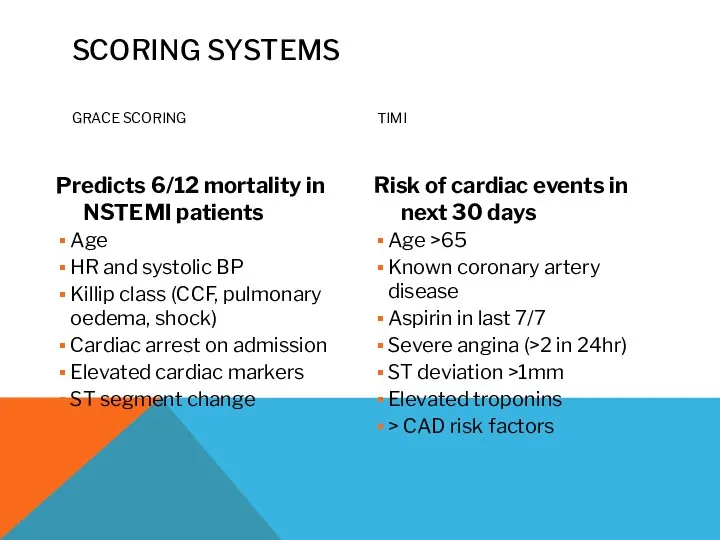
- 16. SCORING SYSTEMS GRACE SCORING Predicts 6/12 mortality in NSTEMI patients Age HR and systolic BP Killip
- 17. TIME IS MUSCLE Percutaneous coronary intervention (Primary PCI) ‘Call to balloon time’ of 120 minutes Requires
- 18. LONGER-TERM MANAGEMENT Continuous ECG monitoring as inpatient/ CCU Aspirin 75mg OD (lifelong) Clopidogrel 75mg (1 year)
- 20. Скачать презентацию
WHAT IS ACUTE CORONARY SYNDROME?
Stable Angina
Unstable Angina
NSTEMI
STEMI
WHAT IS ACUTE CORONARY SYNDROME?
Stable Angina
Unstable Angina
NSTEMI
STEMI
DEFINITIONS
Unstable angina:
An unprovoked or prolonged episode of chest pain raising suspicion
DEFINITIONS
Unstable angina:
An unprovoked or prolonged episode of chest pain raising suspicion
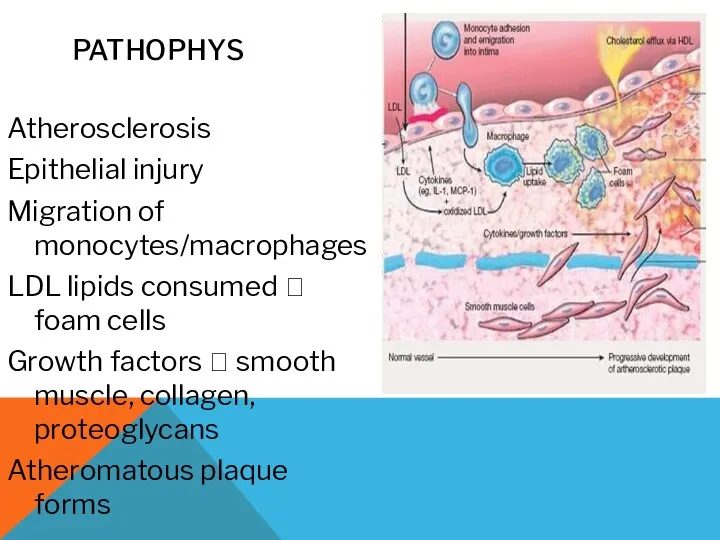
Atherosclerosis
Epithelial injury
Migration of monocytes/macrophages
LDL lipids consumed ? foam cells
Growth factors ?
Atherosclerosis
Epithelial injury
Migration of monocytes/macrophages
LDL lipids consumed ? foam cells
Growth factors ?
RISK FACTORS
Increasing age
Gender (male)
Family History
Hypertension
Diabetes
Smoking
Obesity
Diet
Lack of exercise
High serum cholesterol
RISK FACTORS
Increasing age
Gender (male)
Family History
Hypertension
Diabetes
Smoking
Obesity
Diet
Lack of exercise
High serum cholesterol
CLINICAL FEATURES
Dyspnoea
Heart murmurs
Palpitations
Chest pain
Nausea
Acute confusion
Pallor
Hypotension or hypertension
Sweaty
Vomiting
Syncope
Indigestion
Tachycardia or bradycardia
Fever
Asymptomatic/silent
CLINICAL FEATURES
Dyspnoea
Heart murmurs
Palpitations
Chest pain
Nausea
Acute confusion
Pallor
Hypotension or hypertension
Sweaty
Vomiting
Syncope
Indigestion
Tachycardia or bradycardia
Fever
Asymptomatic/silent
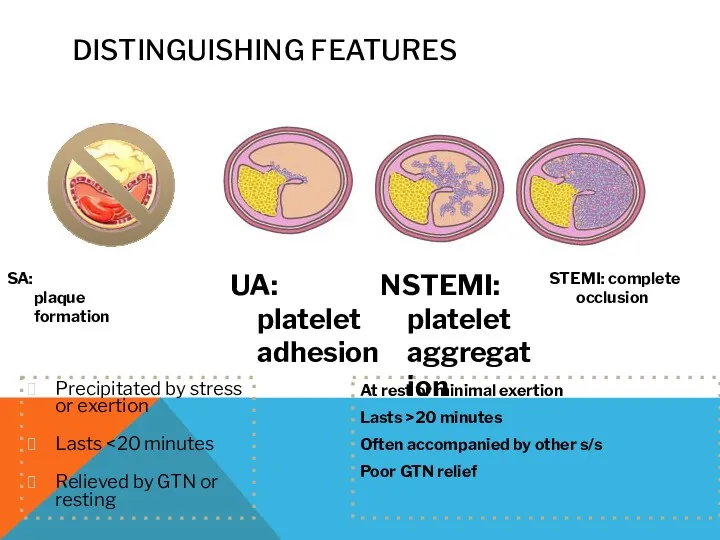
UA:
platelet
adhesion
NSTEMI: platelet aggregation
DISTINGUISHING FEATURES
STEMI: complete occlusion
SA:
plaque
formation
At rest
UA:
platelet
adhesion
NSTEMI: platelet aggregation
DISTINGUISHING FEATURES
STEMI: complete occlusion
SA:
plaque
formation
At rest
RISK FACTORS
MODIFIABLE
Smoking
Obesity
Diet
Lack of exercise
High serum cholesterol
Hypertension
Diabetes
NON-MODIFIABLE
Increasing age
Gender (male)
Ethnicity
Family History
?Diabetes
RISK FACTORS
MODIFIABLE
Smoking
Obesity
Diet
Lack of exercise
High serum cholesterol
Hypertension
Diabetes
NON-MODIFIABLE
Increasing age
Gender (male)
Ethnicity
Family History
?Diabetes
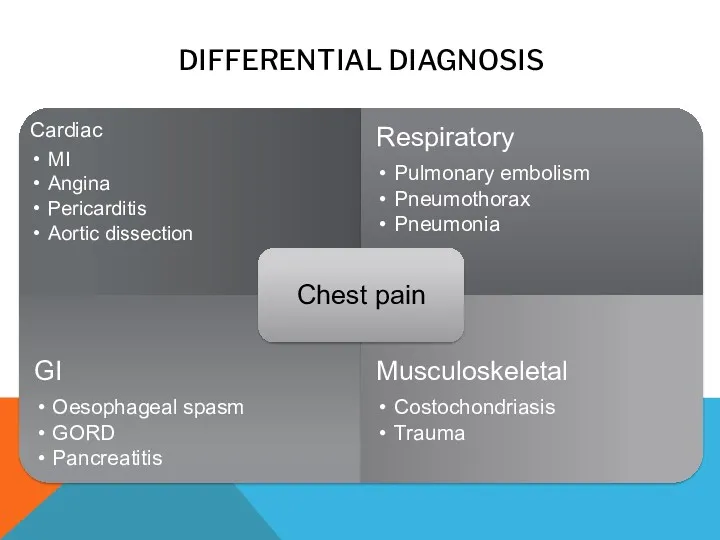
DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS
WHAT DO YOU WANT TO ASK HIM/HER?
30minute history of central ‘crushing’
WHAT DO YOU WANT TO ASK HIM/HER?
30minute history of central ‘crushing’

INVESTIGATIONS
* ST elevation is >1mm in limb leads and >2mm
INVESTIGATIONS
* ST elevation is >1mm in limb leads and >2mm
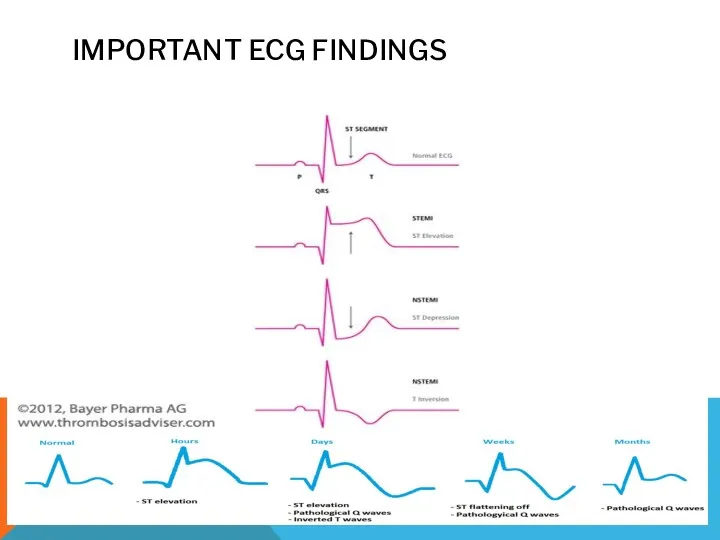
IMPORTANT ECG FINDINGS
IMPORTANT ECG FINDINGS
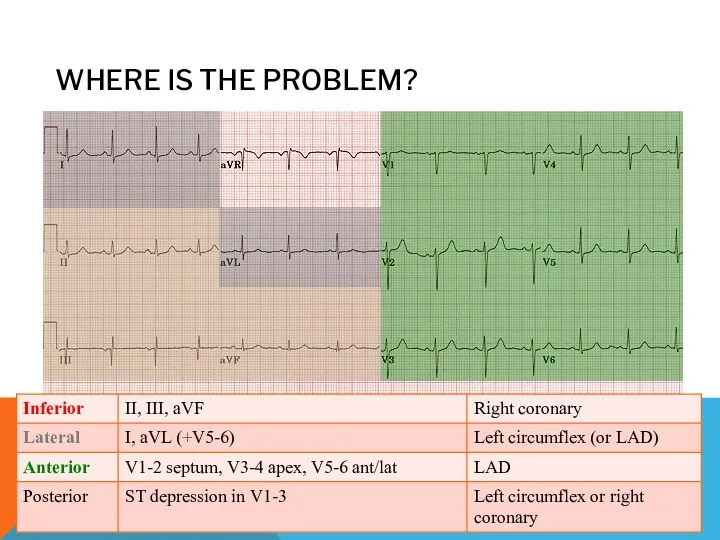
WHERE IS THE PROBLEM?
WHERE IS THE PROBLEM?
COMMON ACS MANAGEMENT
Morphine (5-10mg slow IV injection)
Oxygen (titrate sats to need)
Nitrates
COMMON ACS MANAGEMENT
Morphine (5-10mg slow IV injection)
Oxygen (titrate sats to need)
Nitrates
LMWH i.e. Enoxaparin 1mg/kg BD or Fondaparinux 2.5mg OD
Clopidogrel 300mg loading
LMWH i.e. Enoxaparin 1mg/kg BD or Fondaparinux 2.5mg OD
Clopidogrel 300mg loading
SCORING SYSTEMS
GRACE SCORING
Predicts 6/12 mortality in NSTEMI patients
Age
HR and systolic BP
Killip
SCORING SYSTEMS
GRACE SCORING
Predicts 6/12 mortality in NSTEMI patients
Age
HR and systolic BP
Killip
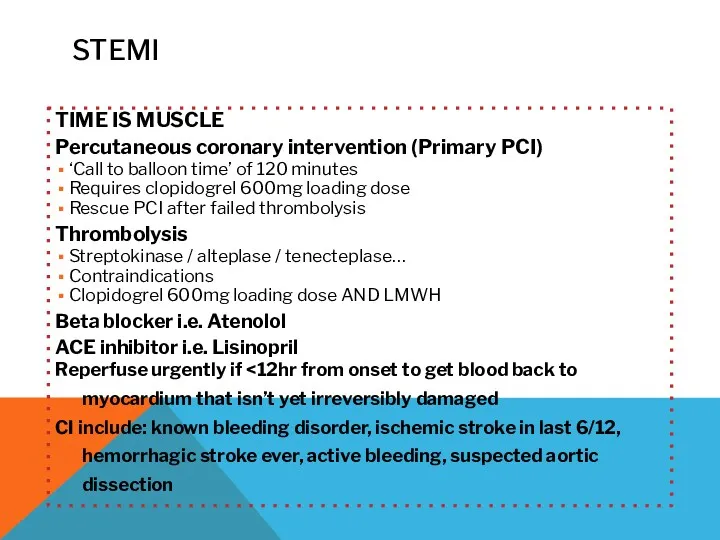
TIME IS MUSCLE
Percutaneous coronary intervention (Primary PCI)
‘Call to balloon time’ of
TIME IS MUSCLE
Percutaneous coronary intervention (Primary PCI)
‘Call to balloon time’ of

LONGER-TERM MANAGEMENT
Continuous ECG monitoring as inpatient/ CCU
Aspirin 75mg OD (lifelong)
Clopidogrel 75mg
LONGER-TERM MANAGEMENT
Continuous ECG monitoring as inpatient/ CCU
Aspirin 75mg OD (lifelong)
Clopidogrel 75mg
 Костная система. Кость, как орган. Классификация костей. Классификация суставов и их общая характеристика
Костная система. Кость, как орган. Классификация костей. Классификация суставов и их общая характеристика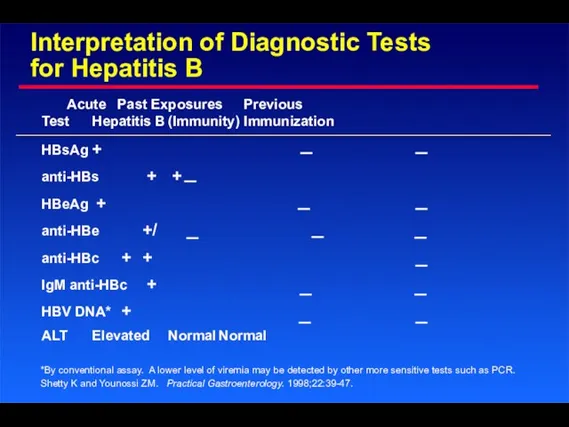 Interpretation of Diagnostic Tests for Hepatitis B. Test HBsAg Acute Hepatitis B
Interpretation of Diagnostic Tests for Hepatitis B. Test HBsAg Acute Hepatitis B Остеоартрит. Клинические рекомендации
Остеоартрит. Клинические рекомендации Инфекция или инфекционный процесс
Инфекция или инфекционный процесс Изготовление разборных моделей по технологии фирмы Renfert
Изготовление разборных моделей по технологии фирмы Renfert Psychopharmacologie: troubles anxieux
Psychopharmacologie: troubles anxieux Брэнды и Дженерики, вопросы взаимозаменяемости лекарственных препаратов
Брэнды и Дженерики, вопросы взаимозаменяемости лекарственных препаратов Рост и развитие зубочелюстно-лицевой области в пренатальный и постнатальный периоды
Рост и развитие зубочелюстно-лицевой области в пренатальный и постнатальный периоды Ауески ауруы
Ауески ауруы Суточное мониторирование АД
Суточное мониторирование АД Хронический бронхит
Хронический бронхит Основные инфекционные болезни
Основные инфекционные болезни Производство таблеток фурацилина
Производство таблеток фурацилина Нейропсихологические основы коррекционной педагогики. Лекция 1
Нейропсихологические основы коррекционной педагогики. Лекция 1 Tuberculosis. Mycobacterium tuberculosis
Tuberculosis. Mycobacterium tuberculosis Возрастные особенности кровеносных сосудов
Возрастные особенности кровеносных сосудов Учение о диагнозе
Учение о диагнозе Эпидемиологические характеристики инфекций, переносимых воздушно-капельным путем, профилактические меры в их распространении
Эпидемиологические характеристики инфекций, переносимых воздушно-капельным путем, профилактические меры в их распространении District sales manager, Novo Nordisk
District sales manager, Novo Nordisk Физиология детей и подростков (лекция 1)
Физиология детей и подростков (лекция 1) Кровотечение. Классификация. Временные и окончательные методы остановки кровотечения
Кровотечение. Классификация. Временные и окончательные методы остановки кровотечения Иммунотерапия в гастроэнтерологии
Иммунотерапия в гастроэнтерологии Расстройства внимания
Расстройства внимания Пред дошкольное медицинское обследование и оздоровление детей
Пред дошкольное медицинское обследование и оздоровление детей Здоровье родителей и здоровье будущего ребёнка
Здоровье родителей и здоровье будущего ребёнка Ревматоидный артрит
Ревматоидный артрит Мезенхимальные опухоли
Мезенхимальные опухоли Миома матки. Эндометриоз
Миома матки. Эндометриоз