- Risky business. Making decisions under uncertainty

Содержание
- 2. Overview Next unit up - Insurers Insurance theory & concepts Risk & uncertainty Insurance premiums Evolution
- 3. Risky Business: Making Decisions Under Uncertainty Uncertainty: A situation when more than one event may occur
- 4. Risk Defined Risk: The probability of incurring a loss (or some other misfortune). More precisely, risk
- 5. The Cost of Risk Some people are willing to bear more risk than others. In economics,
- 6. The Utility of Wealth
- 7. What can we observe from the Utility of Wealth Schedule? Utility increases as wealth increases. Change
- 8. Translate Utility of Wealth into Expected Utility Due to uncertainty, people do not know the actual
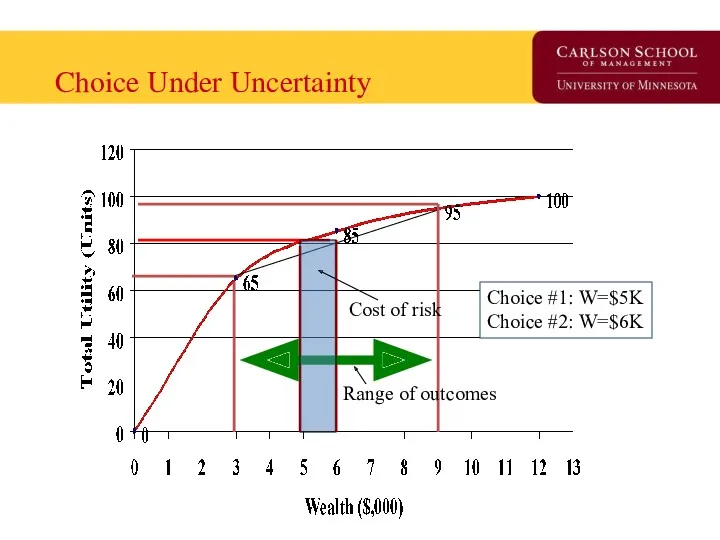
- 9. Choice Under Uncertainty Range of outcomes Cost of risk Choice #1: W=$5K Choice #2: W=$6K
- 10. Interpretation of Choice under Uncertainty At Choice #1, Tania’s wealth is $5K, U=80, no risk, At
- 11. Risk Aversion and Risk Neutrality Risk Averse: Someone who sees risk as not cost-less. The degree
- 12. Choice Under Uncertainty for Risk Neutral Person For Risk Neutral Person, Uncertainty is not an issue.
- 13. How do we reduce risk? Buy the ‘the cost of risk’ off. (similar to getting protection
- 14. How does Insurance work? Insurance works by ‘pooling’ risks. Insurance is possible and profitable because people
- 15. The Gains from Insurance Maximum value of Insurance Minimum cost of insurance Total Utility Wealth Range
- 16. Understanding the Graph At $10K, utility is 100. If one loses health (or a another valued
- 17. Understanding the Graph - 2 Up to what price will you buy insurance? What will insurance
- 18. Moral Hazard & Adverse Selection Private information is information that is available to one person but
- 19. Moral Hazard Defined: When one of two or more parities with an agreement has an incentive
- 20. Adverse Selection Defined: The tendency for people to enter into agreements in which they use private
- 21. Understanding the difference between the two People who face greater risks are more likely to purchase
- 22. How do insurance companies overcome these problems? Find a signal to convey information from outside the
- 23. Examine Evolution of a Market Using the “Time Machine” from Davey & Goliath
- 24. Slow Day? Starr got you down? Consider…. http://www.awn.com/heaven_and_hell/DG/DG4.htm
- 25. Early Public Health Insurance First instance of public insurance is Germany’s 1883 ‘compulsory sickness insurance’. Followed
- 26. U.S. Public Health Insurance Failed proposals made in Congress for National Health Insurance: 1918-19 1935-36 1948
- 27. Private Insurance – Two early models Fee-for-service insurance Epitomized by Blue Cross plan started for Baylor
- 28. Four characteristics of Blue Cross/Blue Shield fundamentally shaped American health care. Hospitals were reimbursed on a
- 29. Points of Inflection in Insurance Market -1 1930s – Great Depression reduces physician’s opposition to third
- 30. Points of Inflection in Insurance Market - 2 1983 – Medicare institutes prospective payment for hospital
- 31. State of Health Insurance Today Insurance models Demand side control programs Supply side control programs Market
- 32. Insurance Models in 2007 9% Conventional Fee for Service/Managed Indemnity Payment is based on a fee-schedule
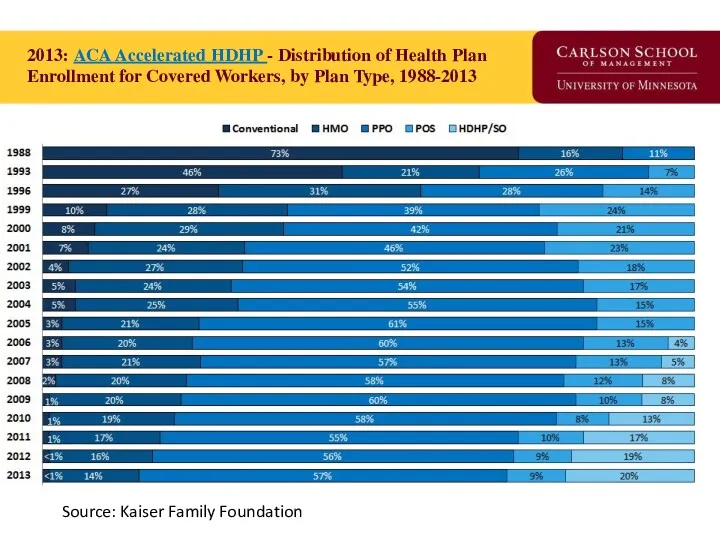
- 33. 2013: ACA Accelerated HDHP - Distribution of Health Plan Enrollment for Covered Workers, by Plan Type,
- 34. Insurance Tower of Babel PPO: Preferred Provider Organization (Medica) IDS: Integrated Delivery System (Fairview) HMO: Health
- 35. CDHP Business Enablers ‘Ready to Lease’ Components of Health Insurance: Electronic claims processing National panel of
- 36. CDHP Component Details Health Tools and Resources Care management program Extensive easy-to-use information and services Health
- 37. …The HSA Model Health Coverage Purchased by ‘Qualified’ Plans Annual deductible Expenses beyond the HSA No
- 38. Demand Side Controls ‘Affect the consumer to mitigate moral hazard’ Coinsurance, Copayments, Deductibles Specialist access through
- 39. Supply Side Controls ‘Reduce the probability of provider induced demand’ Fee schedules Diagnosis Related Groups RBRVS
- 40. Insurance ‘Market Success’ Primary funding source of medical innovation in the United States. Consumers have more
- 41. Insurance ‘Market Failures’ 50+ million uninsured (at any point in time) prior to ACA 120% health
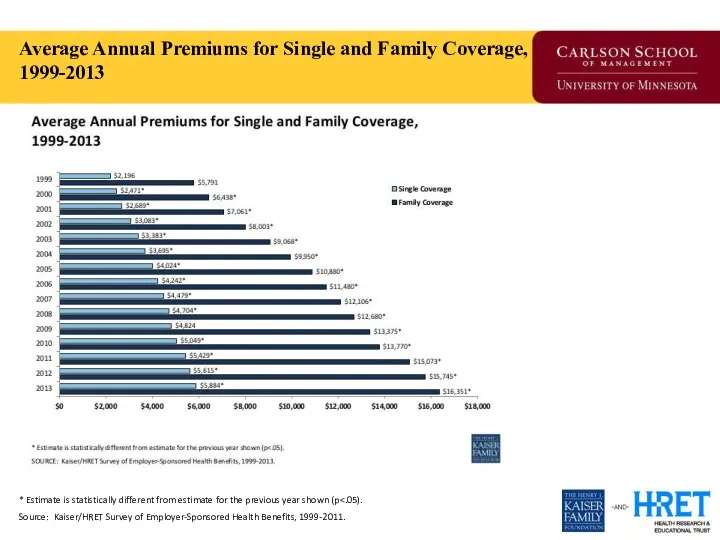
- 42. Average Annual Premiums for Single and Family Coverage, 1999-2013 * Estimate is statistically different from estimate
- 43. Question for Reflection How uniquely American is evolution of the insurance market in the 20th century?
- 44. The Uninsured Problem Who are the uninsured? Why is this a ‘market failure’? If government were
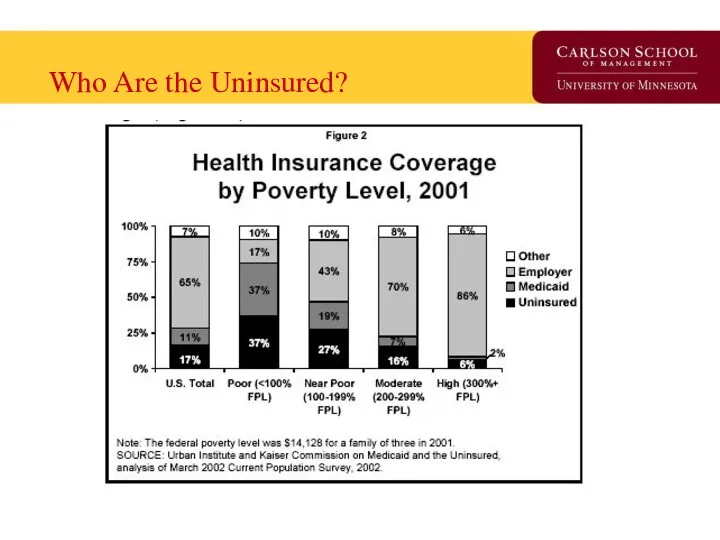
- 45. Who Are the Uninsured?
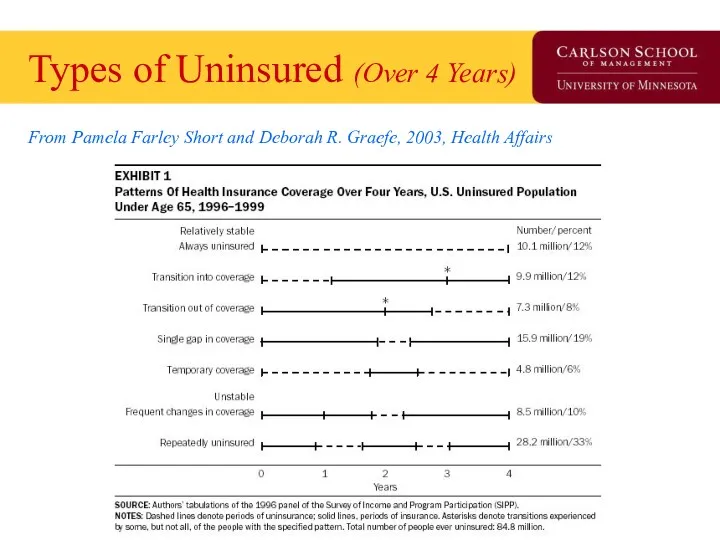
- 46. Types of Uninsured (Over 4 Years) From Pamela Farley Short and Deborah R. Graefe, 2003, Health
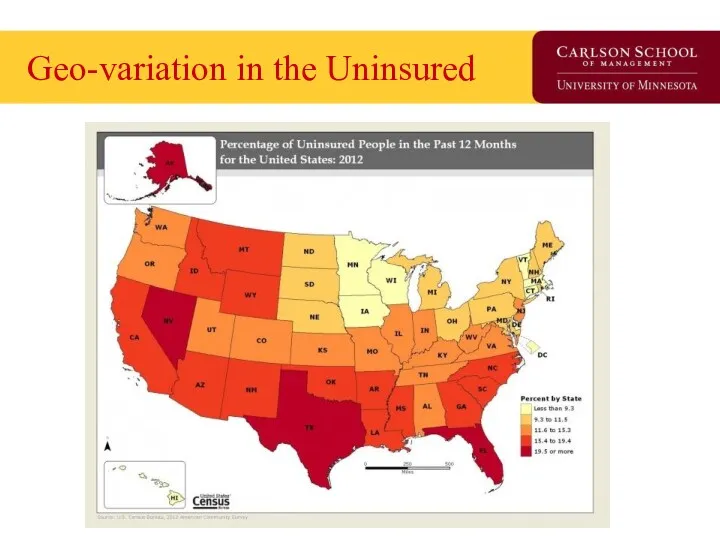
- 47. Geo-variation in the Uninsured
- 48. Does theory square with health insurance today? What is the purpose of insurance? How is modern
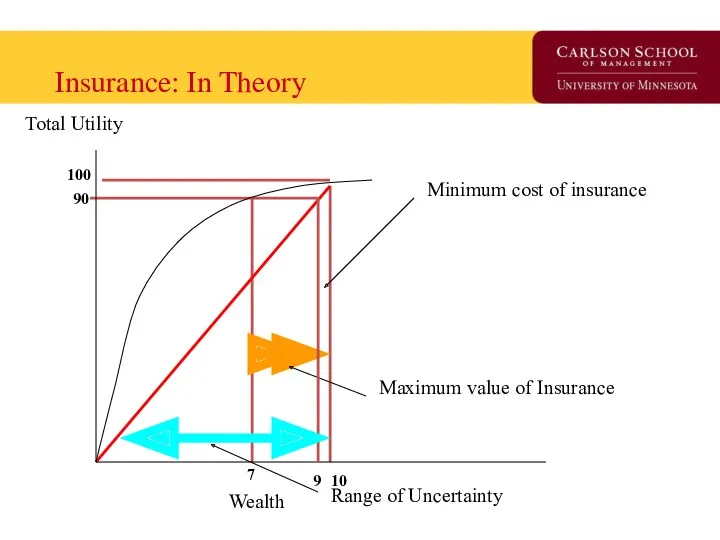
- 49. Insurance: In Theory Maximum value of Insurance Minimum cost of insurance Total Utility Wealth Range of
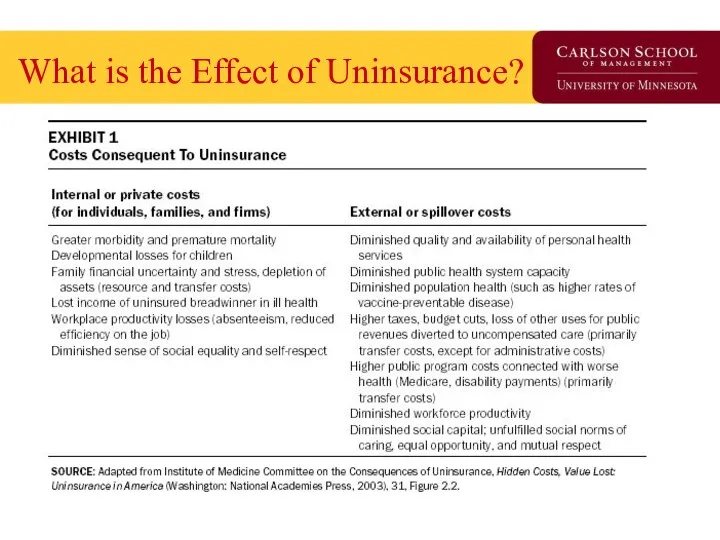
- 50. What is the Effect of Uninsurance?
- 51. One Insurance Reform Option (G.H.W. Bush ’92, M. Romney ’06, and H.R. Clinton & B. Obama
- 52. What has the Uninsured Problem been Proposed to be Addressed? Pay or play Federal effort failed
- 53. What is the minimal form of health insurance you can live with? High-deductible catastrophic Service-specific coverage
- 54. The Free-Rider Problem Free-rider is a person who consumes a good without paying for it. The
- 55. Break
- 56. Health Insurance Market Today Health Economist Health Reform Priors Current Law Overview Coverage and Financing Insurance
- 57. Priors as a Health Economist Health economists find that technology is both good for society and
- 58. Coverage and Financing Coverage: 32 of 54 million uninsured covered 24 million in Exchange 16 million
- 59. Insurance Market: 2010 Effective Immediately: Annual process set by HHS and States for premium rate review.
- 60. NAIC Health Reform Committees HHS is required to consult with the National Association of Insurance Commissioners
- 61. Insurance Market: 2011 Effective January 2011: 80% MLR for individual and small group, 85% MLR for
- 62. New Federal Health Reform Structure -2010 New “Office of Consumer Information and Insurance Oversight” established within
- 63. Exchanges: 2010 Effective July 2010: HHS with States to establish internet portal to identify coverage options.
- 64. Exchanges: 2014 Effective 2014: States to establish Exchange to facilitate comparison shopping, enrollment, and subsidy administration
- 65. Payment Reform & Care Coordination CMS Innovation Center: Created in 2011 to test and expand Medicare
- 66. National Impact of Health Reform Uninsured status is reduced by 59.8% (81% if base is US
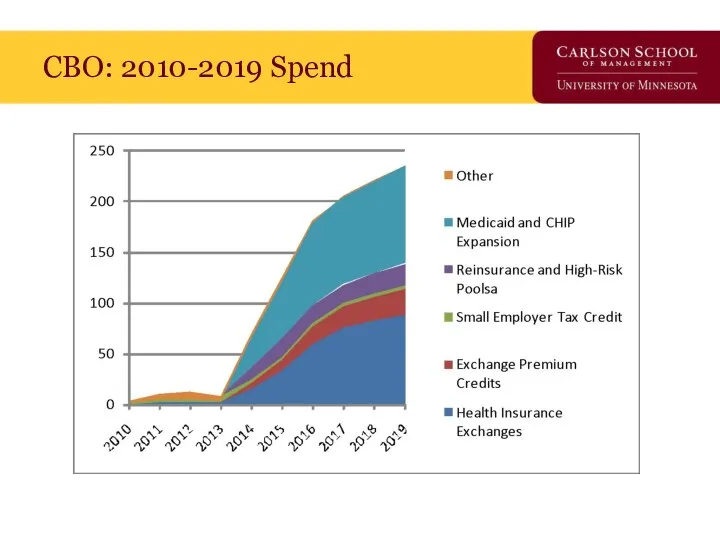
- 67. CBO: 2010-2019 Spend
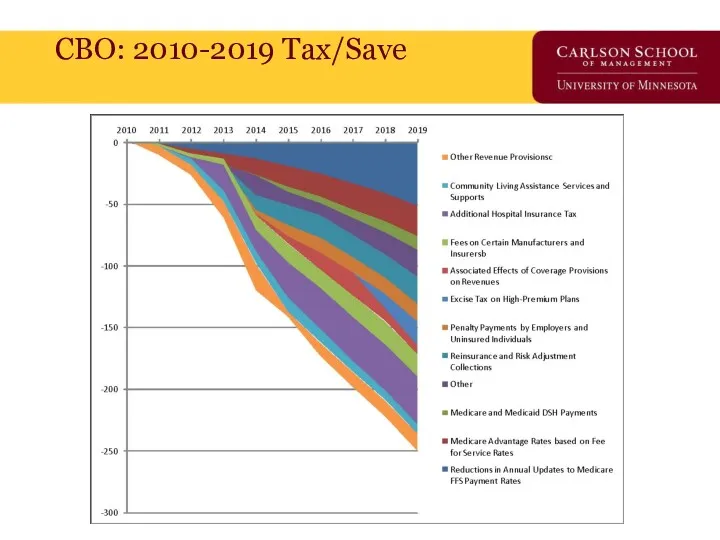
- 68. CBO: 2010-2019 Tax/Save
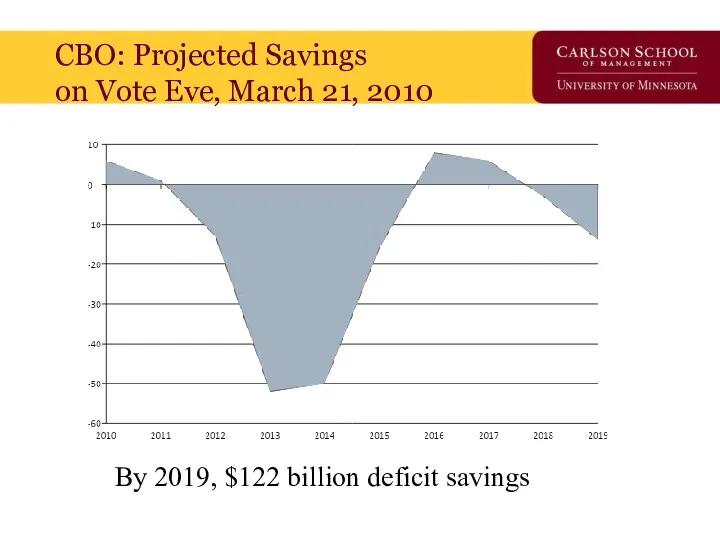
- 69. CBO: Projected Savings on Vote Eve, March 21, 2010 By 2019, $122 billion deficit savings
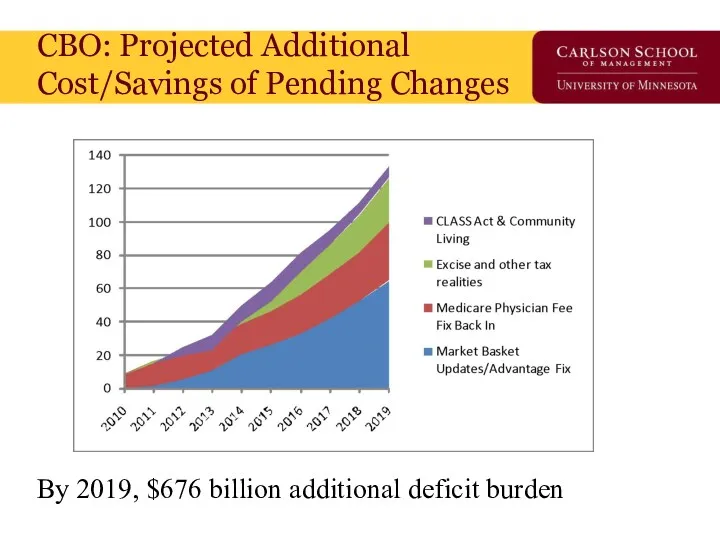
- 70. CBO: Projected Additional Cost/Savings of Pending Changes By 2019, $676 billion additional deficit burden
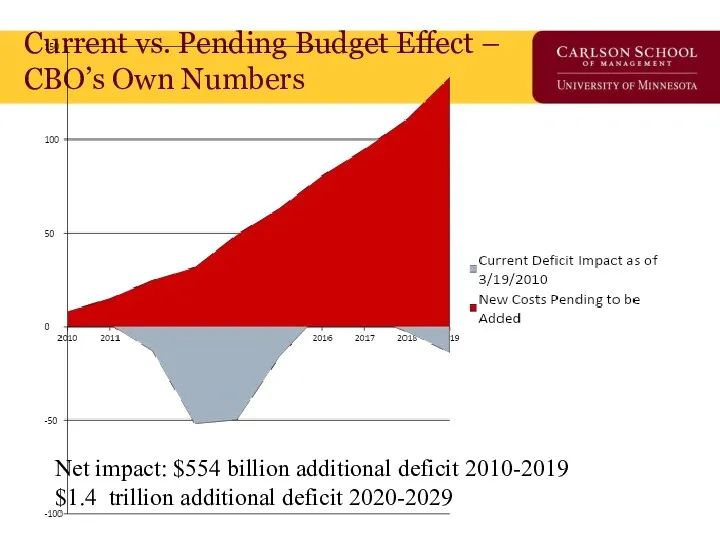
- 71. Current vs. Pending Budget Effect – CBO’s Own Numbers Net impact: $554 billion additional deficit 2010-2019
- 72. Train Wrecks Do Happen In DC But, to be fair, who’s train wreck is it?
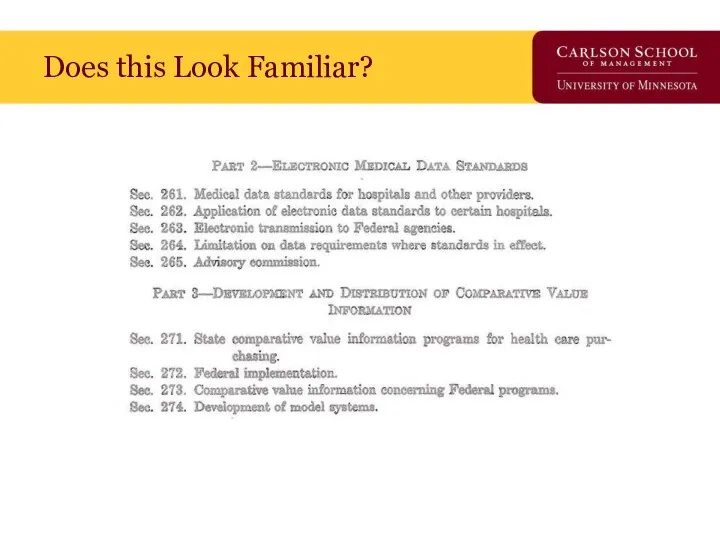
- 73. Does this Look Familiar?
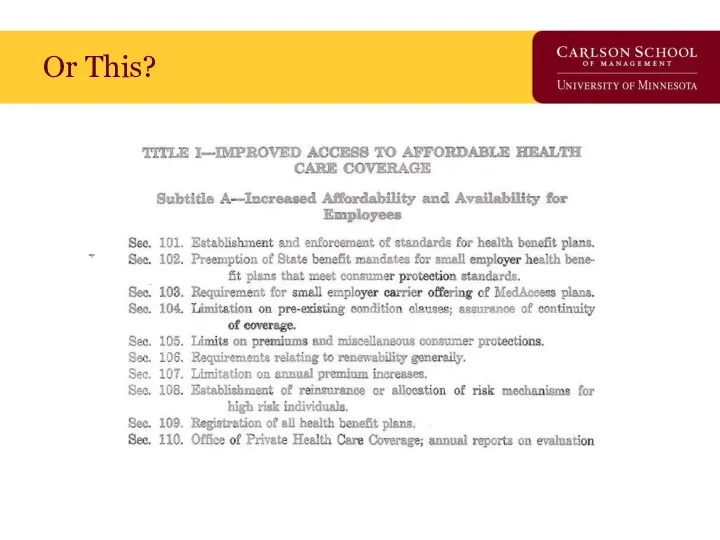
- 74. Or This?
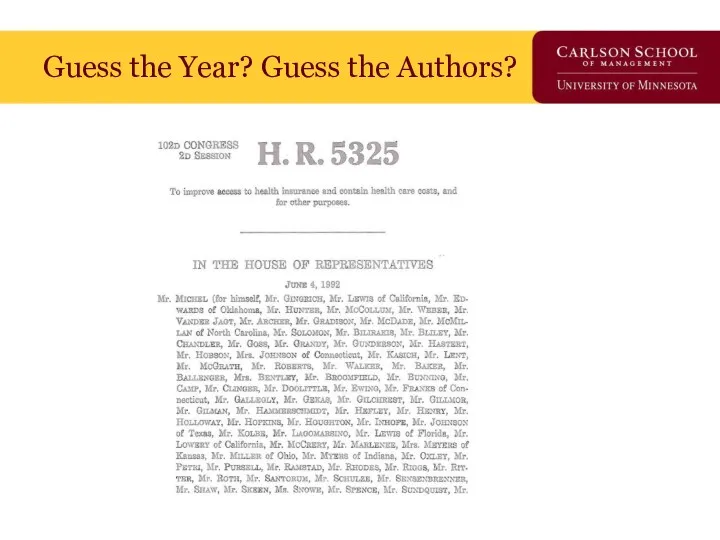
- 75. Guess the Year? Guess the Authors?
- 76. Guess the Year? Guess the Authors?
- 77. Implementation Iceberg Cometh?
- 79. Even Friends can Wound if Implementation Poor
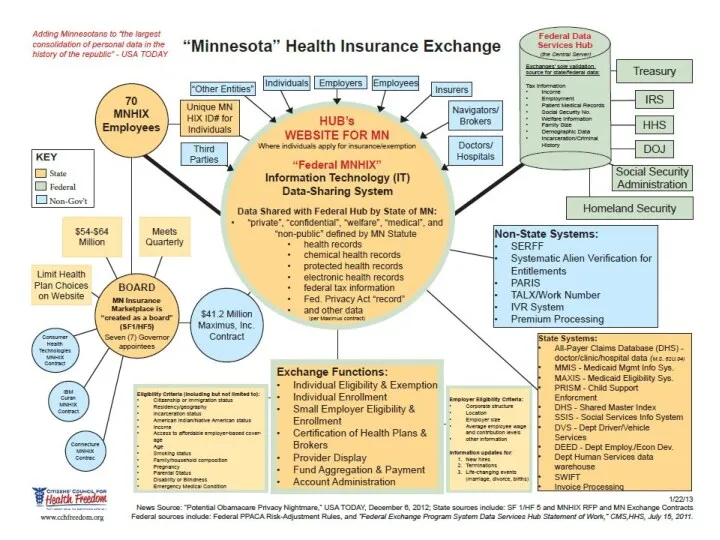
- 80. ACA Privacy Nightmare?
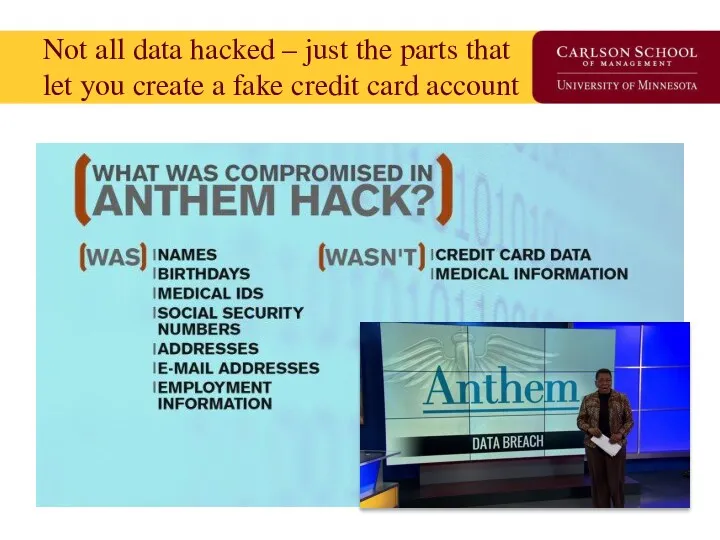
- 81. Not all data hacked – just the parts that let you create a fake credit card
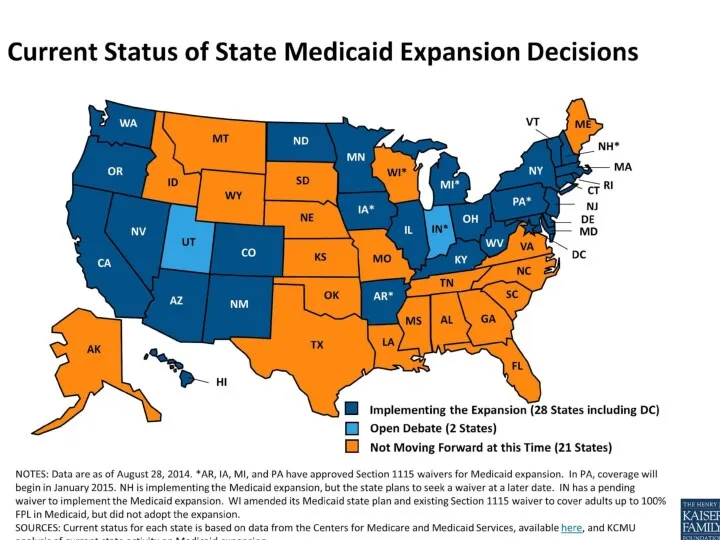
- 82. Major Reform Component – Medicaid Expansion The Act transforms Medicaid into a program to meet the
- 83. Supreme Court Ruling “Gun to the Head” Rationale: “…the financial “inducement” Congress has chosen is much
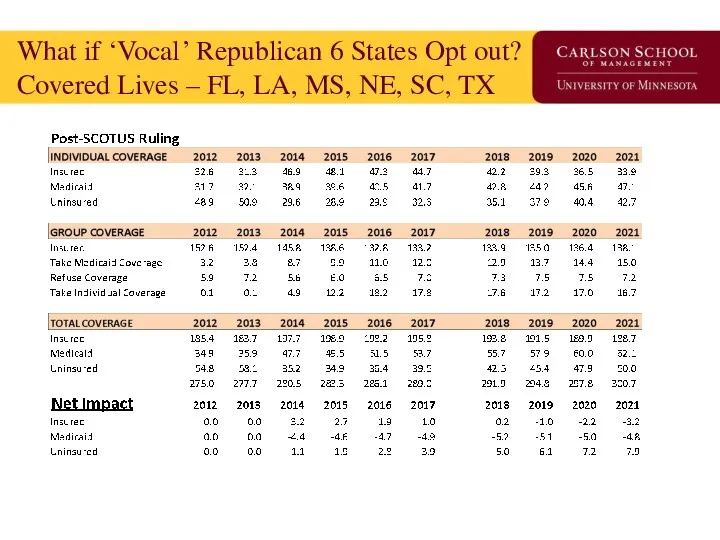
- 85. What if ‘Vocal’ Republican 6 States Opt out? Covered Lives – FL, LA, MS, NE, SC,
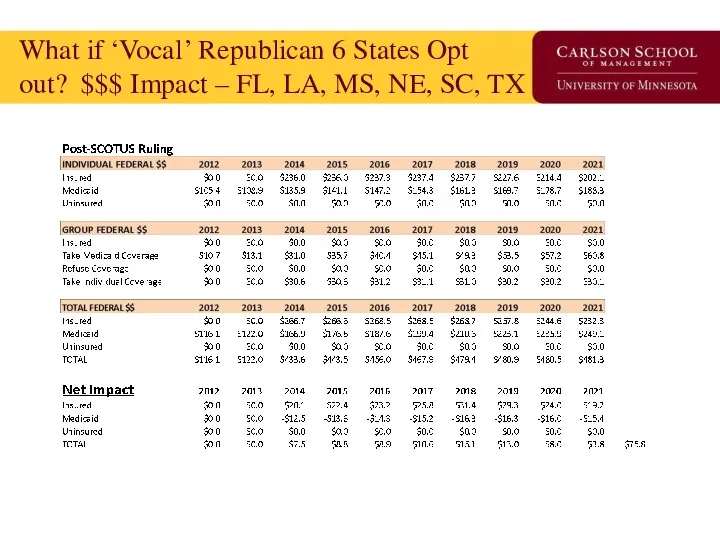
- 86. What if ‘Vocal’ Republican 6 States Opt out? $$$ Impact – FL, LA, MS, NE, SC,
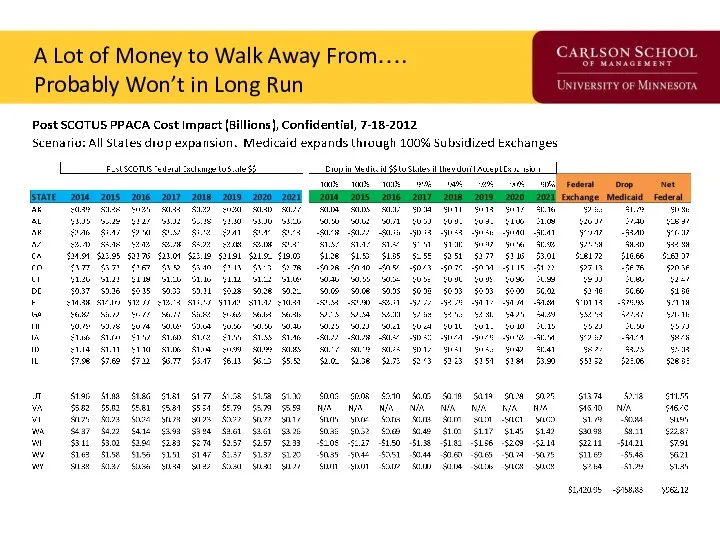
- 87. A Lot of Money to Walk Away From…. Probably Won’t in Long Run
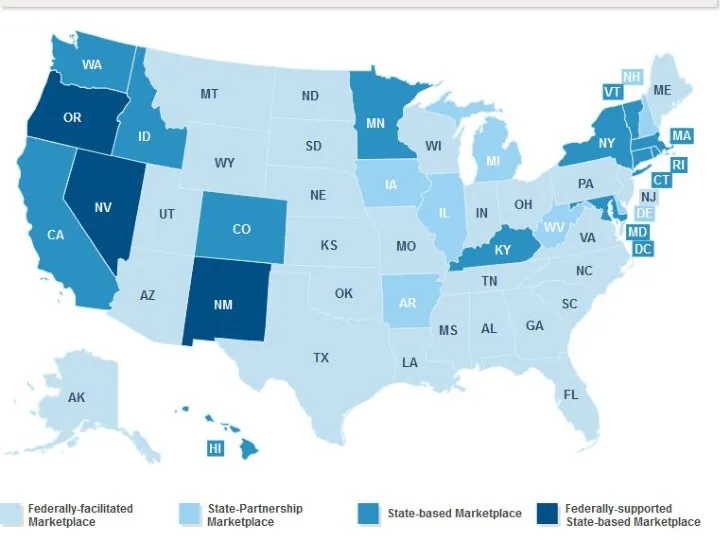
- 88. Next Supreme Court Ruling, June 2015 Are Insurance Subsidies Legal in 34 States using Federal Exchange?
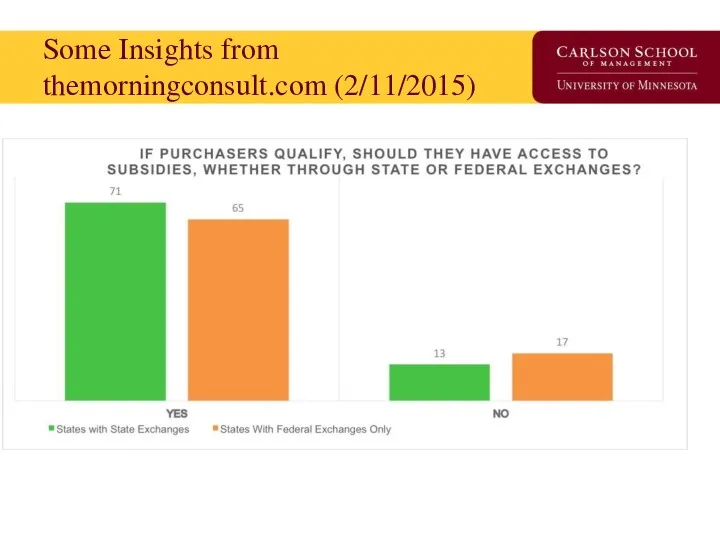
- 90. Some Insights from themorningconsult.com (2/11/2015)
- 91. If Asked: A 21st Century Version of Health Insurance Reform Get actuarially certified risk profiles for
- 92. Supreme Court Decision in June, 2015 on State Exchanges The GOP Unicorn / Replace Plan Trojan
- 93. Closing Thoughts We are going to get a great natural experiment in economics, political science and
- 95. Скачать презентацию
Overview
Next unit up - Insurers
Insurance theory & concepts
Risk & uncertainty
Insurance premiums
Evolution of modern
Overview
Next unit up - Insurers
Insurance theory & concepts
Risk & uncertainty
Insurance premiums
Evolution of modern
Risky Business:
Making Decisions Under Uncertainty
Uncertainty: A situation when more than one event may
Risky Business:
Making Decisions Under Uncertainty
Uncertainty: A situation when more than one event may
Risk Defined
Risk: The probability of incurring a loss (or some other misfortune).
More precisely,
Risk Defined
Risk: The probability of incurring a loss (or some other misfortune).
More precisely,
The Cost of Risk
Some people are willing to bear more risk than others.
In
The Cost of Risk
Some people are willing to bear more risk than others.
In
The Utility of Wealth
The Utility of Wealth
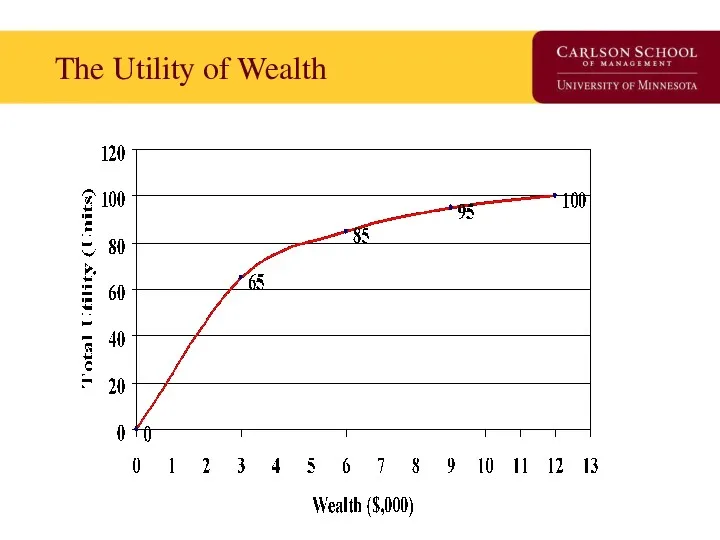
What can we observe from the Utility
of Wealth Schedule?
Utility increases as wealth
What can we observe from the Utility
of Wealth Schedule?
Utility increases as wealth
Translate Utility of Wealth into
Expected Utility
Due to uncertainty, people do not know
Translate Utility of Wealth into
Expected Utility
Due to uncertainty, people do not know
Choice Under Uncertainty
Range of outcomes
Cost of risk
Choice #1: W=$5K
Choice #2: W=$6K
Choice Under Uncertainty
Range of outcomes
Cost of risk
Choice #1: W=$5K
Choice #2: W=$6K
Interpretation of Choice under Uncertainty
At Choice #1, Tania’s wealth is $5K, U=80, no
Interpretation of Choice under Uncertainty
At Choice #1, Tania’s wealth is $5K, U=80, no
Risk Aversion and Risk Neutrality
Risk Averse: Someone who sees risk as not cost-less.
The
Risk Aversion and Risk Neutrality
Risk Averse: Someone who sees risk as not cost-less.
The
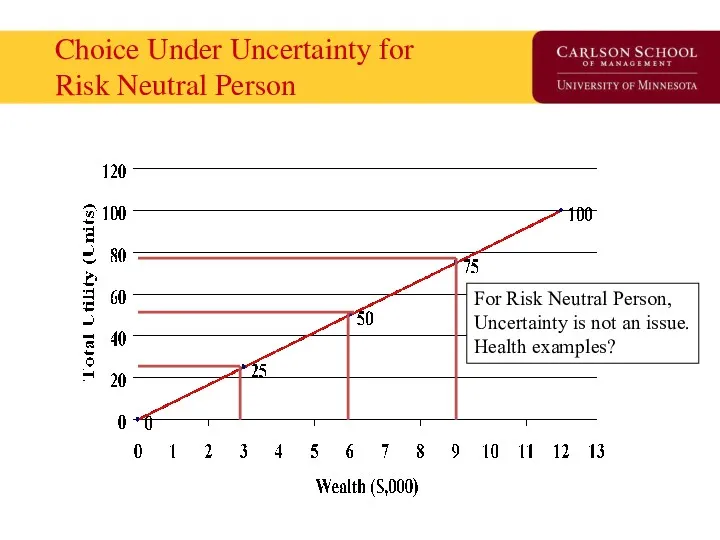
Choice Under Uncertainty for
Risk Neutral Person
For Risk Neutral Person,
Uncertainty is not an
Choice Under Uncertainty for
Risk Neutral Person
For Risk Neutral Person,
Uncertainty is not an
How do we reduce risk?
Buy the ‘the cost of risk’ off. (similar to
How do we reduce risk?
Buy the ‘the cost of risk’ off. (similar to
How does Insurance work?
Insurance works by ‘pooling’ risks.
Insurance is possible and profitable because
How does Insurance work?
Insurance works by ‘pooling’ risks.
Insurance is possible and profitable because
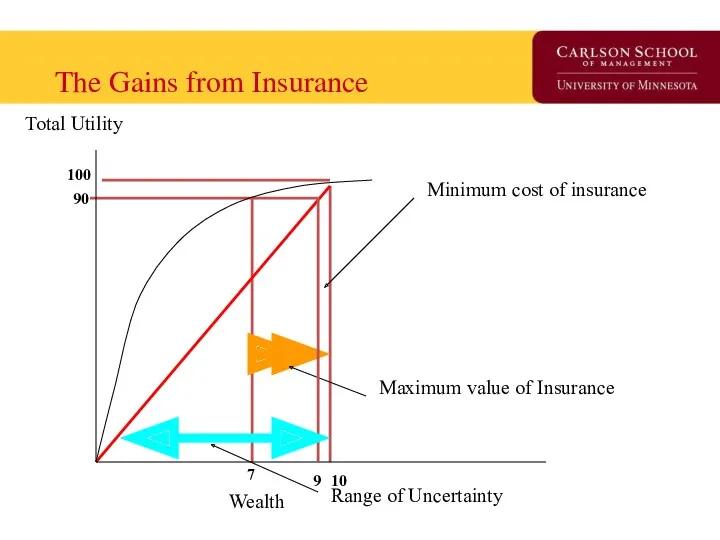
The Gains from Insurance
Maximum value of Insurance
Minimum cost of insurance
Total Utility
Wealth
Range of Uncertainty
100
90
10
7
9
The Gains from Insurance
Maximum value of Insurance
Minimum cost of insurance
Total Utility
Wealth
Range of Uncertainty
100
90
10
7
9
Understanding the Graph
At $10K, utility is 100.
If one loses health (or a another
Understanding the Graph
At $10K, utility is 100.
If one loses health (or a another
Understanding the Graph - 2
Up to what price will you buy insurance?
What will
Understanding the Graph - 2
Up to what price will you buy insurance?
What will
Moral Hazard & Adverse Selection
Private information is information that is available to one
Moral Hazard & Adverse Selection
Private information is information that is available to one
Moral Hazard
Defined: When one of two or more parities with an agreement has
Moral Hazard
Defined: When one of two or more parities with an agreement has
Adverse Selection
Defined: The tendency for people to enter into agreements in which they
Adverse Selection
Defined: The tendency for people to enter into agreements in which they
Understanding the difference between the two
People who face greater risks are more likely
Understanding the difference between the two
People who face greater risks are more likely
How do insurance companies overcome these problems?
Find a signal to convey information from
How do insurance companies overcome these problems?
Find a signal to convey information from
Examine Evolution of a Market
Using the “Time Machine” from Davey & Goliath
Examine Evolution of a Market
Using the “Time Machine” from Davey & Goliath
Slow Day? Starr got you down?
Consider….
http://www.awn.com/heaven_and_hell/DG/DG4.htm
Slow Day? Starr got you down?
Consider….
http://www.awn.com/heaven_and_hell/DG/DG4.htm
Early Public Health Insurance
First instance of public insurance is Germany’s 1883 ‘compulsory
Early Public Health Insurance
First instance of public insurance is Germany’s 1883 ‘compulsory
U.S. Public Health Insurance
Failed proposals made in Congress for National Health Insurance:
1918-19
1935-36
1948
1974
1993-94
Successful
U.S. Public Health Insurance
Failed proposals made in Congress for National Health Insurance:
1918-19
1935-36
1948
1974
1993-94
Successful
Private Insurance – Two early models
Fee-for-service insurance
Epitomized by Blue Cross plan started for
Private Insurance – Two early models
Fee-for-service insurance
Epitomized by Blue Cross plan started for
Four characteristics of Blue Cross/Blue Shield fundamentally shaped American health care.
Hospitals were
Four characteristics of Blue Cross/Blue Shield fundamentally shaped American health care.
Hospitals were
Points of Inflection in
Insurance Market -1
1930s – Great Depression reduces physician’s opposition
Points of Inflection in
Insurance Market -1
1930s – Great Depression reduces physician’s opposition
Points of Inflection in
Insurance Market - 2
1983 – Medicare institutes prospective payment
Points of Inflection in
Insurance Market - 2
1983 – Medicare institutes prospective payment
State of Health Insurance Today
Insurance models
Demand side control programs
Supply side control programs
Market
State of Health Insurance Today
Insurance models
Demand side control programs
Supply side control programs
Market
Insurance Models in 2007
9% Conventional Fee for Service/Managed Indemnity
Payment is based on a
Insurance Models in 2007
9% Conventional Fee for Service/Managed Indemnity
Payment is based on a
2013: ACA Accelerated HDHP - Distribution of Health Plan
Enrollment for Covered Workers,
2013: ACA Accelerated HDHP - Distribution of Health Plan Enrollment for Covered Workers,
Insurance Tower of Babel
PPO: Preferred Provider Organization (Medica)
IDS: Integrated Delivery System (Fairview)
HMO:
Insurance Tower of Babel
PPO: Preferred Provider Organization (Medica)
IDS: Integrated Delivery System (Fairview)
HMO:
CDHP Business Enablers
‘Ready to Lease’ Components of Health Insurance:
Electronic claims processing
National panel
CDHP Business Enablers
‘Ready to Lease’ Components of Health Insurance:
Electronic claims processing
National panel
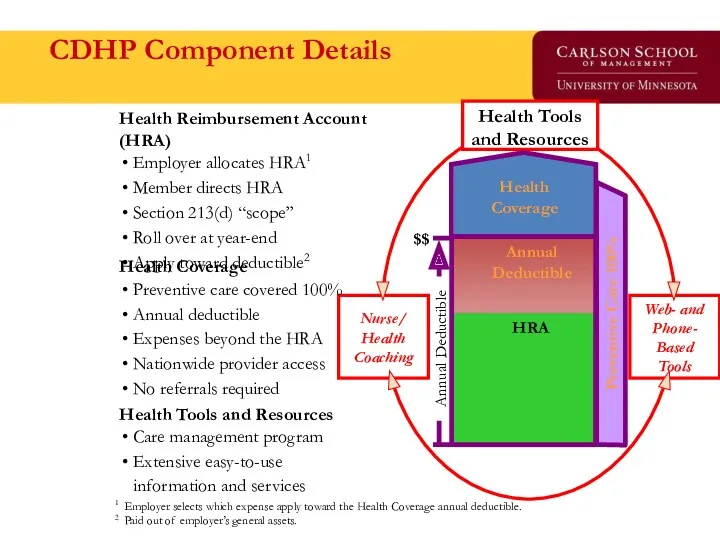
CDHP Component Details
Health Tools and Resources
Care management program
Extensive easy-to-use
information and services
Health Coverage
Preventive
CDHP Component Details
Health Tools and Resources
Care management program
Extensive easy-to-use
information and services
Health Coverage
Preventive
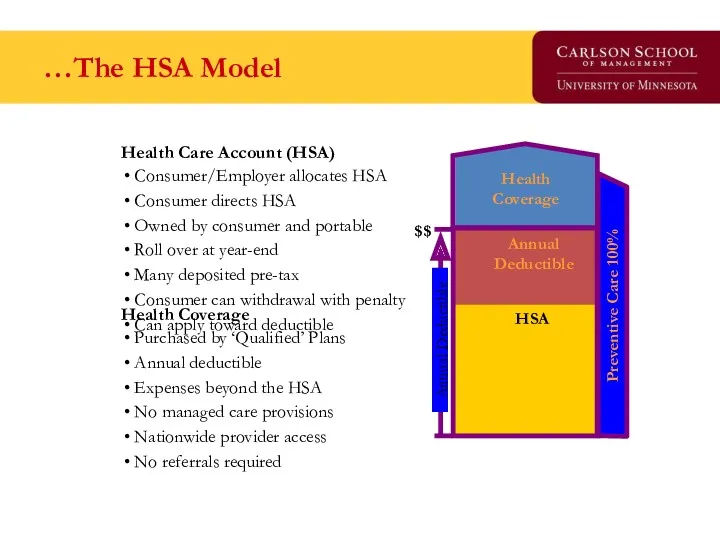
…The HSA Model
Health Coverage
Purchased by ‘Qualified’ Plans
Annual deductible
Expenses beyond the HSA
No managed care
…The HSA Model
Health Coverage
Purchased by ‘Qualified’ Plans
Annual deductible
Expenses beyond the HSA
No managed care
Demand Side Controls
‘Affect the consumer to mitigate moral hazard’
Coinsurance, Copayments, Deductibles
Specialist access through
Demand Side Controls
‘Affect the consumer to mitigate moral hazard’
Coinsurance, Copayments, Deductibles
Specialist access through
Supply Side Controls
‘Reduce the probability of provider induced demand’
Fee schedules
Diagnosis Related Groups
RBRVS
Outpatient
Supply Side Controls
‘Reduce the probability of provider induced demand’
Fee schedules
Diagnosis Related Groups
RBRVS
Outpatient
Insurance ‘Market Success’
Primary funding source of medical innovation in the United States.
Consumers have
Insurance ‘Market Success’
Primary funding source of medical innovation in the United States.
Consumers have
Insurance ‘Market Failures’
50+ million uninsured (at any point in time) prior to ACA
120%
Insurance ‘Market Failures’
50+ million uninsured (at any point in time) prior to ACA
120%
Average Annual Premiums for Single and Family Coverage, 1999-2013
* Estimate is statistically different
Average Annual Premiums for Single and Family Coverage, 1999-2013
* Estimate is statistically different
Question for Reflection
How uniquely American is evolution of the insurance market in the
Question for Reflection
How uniquely American is evolution of the insurance market in the
The Uninsured Problem
Who are the uninsured?
Why is this a ‘market failure’?
If government were
The Uninsured Problem
Who are the uninsured?
Why is this a ‘market failure’?
If government were
Who Are the Uninsured?
Who Are the Uninsured?
Types of Uninsured (Over 4 Years)
From Pamela Farley Short and Deborah R. Graefe,
Types of Uninsured (Over 4 Years)
From Pamela Farley Short and Deborah R. Graefe,
Geo-variation in the Uninsured
Geo-variation in the Uninsured
Does theory square with
health insurance today?
What is the purpose of insurance?
How is
Does theory square with
health insurance today?
What is the purpose of insurance?
How is
Insurance: In Theory
Maximum value of Insurance
Minimum cost of insurance
Total Utility
Wealth
Range of Uncertainty
100
90
10
7
9
Insurance: In Theory
Maximum value of Insurance
Minimum cost of insurance
Total Utility
Wealth
Range of Uncertainty
100
90
10
7
9
What is the Effect of Uninsurance?
What is the Effect of Uninsurance?
One Insurance Reform Option
(G.H.W. Bush ’92, M. Romney ’06, and
H.R. Clinton & B.
One Insurance Reform Option (G.H.W. Bush ’92, M. Romney ’06, and H.R. Clinton & B.
What has the Uninsured Problem been
Proposed to be Addressed?
Pay or play
Federal
What has the Uninsured Problem been
Proposed to be Addressed?
Pay or play
Federal
What is the minimal form of health insurance you can live with?
High-deductible catastrophic
Service-specific
What is the minimal form of health insurance you can live with?
High-deductible catastrophic
Service-specific
The Free-Rider Problem
Free-rider is a person who consumes a good without paying for
The Free-Rider Problem
Free-rider is a person who consumes a good without paying for
Break
Break
Health Insurance Market Today
Health Economist Health Reform Priors
Current Law Overview
Coverage and Financing
Insurance Markets
Exchanges
Payment
Health Insurance Market Today
Health Economist Health Reform Priors
Current Law Overview
Coverage and Financing
Insurance Markets
Exchanges
Payment
Priors as a Health Economist
Health economists find that technology is both good for
Priors as a Health Economist
Health economists find that technology is both good for
Coverage and Financing
Coverage: 32 of 54 million uninsured covered
24 million in Exchange
16
Coverage and Financing
Coverage: 32 of 54 million uninsured covered
24 million in Exchange
16
Insurance Market: 2010
Effective Immediately: Annual process set by HHS and States for premium
Insurance Market: 2010
Effective Immediately: Annual process set by HHS and States for premium
NAIC Health Reform Committees
HHS is required to consult with the National Association
NAIC Health Reform Committees
HHS is required to consult with the National Association
Insurance Market: 2011
Effective January 2011: 80% MLR for individual and small group, 85%
Insurance Market: 2011
Effective January 2011: 80% MLR for individual and small group, 85%
New Federal Health Reform
Structure -2010
New “Office of Consumer Information and Insurance Oversight” established
New Federal Health Reform
Structure -2010
New “Office of Consumer Information and Insurance Oversight” established
Exchanges: 2010
Effective July 2010: HHS with States to establish internet portal to identify
Exchanges: 2010
Effective July 2010: HHS with States to establish internet portal to identify
Exchanges: 2014
Effective 2014: States to establish Exchange to facilitate comparison shopping, enrollment, and
Exchanges: 2014
Effective 2014: States to establish Exchange to facilitate comparison shopping, enrollment, and
Payment Reform &
Care Coordination
CMS Innovation Center: Created in 2011 to test and
Payment Reform &
Care Coordination
CMS Innovation Center: Created in 2011 to test and
National Impact of Health Reform
Uninsured status is reduced by 59.8% (81% if base
National Impact of Health Reform
Uninsured status is reduced by 59.8% (81% if base
CBO: 2010-2019 Spend
CBO: 2010-2019 Spend
CBO: 2010-2019 Tax/Save
CBO: 2010-2019 Tax/Save
CBO: Projected Savings
on Vote Eve, March 21, 2010
By 2019, $122 billion deficit
CBO: Projected Savings
on Vote Eve, March 21, 2010
By 2019, $122 billion deficit
CBO: Projected Additional
Cost/Savings of Pending Changes
By 2019, $676 billion additional deficit burden
CBO: Projected Additional
Cost/Savings of Pending Changes
By 2019, $676 billion additional deficit burden
Current vs. Pending Budget Effect –
CBO’s Own Numbers
Net impact: $554 billion additional
Current vs. Pending Budget Effect –
CBO’s Own Numbers
Net impact: $554 billion additional
Train Wrecks Do Happen In DC
But, to be fair, who’s train wreck is
Train Wrecks Do Happen In DC
But, to be fair, who’s train wreck is
Does this Look Familiar?
Does this Look Familiar?
Or This?
Or This?
Guess the Year? Guess the Authors?
Guess the Year? Guess the Authors?
Guess the Year? Guess the Authors?
Guess the Year? Guess the Authors?
Implementation Iceberg Cometh?
Implementation Iceberg Cometh?

Even Friends can Wound if
Implementation Poor
Even Friends can Wound if
Implementation Poor
ACA Privacy Nightmare?
ACA Privacy Nightmare?

Not all data hacked – just the parts that
let you create a
Not all data hacked – just the parts that let you create a
Major Reform Component –
Medicaid Expansion
The Act transforms Medicaid into a program to meet
Major Reform Component –
Medicaid Expansion
The Act transforms Medicaid into a program to meet
Supreme Court Ruling
“Gun to the Head”
Rationale:
“…the financial “inducement” Congress has chosen is much
Supreme Court Ruling
“Gun to the Head”
Rationale:
“…the financial “inducement” Congress has chosen is much
What if ‘Vocal’ Republican 6 States Opt out?
Covered Lives – FL, LA,
What if ‘Vocal’ Republican 6 States Opt out? Covered Lives – FL, LA,
What if ‘Vocal’ Republican 6 States Opt
out? $$$ Impact – FL, LA,
What if ‘Vocal’ Republican 6 States Opt out? $$$ Impact – FL, LA,
A Lot of Money to Walk Away From….
Probably Won’t in Long Run
A Lot of Money to Walk Away From….
Probably Won’t in Long Run
Next Supreme Court Ruling, June 2015
Are Insurance Subsidies Legal in 34 States using
Next Supreme Court Ruling, June 2015 Are Insurance Subsidies Legal in 34 States using
Some Insights from
themorningconsult.com (2/11/2015)
Some Insights from
themorningconsult.com (2/11/2015)
If Asked: A 21st Century Version of Health Insurance Reform
Get actuarially certified risk
If Asked: A 21st Century Version of Health Insurance Reform
Get actuarially certified risk
Supreme Court Decision in June, 2015 on State Exchanges
The GOP Unicorn / Replace
Supreme Court Decision in June, 2015 on State Exchanges
The GOP Unicorn / Replace
Closing Thoughts
We are going to get a great natural experiment in economics, political
Closing Thoughts
We are going to get a great natural experiment in economics, political
 Индивид в организации
Индивид в организации Структура и основной сортамент продукции ОАО ММК. Численность кадрового состава
Структура и основной сортамент продукции ОАО ММК. Численность кадрового состава Управление и моделирование бизнес-процессами
Управление и моделирование бизнес-процессами История развития менеджмента в России
История развития менеджмента в России Стратегии масштабирования бизнеса
Стратегии масштабирования бизнеса Научный менеджмент в России в первой половине XX века
Научный менеджмент в России в первой половине XX века Первые научные теории управления
Первые научные теории управления КБ Ренессанс кредит. ООО Поиск клининговой компании для офиса в г. Москва
КБ Ренессанс кредит. ООО Поиск клининговой компании для офиса в г. Москва Методы отбора персонала в организации
Методы отбора персонала в организации Основы коммуникации
Основы коммуникации Сущность организационного поведения
Сущность организационного поведения Nonverbal intercultural communication
Nonverbal intercultural communication Көлік логистикасы слайд-дәрісі мамандығы үшін тасымалды ұйымдастыру, қозғалысты басқару
Көлік логистикасы слайд-дәрісі мамандығы үшін тасымалды ұйымдастыру, қозғалысты басқару Действия бортпроводников. Вопросы брифинга и инструктажи
Действия бортпроводников. Вопросы брифинга и инструктажи Этапы рационального решения проблем
Этапы рационального решения проблем Мотивация сотрудников. Сектора обслуживания дебетовых карт
Мотивация сотрудников. Сектора обслуживания дебетовых карт Диаграмма Исикавы и Парето
Диаграмма Исикавы и Парето Onboarding сотрудников в ГК СНЕГ
Onboarding сотрудников в ГК СНЕГ Дерево решений
Дерево решений Концепція менеджменту заінтересованих сторін
Концепція менеджменту заінтересованих сторін Инструменты для ведения открытого диалога с клиентом
Инструменты для ведения открытого диалога с клиентом Стратегическое управление: необходимость, сущность, этапы. Лекция 1
Стратегическое управление: необходимость, сущность, этапы. Лекция 1 Эффективное трудоустройство. Программа тренинга
Эффективное трудоустройство. Программа тренинга Инструкция по навигации и оформлению офиса
Инструкция по навигации и оформлению офиса Цель и задачи современной службы управления персоналом
Цель и задачи современной службы управления персоналом Система государственного управления. Лекция 3
Система государственного управления. Лекция 3 Major building systems
Major building systems Создать стандарт
Создать стандарт