- Processes of Respiration

Содержание
- 2. Processes of Respiration Respiration (exchange of gases between atmosphere and body’s cells) involves four processes Pulmonary
- 3. Processes of Respiration Net movement of respiratory gases Air containing O2 is inhaled into alveoli during
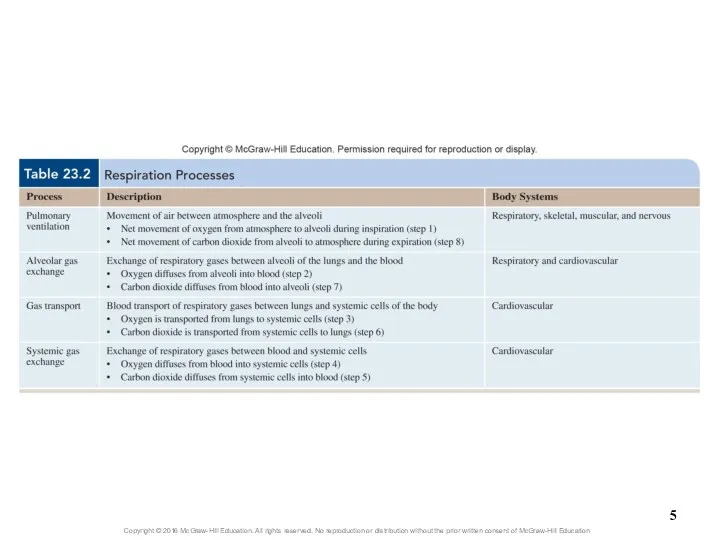
- 4. Overview of Respiration Figure 23.18
- 6. 23.5 Respiration: Pulmonary Ventilation Give an overview of the process of pulmonary ventilation. Explain how pressure
- 7. 23.5 Respiration: Pulmonary Ventilation (continued) Explain the physiologic events associated with controlling quiet breathing. Explain the
- 8. 23.5 Respiration: Pulmonary Ventilation (continued) Distinguish between pulmonary ventilation and alveolar ventilation, and discuss the significance
- 9. 23.5a Introduction to Pulmonary Ventilation Pulmonary ventilation (breathing): air movement Consists of two cyclic phases Inspiration
- 10. 23.5b Mechanics of Breathing Involve several integrated aspects Specific actions of skeletal muscles of breathing Dimensional
- 11. 23.5b Mechanics of Breathing Skeletal muscles of breathing Muscles of quiet breathing Diaphragm and external intercostals
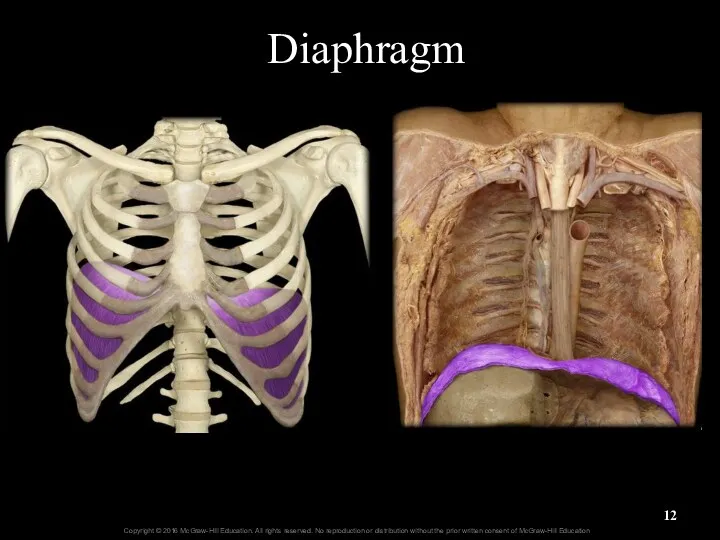
- 12. Diaphragm
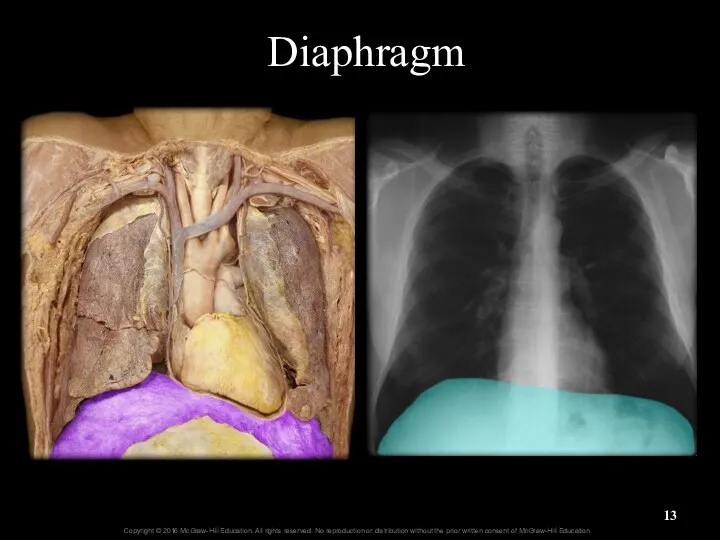
- 13. Diaphragm
- 14. Phrenic Nerve—Diaphragm
- 15. External Intercostals
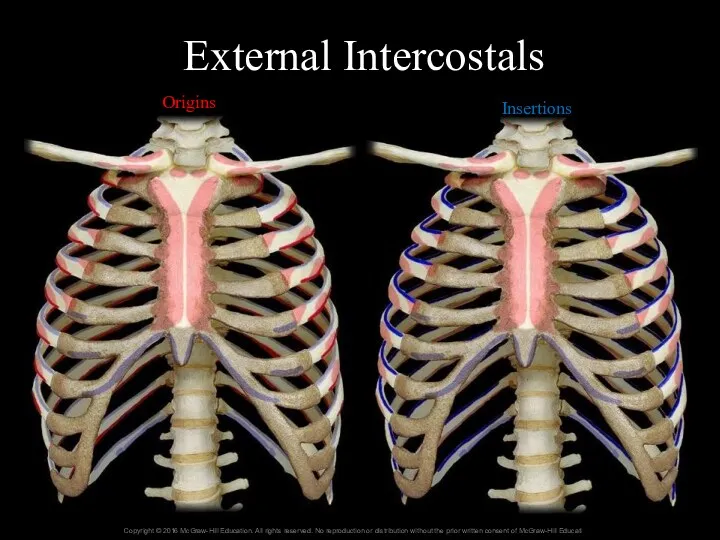
- 16. External Intercostals Origins Insertions
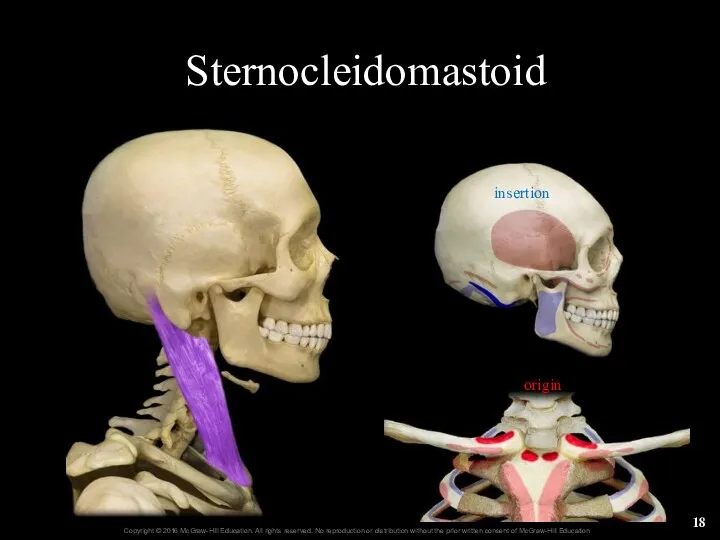
- 17. Sternocleidomastoid
- 18. Sternocleidomastoid origin insertion
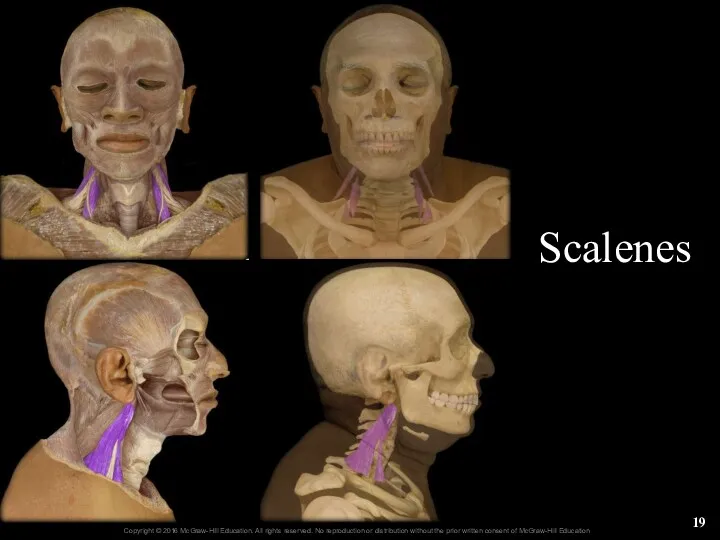
- 19. Scalenes 22-
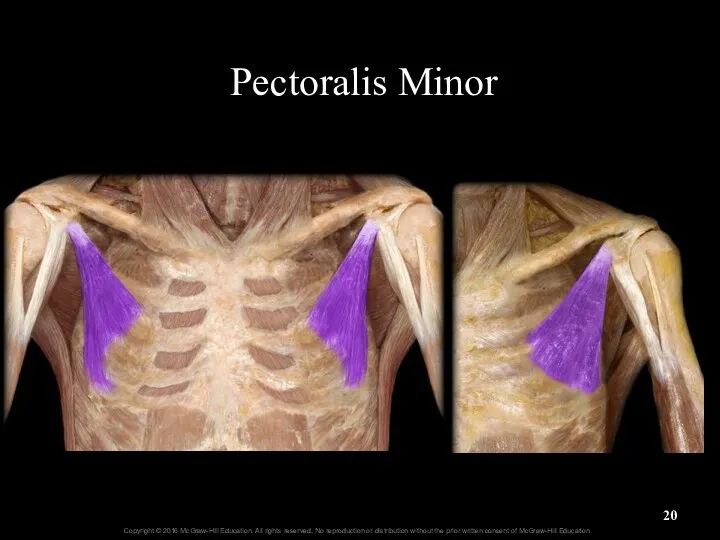
- 20. Pectoralis Minor
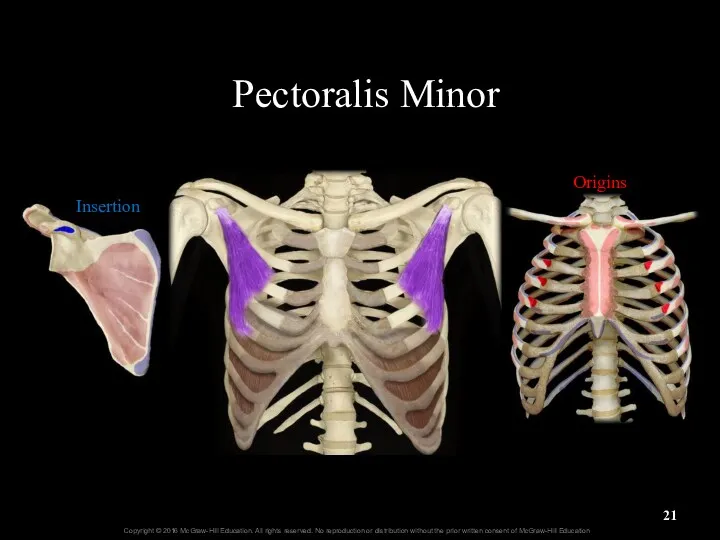
- 21. Pectoralis Minor Insertion Origins
- 22. Serratus Posterior Superior serrate = scalloped or zigzag
- 23. Erector Spinae origin insertion
- 24. Iliocostalis of Erector Spinae
- 25. Longissimus of Erector Spinae origin insertion
- 26. Spinalis of Erector Spinae origin insertion
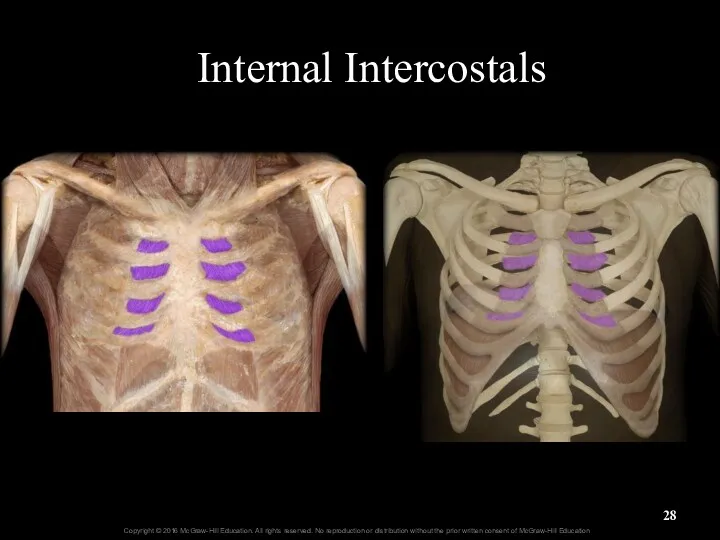
- 27. 23.5b Mechanics of Breathing Skeletal muscles of breathing (continued) Muscles of forced expiration Include internal intercostals,
- 28. Internal Intercostals
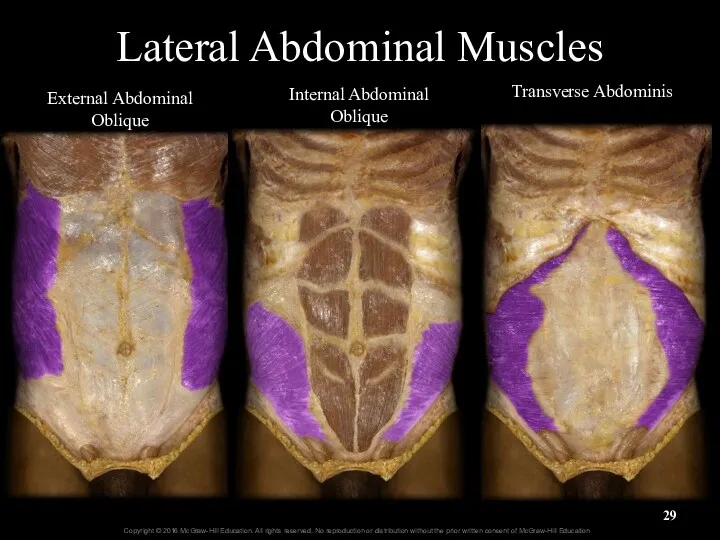
- 29. Lateral Abdominal Muscles External Abdominal Oblique Internal Abdominal Oblique Transverse Abdominis
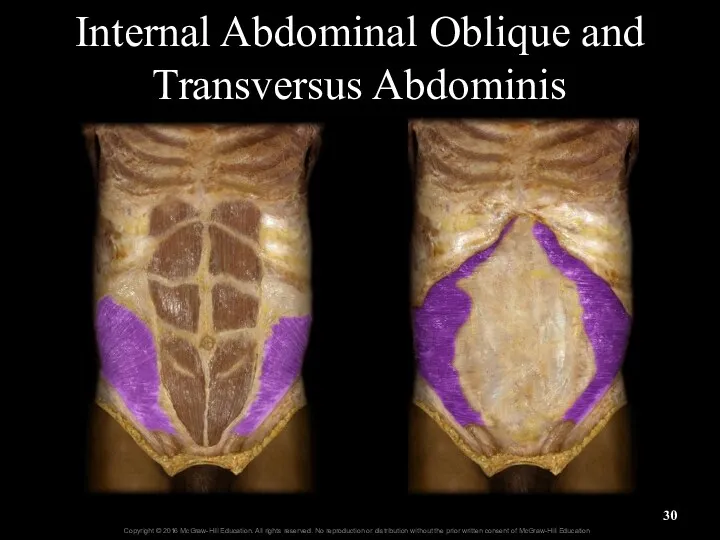
- 30. Internal Abdominal Oblique and Transversus Abdominis
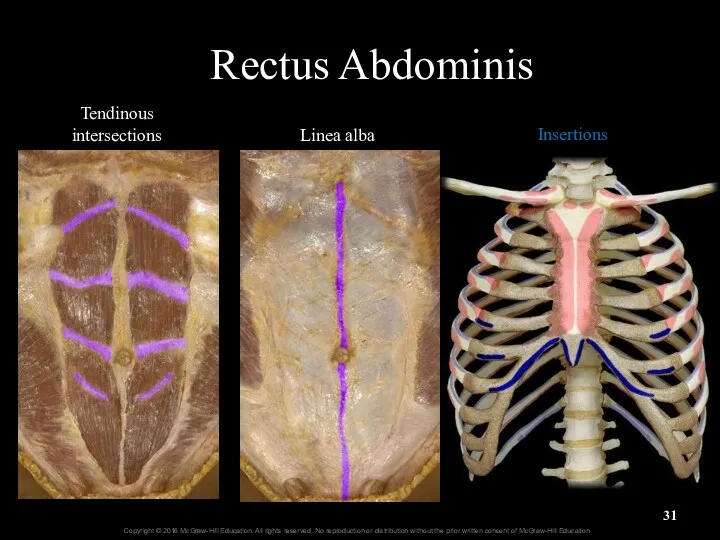
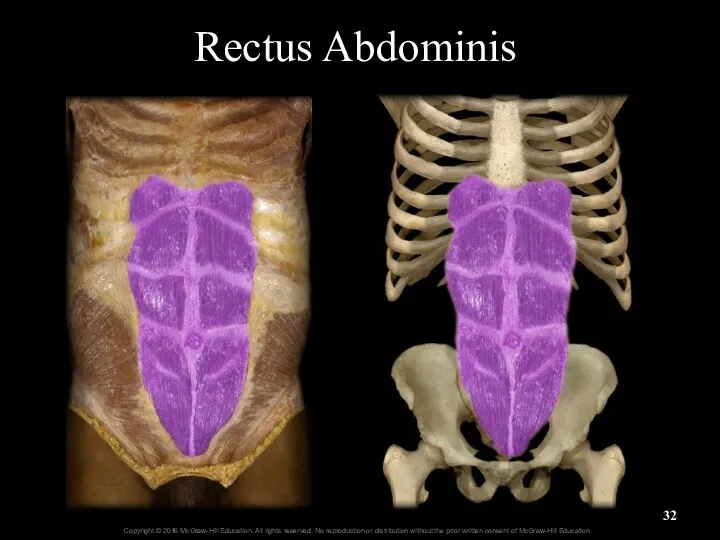
- 31. Rectus Abdominis Tendinous intersections Linea alba Insertions
- 32. Rectus Abdominis
- 33. Serratus Posterior Inferior serrate = scalloped or zigzag
- 34. Skeletal Muscles of Breathing Figure 23.19-top
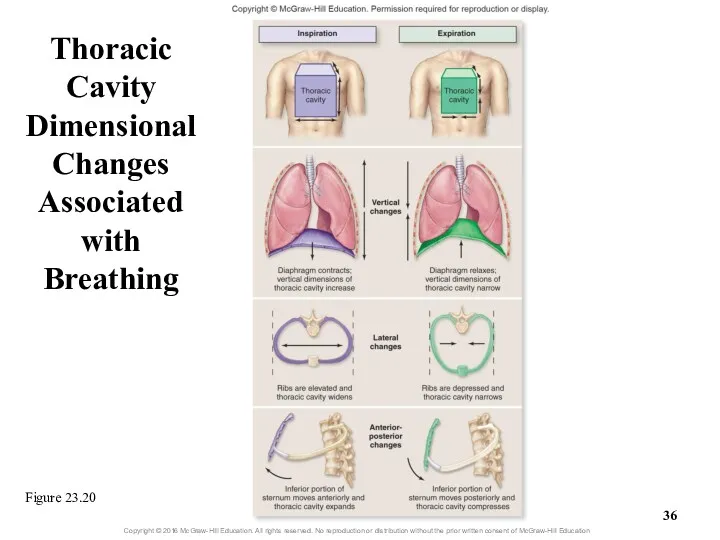
- 35. 23.5b Mechanics of Breathing Volume changes in the thoracic cavity Thoracic volume changes vertically, laterally, and
- 36. Thoracic Cavity Dimensional Changes Associated with Breathing Figure 23.20
- 37. 23.5b Mechanics of Breathing Volume changes in the thoracic cavity (continued) Lateral dimension changes Rib cage
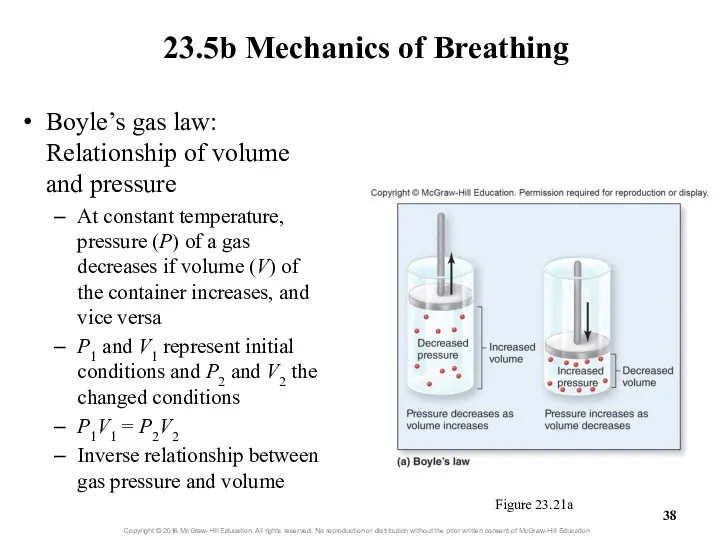
- 38. Boyle’s gas law: Relationship of volume and pressure At constant temperature, pressure (P) of a gas
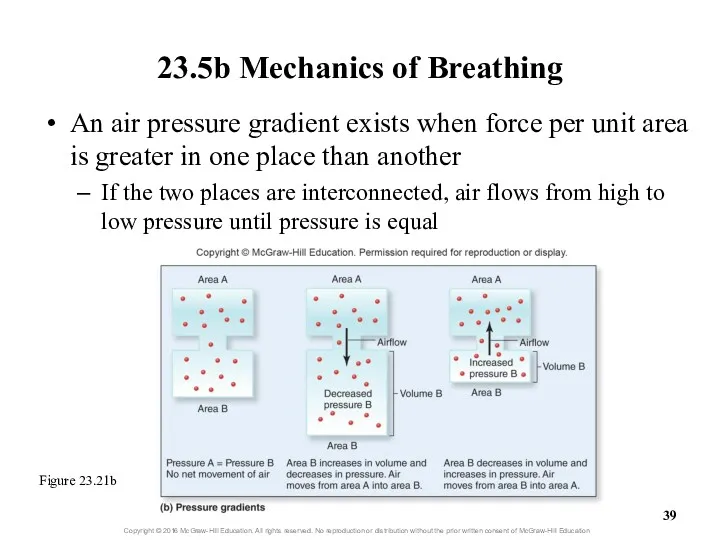
- 39. 23.5b Mechanics of Breathing An air pressure gradient exists when force per unit area is greater
- 40. 23.5b Mechanics of Breathing Volumes and pressures associated with breathing Atmospheric pressure: pressure of air in
- 41. 23.5b Mechanics of Breathing Volumes and pressures associated with breathing (cont’d.) Intrapleural pressure: pressure in pleural
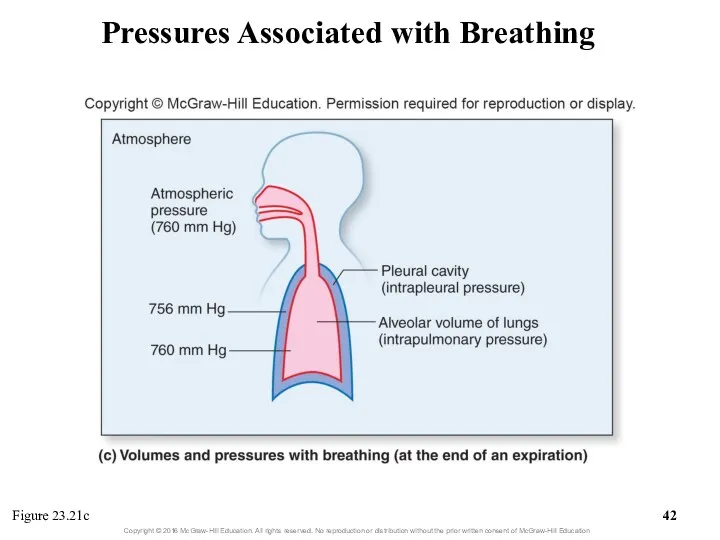
- 42. Pressures Associated with Breathing Figure 23.21c
- 43. 23.5b Mechanics of Breathing Quiet breathing: Inspiration Intrapulmonary pressure and atmospheric pressure are initially equal (760
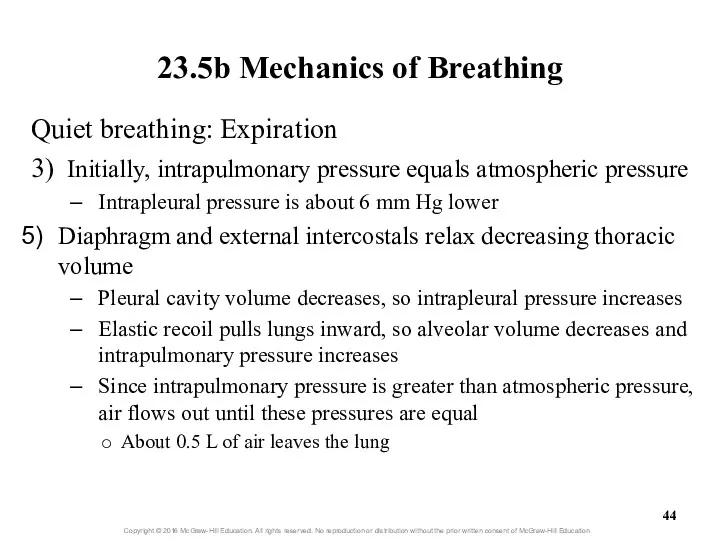
- 44. 23.5b Mechanics of Breathing Quiet breathing: Expiration 3) Initially, intrapulmonary pressure equals atmospheric pressure Intrapleural pressure
- 45. Volume and Pressure Changes During Quiet Breathing Figure 23.22a
- 46. Volume and Pressure Changes During Quiet Breathing Figure 23.22b-c
- 48. 23.5b Mechanics of Breathing Forced breathing Involves steps similar to quiet breathing Requires contraction of additional
- 49. 23.5c Nervous Control of Breathing Autonomic nuclei within the brain coordinate breathing Respiratory center of the
- 50. Neural Control of Breathing Medulla oblongata Pons
- 51. 23.5c Nervous Control of Breathing Chemoreceptors monitor changes in concentrations of H+, PCO2 and PO2 Central
- 52. 23.5c Nervous Control of Breathing Other receptors also influence respiration Proprioceptors of muscles and joints are
- 53. Figure 23.23 Respiratory Center
- 54. 23.5c Nervous Control of Breathing Physiology of quiet breathing Inspiration begins when VRG inspiratory neurons fire
- 55. 23.5c Nervous Control of Breathing Physiology of quiet breathing (continued) Respiration rate for normal, quiet breathing
- 56. Clinical View: Apnea Apnea = absence of breathing Can occur voluntarily Swallowing or holding your breath
- 57. 23.5c Nervous Control of Breathing Reflexes that alter breathing rate and depth Chemoreceptors alter breathing by
- 58. 23.5c Nervous Control of Breathing Reflexes that alter breathing rate and depth (cont’d.) Blood PCO2 is
- 59. Clinical View: Hypoxic Drive Normally the most important stimulus affecting breathing rate and depth is blood
- 60. 23.5c Nervous Control of Breathing Reflexes that alter breathing rate and depth (cont’d.) Altering breathing through
- 61. 23.5c Nervous Control of Breathing Reflexes that alter breathing rate and depth (cont’d.) Action of higher
- 62. 23.5c Nervous Control of Breathing Nervous control of respiratory system structures and breathing structures Respiratory system
- 63. 23.5d Airflow, Pressure Gradients, and Resistance Airflow: amount of air moving in and out of lungs
- 64. 23.5d Airflow, Pressure Gradients, and Resistance F = ∆P/R F = flow ∆P = difference in
- 65. 23.5d Airflow, Pressure Gradients, and Resistance Pressure gradient Can be changed by altering volume of thoracic
- 66. 23.5d Airflow, Pressure Gradients, and Resistance Resistance (continued) Decreases in chest wall elasticity increase resistance Chest
- 67. 23.5d Airflow, Pressure Gradients, and Resistance Resistance (continued) Collapsed alveoli increase resistance Can occur if alveolar
- 68. 23.5d Airflow, Pressure Gradients, and Resistance Several conditions can increase resistance to airflow Decreases in size
- 69. 23.5e Pulmonary and Alveolar Ventilation Pulmonary ventilation Process of moving air into and out of the
- 70. 23.5e Pulmonary and Alveolar Ventilation Anatomic dead space: conducting zone space No exchange of respiratory gases
- 71. 23.5e Pulmonary and Alveolar Ventilation Physiologic dead space Normal anatomic dead space + any loss of
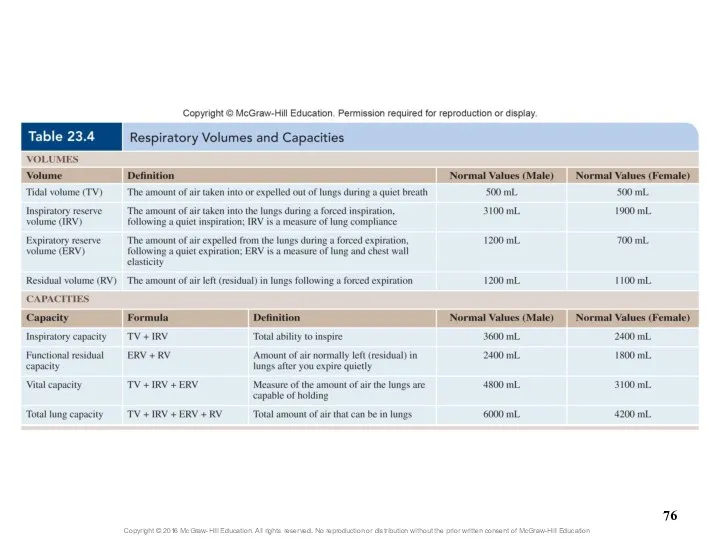
- 72. 23.5f Volume and Capacity Spirometer measures respiratory volume Can be used to assess respiratory health Standard
- 73. 23.5f Volume and Capacity Four capacities calculated from respiratory volumes Inspiratory capacity (IC) Tidal volume +
- 74. 23.5f Volume and Capacity Additional respiratory measurements—rates of air movement Forced expiratory volume (FEV) Percent of
- 75. Respiratory Volumes and Capacities Figure 23.24
- 77. What did you learn? What is Boyle’s law and how does it relate to respiration? Which
- 78. 23.6 Respiration: Alveolar and Systemic Gas Exchange Define partial pressure and the movement of gases relative
- 79. 23.6 Respiration: Alveolar and Systemic Gas Exchange (continued) Name the two anatomic features of the respiratory
- 80. 23.6a Chemical Principles of Gas Exchange Partial pressure and Dalton’s law Partial pressure: pressure exerted by
- 81. 23.6a Chemical Principles of Gas Exchange Partial pressure and Dalton’s law (continued) Total pressure × %
- 82. 23.6a Chemical Principles of Gas Exchange Partial pressure gradients Gradient exists when partial pressure for a
- 83. 23.6a Chemical Principles of Gas Exchange Relevant partial pressures in the body Reasons partial pressures in
- 84. 23.6a Chemical Principles of Gas Exchange Relevant partial pressures in the body (continued) In systemic cells,
- 85. Figure 23.25 Alveolar and Systemic Gas Exchange
- 86. 23.6a Chemical Principles of Gas Exchange Gas solubility and Henry’s law Henry’s law: at a given
- 87. 23.6a Chemical Principles of Gas Exchange Gas solubility and Henry’s law (continued) Gases vary in their
- 88. Clinical View: Decompression Sickness and Hyperbaric Oxygen Chambers Decompression sickness (the bends) Occurs when a diver
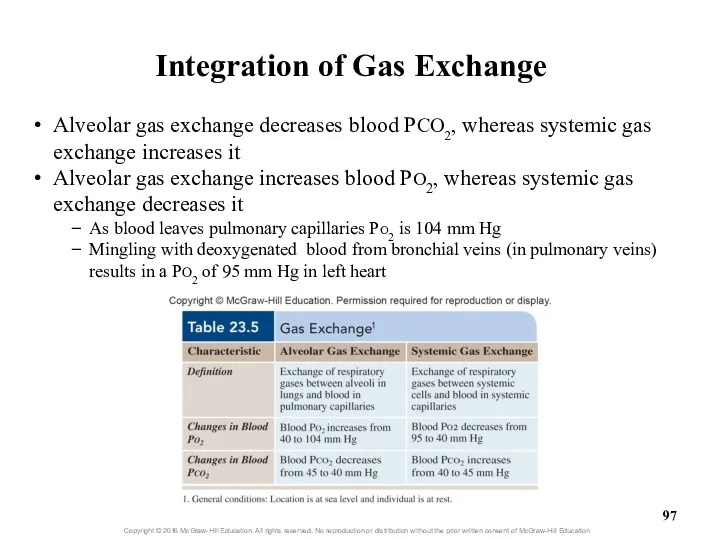
- 89. 23.6b Alveolar Gas Exchange (External Respiration) Oxygen PO2 in alveoli is 104 mm Hg PO2 of
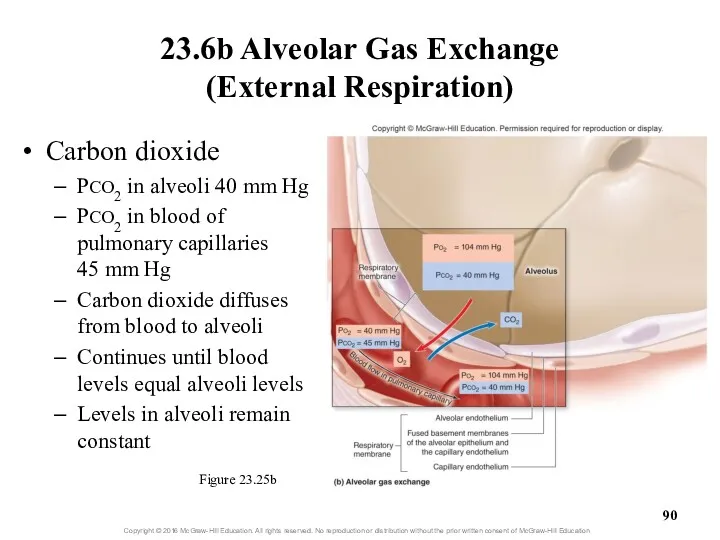
- 90. 23.6b Alveolar Gas Exchange (External Respiration) Figure 23.25b Carbon dioxide PCO2 in alveoli 40 mm Hg
- 91. Clinical View: Emphysema Emphysema causes Irreversible loss of pulmonary gas exchange surface area Inflammation of air
- 92. 23.6b Alveolar Gas Exchange (External Respiration) Efficiency of gas exchange at respiratory membrane Anatomical features of
- 93. Ventilation-Perfusion Coupling Figure 23.26
- 94. Clinical View: Respiratory Diseases and Efficiency of Alveolar Gas Exchange Certain diseases decrease the efficiency of
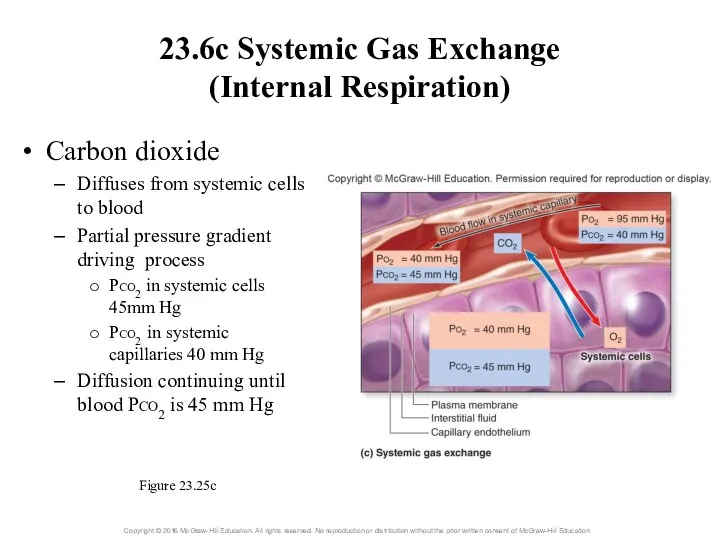
- 95. 23.6c Systemic Gas Exchange (Internal Respiration) Oxygen diffuses out of systemic capillaries to enter systemic cells
- 96. 23.6c Systemic Gas Exchange (Internal Respiration) Carbon dioxide Diffuses from systemic cells to blood Partial pressure
- 97. Alveolar gas exchange decreases blood PCO2, whereas systemic gas exchange increases it Alveolar gas exchange increases
- 98. What did you learn? What is a partial pressure? How does Henry’s law relate to human
- 99. 23.7 Respiration: Gas Transport Explain why hemoglobin is essential to oxygen transport. Describe the three ways
- 100. 23.7a Oxygen Transport Blood’s ability to transport oxygen depends on Solubility coefficient of oxygen This is
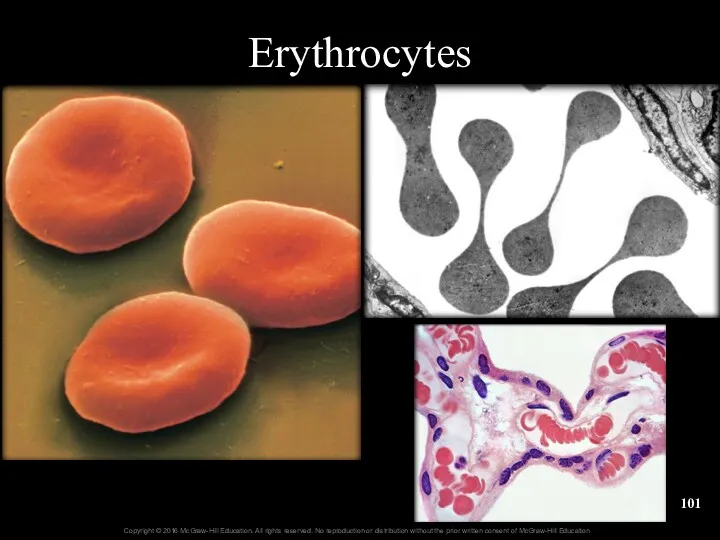
- 101. Erythrocytes
- 102. Clinical View: Measuring Blood Oxygen Levels with a Pulse Oximeter Noninvasive and indirect way to measure
- 103. 23.7b Carbon Dioxide Transport Carbon dioxide has three means of transport As CO2 dissolved in plasma
- 104. Conversion of CO2 to Bicarbonate (Figure 23.27)
- 105. 23.7c Hemoglobin as a Transport Molecule Hemoglobin transports Oxygen attached to iron Carbon dioxide bound to
- 106. 23.7c Hemoglobin as a Transport Molecule Oxygen-hemoglobin saturation curve Each hemoglobin can bind up to four
- 107. Oxygen-Hemoglobin Saturation Curve Figure 23.28
- 108. 23.7c Hemoglobin as a Transport Molecule Oxygen-hemoglobin saturation curve (continued) Large changes in saturation occur with
- 109. 23.7c Hemoglobin as a Transport Molecule Oxygen-hemoglobin saturation curve (continued) Can use graph to determine saturation
- 110. 23.7c Hemoglobin as a Transport Molecule Oxygen-hemoglobin saturation curve (continued) Some (not all) oxygen released from
- 111. 23.7c Hemoglobin as a Transport Molecule Other variables that influence oxygen release from hemoglobin during systemic
- 112. 23.7c Hemoglobin as a Transport Molecule Other variables that influence oxygen release from hemoglobin during systemic
- 113. 23.7c Hemoglobin as a Transport Molecule Other variables that influence oxygen release from hemoglobin during systemic
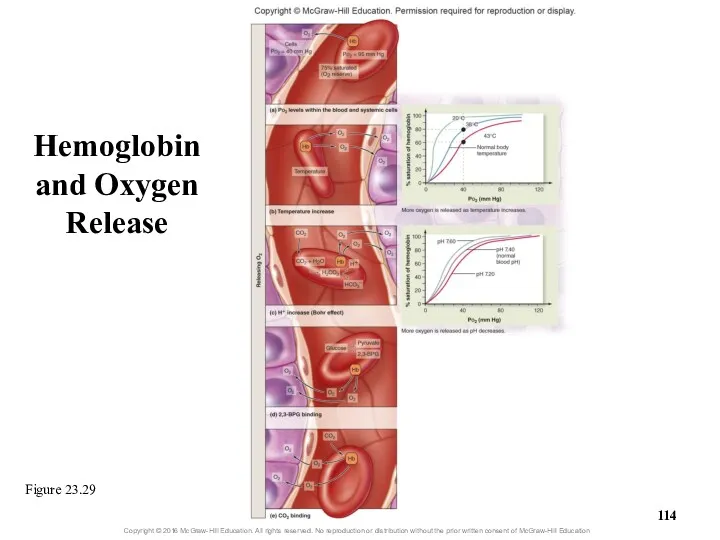
- 114. Hemoglobin and Oxygen Release Figure 23.29
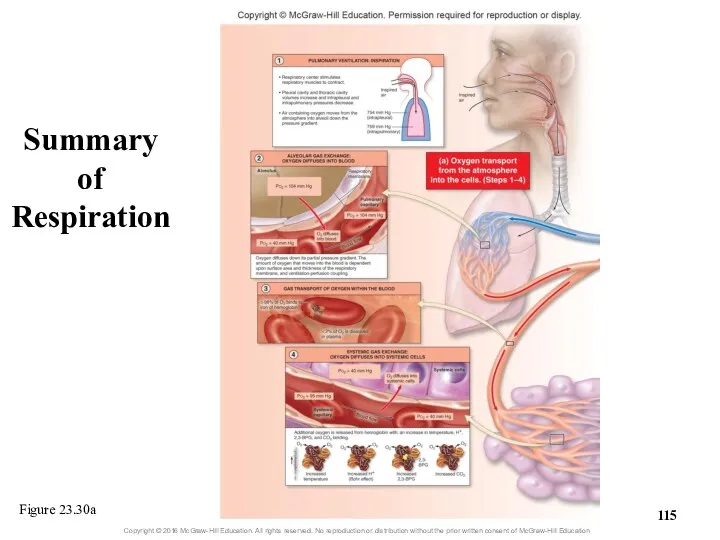
- 115. Summary of Respiration Figure 23.30a
- 116. Figure 23.30b Summary of Respiration
- 117. Clinical View: Fetal Hemoglobin and Physiologic Jaundice Unborn babies have a different type of hemoglobin molecule
- 118. What did you learn? Why is so little O2 dissolved in plasma? How is most CO2
- 119. 23.8 Breathing Rate and Homeostasis Explain how hyperventilation and hypoventilation influence the chemical composition of blood.
- 120. 23.8a Effects of Hyperventilation and Hypoventilation on Cardiovascular Function Hyperventilation: breathing rate or depth above body’s
- 121. 23.8a Effects of Hyperventilation and Hypoventilation on Cardiovascular Function Hyperventilation (continued) Low blood CO2 causes vasoconstriction
- 122. 23.8a Effects of Hyperventilation and Hypoventilation on Cardiovascular Function Hypoventilation: breathing too slow (bradypnea) or too
- 123. 23.8a Effects of Hyperventilation and Hypoventilation on Cardiovascular Function Hypoventilation (continued) May result in inadequate oxygen
- 124. 23.8b Breathing and Exercise While exercising, breathing shows hyperpnea to meet increased tissue needs Breathing depth
- 126. Скачать презентацию
Processes of Respiration
Respiration (exchange of gases between atmosphere and body’s cells)
Processes of Respiration
Respiration (exchange of gases between atmosphere and body’s cells)
Processes of Respiration
Net movement of respiratory gases
Air containing O2 is inhaled
Processes of Respiration
Net movement of respiratory gases
Air containing O2 is inhaled
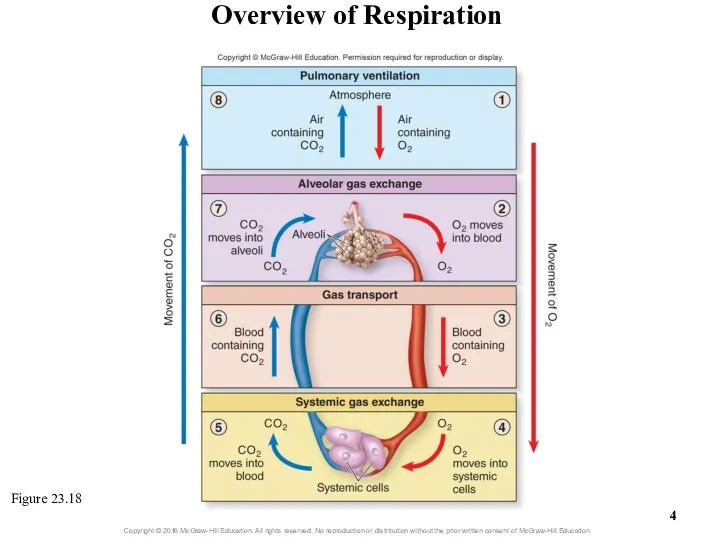
Overview of Respiration
Figure 23.18
Overview of Respiration
Figure 23.18
23.5
Respiration: Pulmonary Ventilation
Give an overview of the process of pulmonary
23.5
Respiration: Pulmonary Ventilation
Give an overview of the process of pulmonary
23.5
Respiration: Pulmonary Ventilation (continued)
Explain the physiologic events associated with controlling
23.5
Respiration: Pulmonary Ventilation (continued)
Explain the physiologic events associated with controlling
23.5
Respiration: Pulmonary Ventilation (continued)
Distinguish between pulmonary ventilation and alveolar ventilation,
23.5
Respiration: Pulmonary Ventilation (continued)
Distinguish between pulmonary ventilation and alveolar ventilation,
23.5a Introduction to Pulmonary Ventilation
Pulmonary ventilation (breathing): air movement
Consists of two
23.5a Introduction to Pulmonary Ventilation
Pulmonary ventilation (breathing): air movement
Consists of two
23.5b Mechanics of Breathing
Involve several integrated aspects
Specific actions of skeletal muscles
23.5b Mechanics of Breathing
Involve several integrated aspects
Specific actions of skeletal muscles
23.5b Mechanics of Breathing
Skeletal muscles of breathing
Muscles of quiet breathing
Diaphragm and
23.5b Mechanics of Breathing
Skeletal muscles of breathing
Muscles of quiet breathing
Diaphragm and
Diaphragm
Diaphragm
Diaphragm
Diaphragm
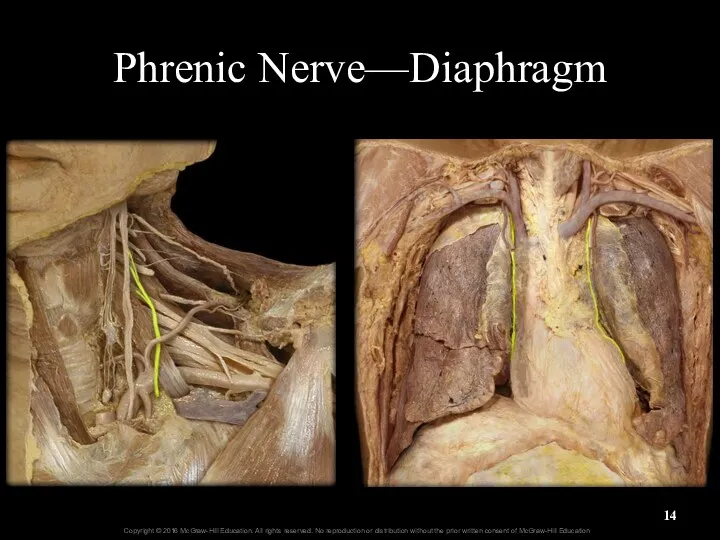
Phrenic Nerve—Diaphragm
Phrenic Nerve—Diaphragm
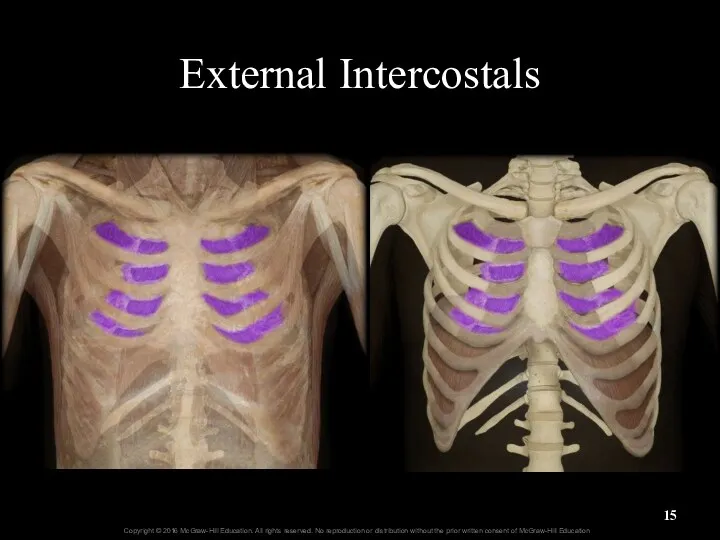
External Intercostals
External Intercostals
External Intercostals
Origins
Insertions
External Intercostals
Origins
Insertions
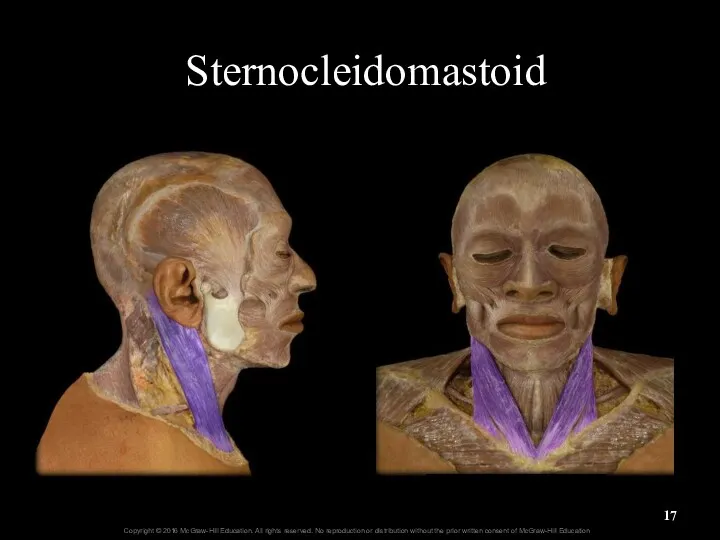
Sternocleidomastoid
Sternocleidomastoid
Sternocleidomastoid
origin
insertion
Sternocleidomastoid
origin
insertion
Scalenes
22-
Scalenes
22-
Pectoralis Minor
Pectoralis Minor
Pectoralis Minor
Insertion
Origins
Pectoralis Minor
Insertion
Origins

Serratus Posterior Superior
serrate = scalloped or zigzag
Serratus Posterior Superior
serrate = scalloped or zigzag
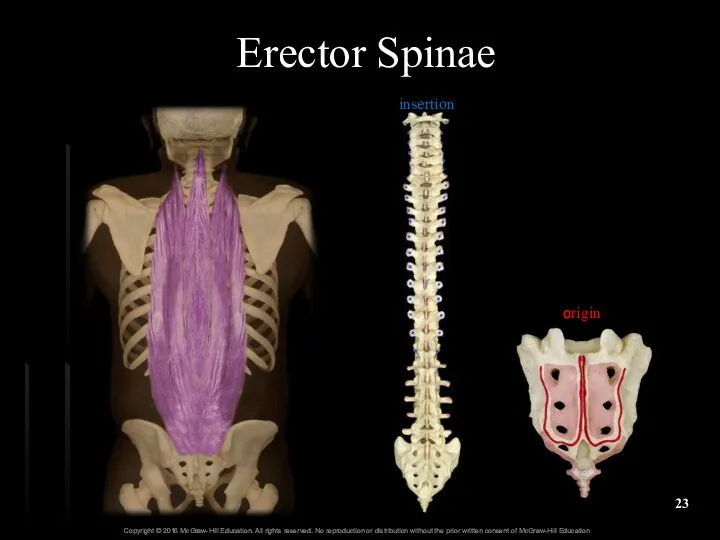
Erector Spinae
origin
insertion
Erector Spinae
origin
insertion
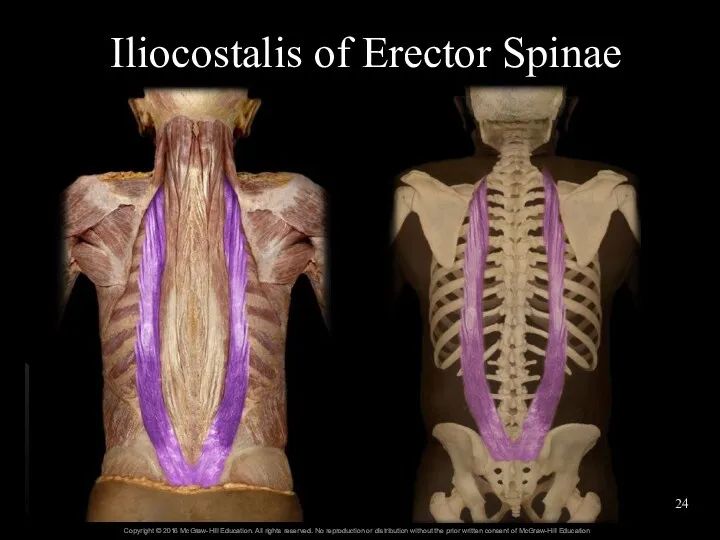
Iliocostalis of Erector Spinae
Iliocostalis of Erector Spinae

Longissimus of Erector Spinae
origin
insertion
Longissimus of Erector Spinae
origin
insertion
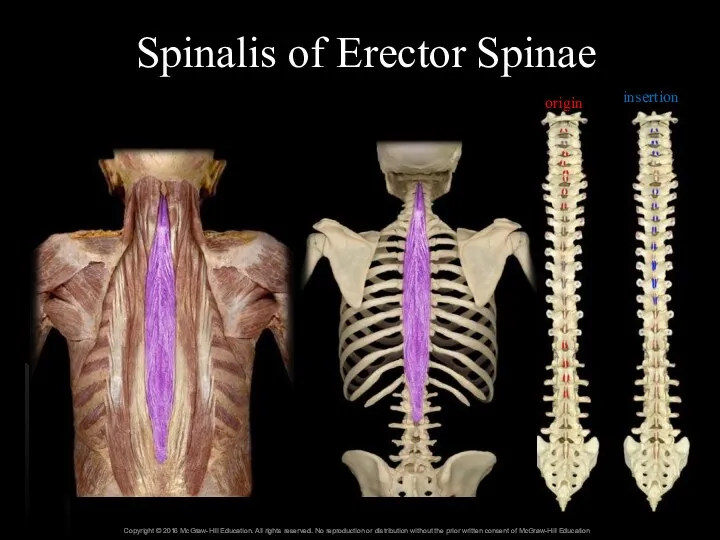
Spinalis of Erector Spinae
origin
insertion
Spinalis of Erector Spinae
origin
insertion
23.5b Mechanics of Breathing
Skeletal muscles of breathing (continued)
Muscles of forced expiration
Include
23.5b Mechanics of Breathing
Skeletal muscles of breathing (continued)
Muscles of forced expiration
Include
Internal Intercostals
Internal Intercostals
Lateral Abdominal Muscles
External Abdominal Oblique
Internal Abdominal Oblique
Transverse Abdominis
Lateral Abdominal Muscles
External Abdominal Oblique
Internal Abdominal Oblique
Transverse Abdominis
Internal Abdominal Oblique and
Transversus Abdominis
Internal Abdominal Oblique and
Transversus Abdominis
Rectus Abdominis
Tendinous intersections
Linea alba
Insertions
Rectus Abdominis
Tendinous intersections
Linea alba
Insertions
Rectus Abdominis
Rectus Abdominis
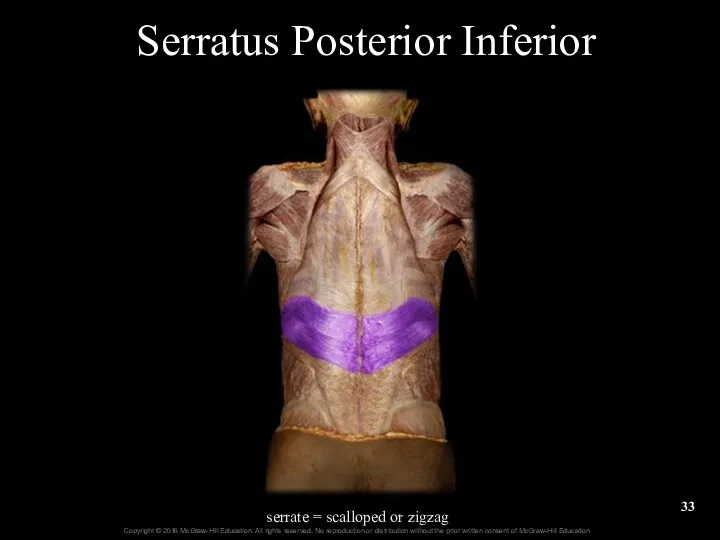
Serratus Posterior Inferior
serrate = scalloped or zigzag
Serratus Posterior Inferior
serrate = scalloped or zigzag
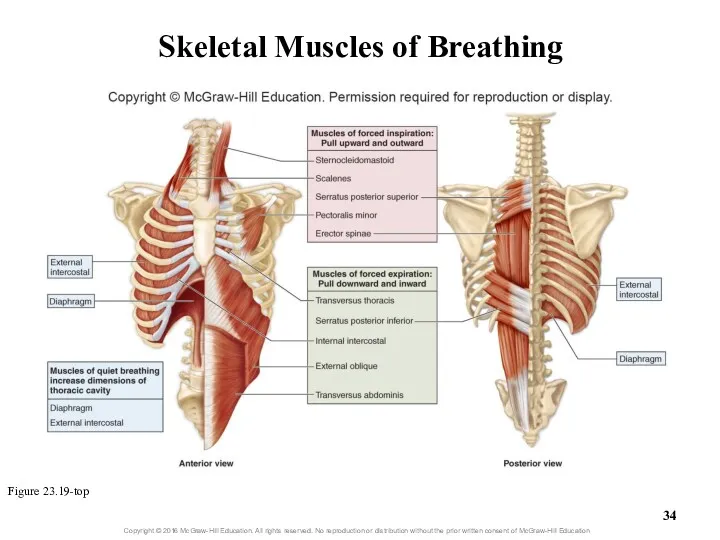
Skeletal Muscles of Breathing
Figure 23.19-top
Skeletal Muscles of Breathing
Figure 23.19-top
23.5b Mechanics of Breathing
Volume changes in the thoracic cavity
Thoracic volume changes
23.5b Mechanics of Breathing
Volume changes in the thoracic cavity
Thoracic volume changes
Thoracic Cavity Dimensional Changes Associated with Breathing
Figure 23.20
Thoracic Cavity Dimensional Changes Associated with Breathing
Figure 23.20
23.5b Mechanics of Breathing
Volume changes in the thoracic cavity (continued)
Lateral dimension
23.5b Mechanics of Breathing
Volume changes in the thoracic cavity (continued)
Lateral dimension
Boyle’s gas law: Relationship of volume and pressure
At constant temperature, pressure
Boyle’s gas law: Relationship of volume and pressure
At constant temperature, pressure
23.5b Mechanics of Breathing
An air pressure gradient exists when force per
23.5b Mechanics of Breathing
An air pressure gradient exists when force per
23.5b Mechanics of Breathing
Volumes and pressures associated with breathing
Atmospheric pressure: pressure
23.5b Mechanics of Breathing
Volumes and pressures associated with breathing
Atmospheric pressure: pressure
23.5b Mechanics of Breathing
Volumes and pressures associated with breathing (cont’d.)
Intrapleural pressure:
23.5b Mechanics of Breathing
Volumes and pressures associated with breathing (cont’d.)
Intrapleural pressure:
Pressures Associated with Breathing
Figure 23.21c
Pressures Associated with Breathing
Figure 23.21c
23.5b Mechanics of Breathing
Quiet breathing: Inspiration
Intrapulmonary pressure and atmospheric pressure
23.5b Mechanics of Breathing
Quiet breathing: Inspiration
Intrapulmonary pressure and atmospheric pressure
23.5b Mechanics of Breathing
Quiet breathing: Expiration
3) Initially, intrapulmonary pressure equals
23.5b Mechanics of Breathing
Quiet breathing: Expiration
3) Initially, intrapulmonary pressure equals
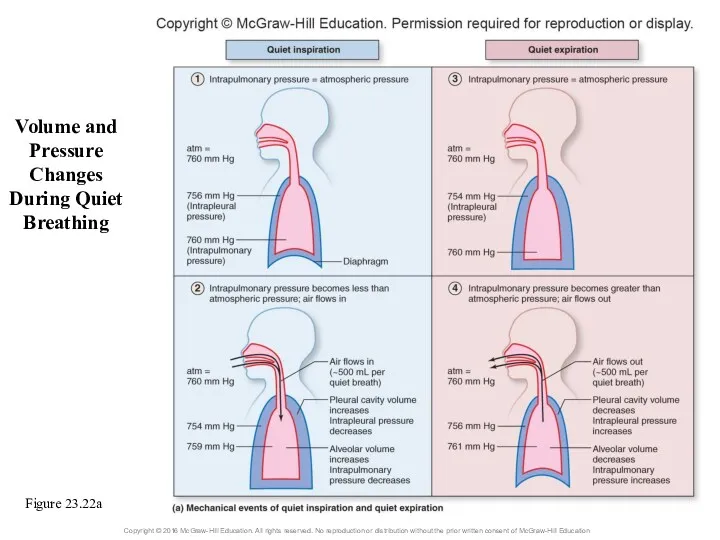
Volume and Pressure Changes During Quiet Breathing
Figure 23.22a
Volume and Pressure Changes During Quiet Breathing
Figure 23.22a
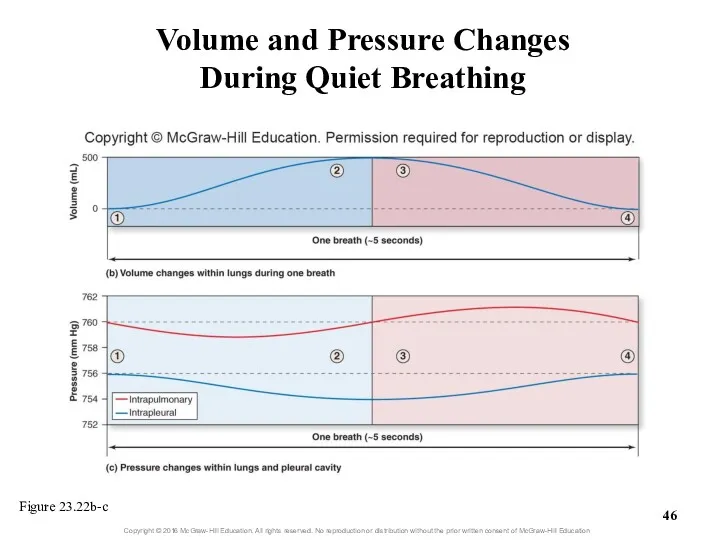
Volume and Pressure Changes
During Quiet Breathing
Figure 23.22b-c
Volume and Pressure Changes
During Quiet Breathing
Figure 23.22b-c
23.5b Mechanics of Breathing
Forced breathing
Involves steps similar to quiet breathing
Requires contraction
23.5b Mechanics of Breathing
Forced breathing
Involves steps similar to quiet breathing
Requires contraction
23.5c Nervous Control of Breathing
Autonomic nuclei within the brain coordinate breathing
Respiratory
23.5c Nervous Control of Breathing
Autonomic nuclei within the brain coordinate breathing
Respiratory
Neural Control of Breathing
Medulla
oblongata
Pons
Neural Control of Breathing
Medulla
oblongata
Pons
23.5c Nervous Control of Breathing
Chemoreceptors monitor changes in concentrations of H+,
23.5c Nervous Control of Breathing
Chemoreceptors monitor changes in concentrations of H+,
23.5c Nervous Control of Breathing
Other receptors also influence respiration
Proprioceptors of muscles
23.5c Nervous Control of Breathing
Other receptors also influence respiration
Proprioceptors of muscles
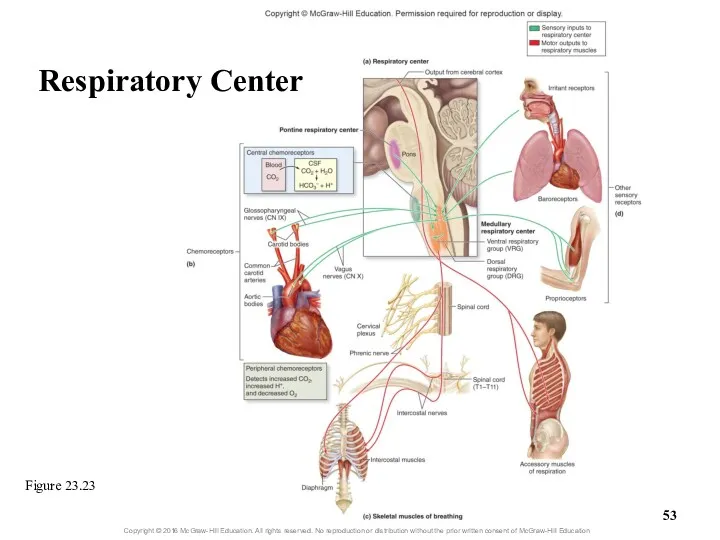
Figure 23.23
Respiratory Center
Figure 23.23
Respiratory Center
23.5c Nervous Control of Breathing
Physiology of quiet breathing
Inspiration begins when VRG
23.5c Nervous Control of Breathing
Physiology of quiet breathing
Inspiration begins when VRG
23.5c Nervous Control of Breathing
Physiology of quiet breathing (continued)
Respiration rate for
23.5c Nervous Control of Breathing
Physiology of quiet breathing (continued)
Respiration rate for
Clinical View: Apnea
Apnea = absence of breathing
Can occur voluntarily
Swallowing
Clinical View: Apnea
Apnea = absence of breathing
Can occur voluntarily
Swallowing
23.5c Nervous Control of Breathing
Reflexes that alter breathing rate and depth
Chemoreceptors
23.5c Nervous Control of Breathing
Reflexes that alter breathing rate and depth
Chemoreceptors
23.5c Nervous Control of Breathing
Reflexes that alter breathing rate and depth
23.5c Nervous Control of Breathing
Reflexes that alter breathing rate and depth
Clinical View: Hypoxic Drive
Normally the most important stimulus affecting breathing rate
Clinical View: Hypoxic Drive
Normally the most important stimulus affecting breathing rate
23.5c Nervous Control of Breathing
Reflexes that alter breathing rate and depth
23.5c Nervous Control of Breathing
Reflexes that alter breathing rate and depth
23.5c Nervous Control of Breathing
Reflexes that alter breathing rate and depth
23.5c Nervous Control of Breathing
Reflexes that alter breathing rate and depth
23.5c Nervous Control of Breathing
Nervous control of respiratory system structures and
23.5c Nervous Control of Breathing
Nervous control of respiratory system structures and
23.5d Airflow, Pressure Gradients,
and Resistance
Airflow: amount of air moving in and
23.5d Airflow, Pressure Gradients,
and Resistance
Airflow: amount of air moving in and
23.5d Airflow, Pressure Gradients,
and Resistance
F = ∆P/R
F = flow
∆P =
23.5d Airflow, Pressure Gradients,
and Resistance
F = ∆P/R
F = flow
∆P =
23.5d Airflow, Pressure Gradients,
and Resistance
Pressure gradient
Can be changed by altering
23.5d Airflow, Pressure Gradients,
and Resistance
Pressure gradient
Can be changed by altering
23.5d Airflow, Pressure Gradients,
and Resistance
Resistance (continued)
Decreases in chest wall elasticity increase
23.5d Airflow, Pressure Gradients,
and Resistance
Resistance (continued)
Decreases in chest wall elasticity increase
23.5d Airflow, Pressure Gradients,
and Resistance
Resistance (continued)
Collapsed alveoli increase resistance
Can occur if
23.5d Airflow, Pressure Gradients,
and Resistance
Resistance (continued)
Collapsed alveoli increase resistance
Can occur if
23.5d Airflow, Pressure Gradients,
and Resistance
Several conditions can increase resistance to airflow
Decreases
23.5d Airflow, Pressure Gradients,
and Resistance
Several conditions can increase resistance to airflow
Decreases
23.5e Pulmonary and Alveolar Ventilation
Pulmonary ventilation
Process of moving air into and
23.5e Pulmonary and Alveolar Ventilation
Pulmonary ventilation
Process of moving air into and
23.5e Pulmonary and Alveolar Ventilation
Anatomic dead space: conducting zone space
No exchange
23.5e Pulmonary and Alveolar Ventilation
Anatomic dead space: conducting zone space
No exchange
23.5e Pulmonary and Alveolar Ventilation
Physiologic dead space
Normal anatomic dead space +
23.5e Pulmonary and Alveolar Ventilation
Physiologic dead space
Normal anatomic dead space +
23.5f Volume and Capacity
Spirometer measures respiratory volume
Can be used to assess
23.5f Volume and Capacity
Spirometer measures respiratory volume
Can be used to assess
23.5f Volume and Capacity
Four capacities calculated from respiratory volumes
Inspiratory capacity (IC)
Tidal
23.5f Volume and Capacity
Four capacities calculated from respiratory volumes
Inspiratory capacity (IC)
Tidal
23.5f Volume and Capacity
Additional respiratory measurements—rates of air movement
Forced expiratory volume
23.5f Volume and Capacity
Additional respiratory measurements—rates of air movement
Forced expiratory volume
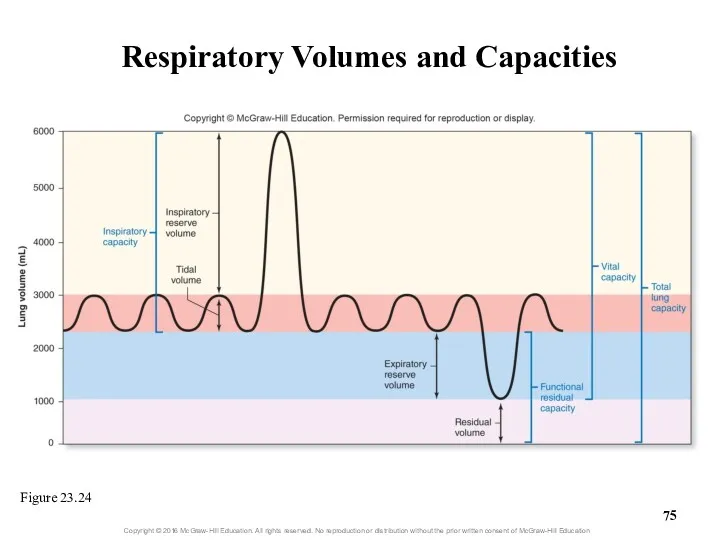
Respiratory Volumes and Capacities
Figure 23.24
Respiratory Volumes and Capacities
Figure 23.24
What did you learn?
What is Boyle’s law and how does it
What did you learn?
What is Boyle’s law and how does it
23.6
Respiration: Alveolar and Systemic Gas Exchange
Define partial pressure and the
23.6
Respiration: Alveolar and Systemic Gas Exchange
Define partial pressure and the
23.6
Respiration: Alveolar and Systemic Gas Exchange (continued)
Name the two anatomic
23.6
Respiration: Alveolar and Systemic Gas Exchange (continued)
Name the two anatomic
23.6a Chemical Principles of Gas Exchange
Partial pressure and Dalton’s law
Partial pressure:
23.6a Chemical Principles of Gas Exchange
Partial pressure and Dalton’s law
Partial pressure:
23.6a Chemical Principles of Gas Exchange
Partial pressure and Dalton’s law (continued)
Total
23.6a Chemical Principles of Gas Exchange
Partial pressure and Dalton’s law (continued)
Total
23.6a Chemical Principles of Gas Exchange
Partial pressure gradients
Gradient exists when partial
23.6a Chemical Principles of Gas Exchange
Partial pressure gradients
Gradient exists when partial
23.6a Chemical Principles of Gas Exchange
Relevant partial pressures in the body
Reasons
23.6a Chemical Principles of Gas Exchange
Relevant partial pressures in the body
Reasons
23.6a Chemical Principles of Gas Exchange
Relevant partial pressures in the body
23.6a Chemical Principles of Gas Exchange
Relevant partial pressures in the body
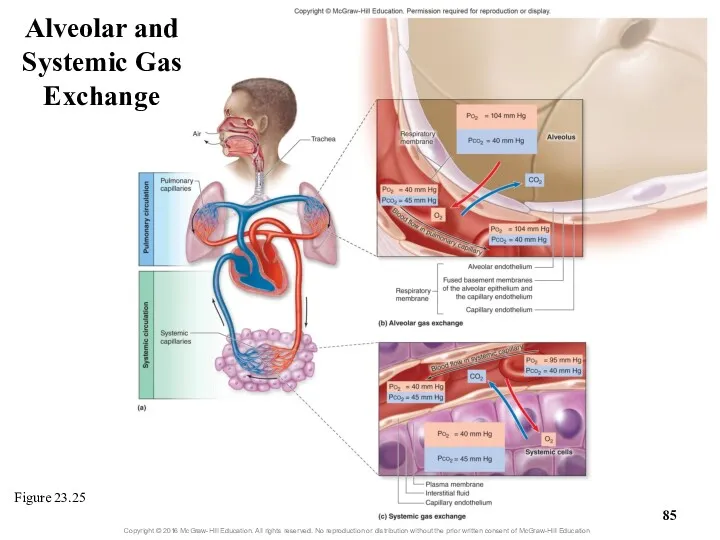
Figure 23.25
Alveolar and Systemic Gas Exchange
Figure 23.25
Alveolar and Systemic Gas Exchange
23.6a Chemical Principles of Gas Exchange
Gas solubility and Henry’s law
Henry’s law:
23.6a Chemical Principles of Gas Exchange
Gas solubility and Henry’s law
Henry’s law:
23.6a Chemical Principles of Gas Exchange
Gas solubility and Henry’s law (continued)
Gases
23.6a Chemical Principles of Gas Exchange
Gas solubility and Henry’s law (continued)
Gases
Clinical View: Decompression Sickness
and Hyperbaric Oxygen Chambers
Decompression sickness (the bends)
Occurs
Clinical View: Decompression Sickness
and Hyperbaric Oxygen Chambers
Decompression sickness (the bends)
Occurs
23.6b Alveolar Gas Exchange
(External Respiration)
Oxygen
PO2 in alveoli is 104 mm Hg
PO2
23.6b Alveolar Gas Exchange
(External Respiration)
Oxygen
PO2 in alveoli is 104 mm Hg
PO2
23.6b Alveolar Gas Exchange
(External Respiration)
Figure 23.25b
Carbon dioxide
PCO2 in alveoli 40 mm
23.6b Alveolar Gas Exchange
(External Respiration)
Figure 23.25b
Carbon dioxide
PCO2 in alveoli 40 mm
Clinical View: Emphysema
Emphysema causes
Irreversible loss of pulmonary gas exchange surface area
Inflammation
Clinical View: Emphysema
Emphysema causes
Irreversible loss of pulmonary gas exchange surface area
Inflammation
23.6b Alveolar Gas Exchange
(External Respiration)
Efficiency of gas exchange at respiratory membrane
Anatomical
23.6b Alveolar Gas Exchange
(External Respiration)
Efficiency of gas exchange at respiratory membrane
Anatomical
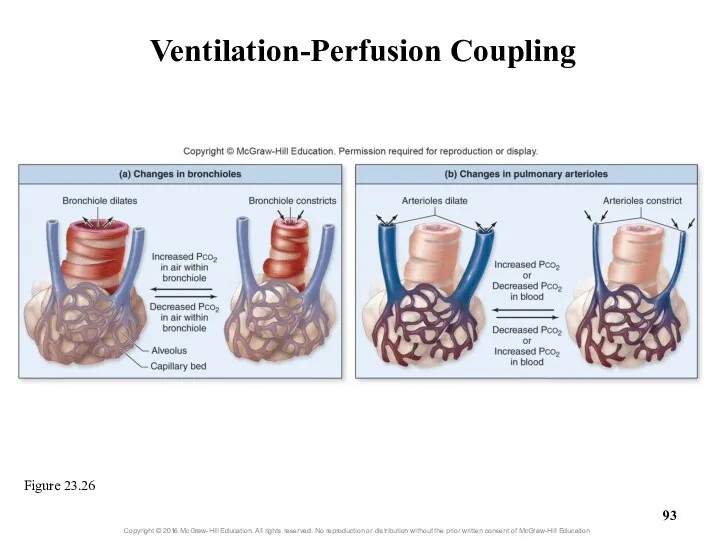
Ventilation-Perfusion Coupling
Figure 23.26
Ventilation-Perfusion Coupling
Figure 23.26
Clinical View: Respiratory Diseases and Efficiency of Alveolar Gas Exchange
Certain diseases
Clinical View: Respiratory Diseases and Efficiency of Alveolar Gas Exchange
Certain diseases
23.6c Systemic Gas Exchange
(Internal Respiration)
Oxygen diffuses out of systemic capillaries to
23.6c Systemic Gas Exchange
(Internal Respiration)
Oxygen diffuses out of systemic capillaries to
23.6c Systemic Gas Exchange
(Internal Respiration)
Carbon dioxide
Diffuses from systemic cells to blood
Partial
23.6c Systemic Gas Exchange
(Internal Respiration)
Carbon dioxide
Diffuses from systemic cells to blood
Partial
Alveolar gas exchange decreases blood PCO2, whereas systemic gas exchange increases
Alveolar gas exchange decreases blood PCO2, whereas systemic gas exchange increases
What did you learn?
What is a partial pressure?
How does Henry’s law
What did you learn?
What is a partial pressure?
How does Henry’s law
23.7
Respiration: Gas Transport
Explain why hemoglobin is essential to oxygen transport.
Describe
23.7
Respiration: Gas Transport
Explain why hemoglobin is essential to oxygen transport.
Describe
23.7a Oxygen Transport
Blood’s ability to transport oxygen depends on
Solubility coefficient
23.7a Oxygen Transport
Blood’s ability to transport oxygen depends on
Solubility coefficient
Erythrocytes
Erythrocytes
Clinical View: Measuring Blood Oxygen Levels with a Pulse Oximeter
Noninvasive and
Clinical View: Measuring Blood Oxygen Levels with a Pulse Oximeter
Noninvasive and
23.7b Carbon Dioxide Transport
Carbon dioxide has three means of transport
As CO2
23.7b Carbon Dioxide Transport
Carbon dioxide has three means of transport
As CO2
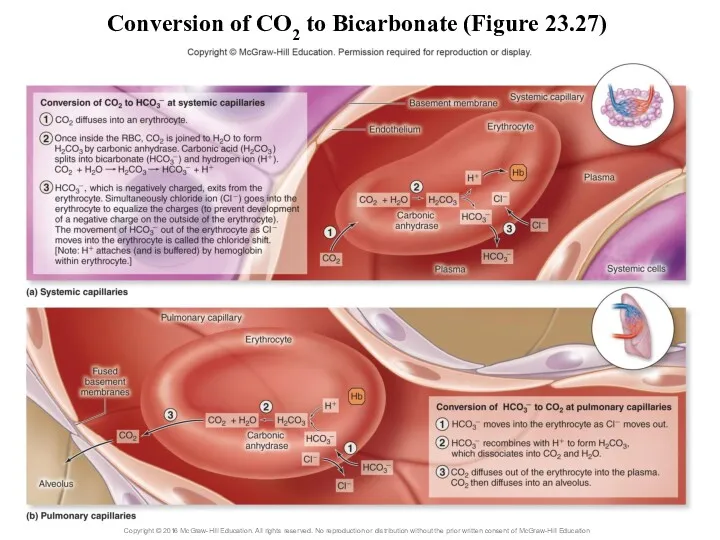
Conversion of CO2 to Bicarbonate (Figure 23.27)
Conversion of CO2 to Bicarbonate (Figure 23.27)
23.7c Hemoglobin as a Transport Molecule
Hemoglobin transports
Oxygen attached to iron
Carbon dioxide
23.7c Hemoglobin as a Transport Molecule
Hemoglobin transports
Oxygen attached to iron
Carbon dioxide
23.7c Hemoglobin as a Transport Molecule
Oxygen-hemoglobin saturation curve
Each hemoglobin can bind
23.7c Hemoglobin as a Transport Molecule
Oxygen-hemoglobin saturation curve
Each hemoglobin can bind
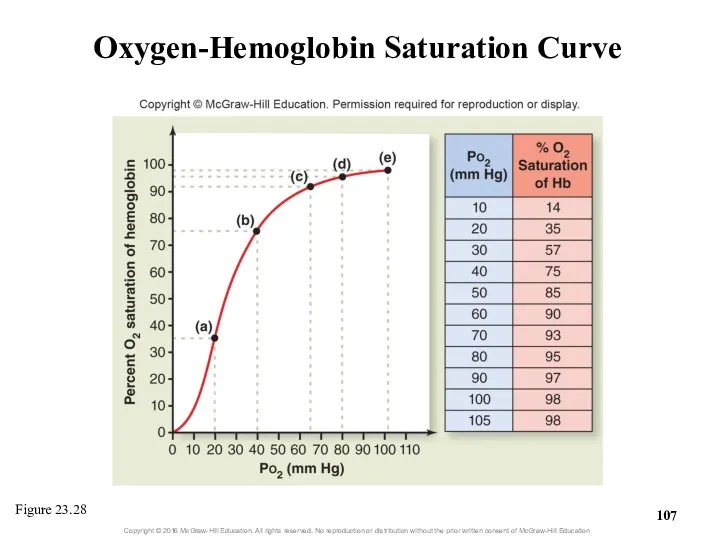
Oxygen-Hemoglobin Saturation Curve
Figure 23.28
Oxygen-Hemoglobin Saturation Curve
Figure 23.28
23.7c Hemoglobin as a Transport Molecule
Oxygen-hemoglobin saturation curve (continued)
Large changes in
23.7c Hemoglobin as a Transport Molecule
Oxygen-hemoglobin saturation curve (continued)
Large changes in
23.7c Hemoglobin as a Transport Molecule
Oxygen-hemoglobin saturation curve (continued)
Can use graph
23.7c Hemoglobin as a Transport Molecule
Oxygen-hemoglobin saturation curve (continued)
Can use graph
23.7c Hemoglobin as a Transport Molecule
Oxygen-hemoglobin saturation curve (continued)
Some (not all)
23.7c Hemoglobin as a Transport Molecule
Oxygen-hemoglobin saturation curve (continued)
Some (not all)
23.7c Hemoglobin as a Transport Molecule
Other variables that influence oxygen release
23.7c Hemoglobin as a Transport Molecule
Other variables that influence oxygen release
23.7c Hemoglobin as a Transport Molecule
Other variables that influence oxygen release
23.7c Hemoglobin as a Transport Molecule
Other variables that influence oxygen release
23.7c Hemoglobin as a Transport Molecule
Other variables that influence oxygen release
23.7c Hemoglobin as a Transport Molecule
Other variables that influence oxygen release
Hemoglobin and Oxygen Release
Figure 23.29
Hemoglobin and Oxygen Release
Figure 23.29
Summary of Respiration
Figure 23.30a
Summary of Respiration
Figure 23.30a
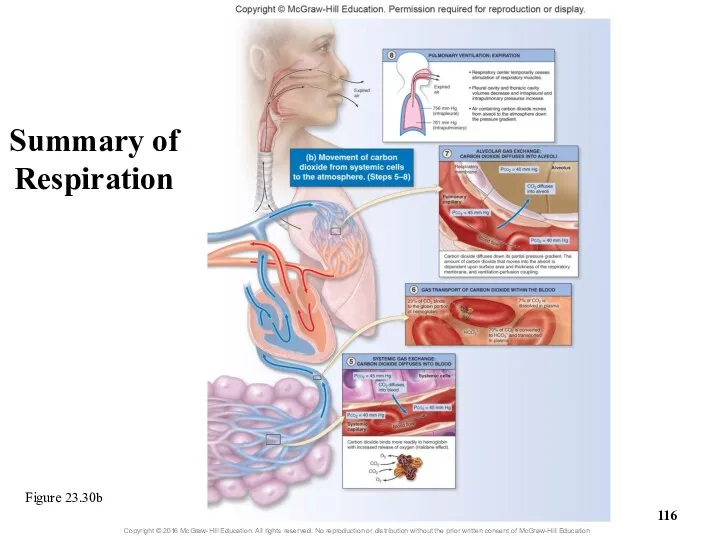
Figure 23.30b
Summary of Respiration
Figure 23.30b
Summary of Respiration
Clinical View: Fetal Hemoglobin and Physiologic Jaundice
Unborn babies have a different
Clinical View: Fetal Hemoglobin and Physiologic Jaundice
Unborn babies have a different
What did you learn?
Why is so little O2 dissolved in plasma?
How
What did you learn?
Why is so little O2 dissolved in plasma?
How
23.8
Breathing Rate and Homeostasis
Explain how hyperventilation and hypoventilation influence the
23.8
Breathing Rate and Homeostasis
Explain how hyperventilation and hypoventilation influence the
23.8a Effects of Hyperventilation and Hypoventilation on Cardiovascular Function
Hyperventilation: breathing rate
23.8a Effects of Hyperventilation and Hypoventilation on Cardiovascular Function
Hyperventilation: breathing rate
23.8a Effects of Hyperventilation and Hypoventilation on Cardiovascular Function
Hyperventilation (continued)
Low blood
23.8a Effects of Hyperventilation and Hypoventilation on Cardiovascular Function
Hyperventilation (continued)
Low blood
23.8a Effects of Hyperventilation and Hypoventilation on Cardiovascular Function
Hypoventilation: breathing too
23.8a Effects of Hyperventilation and Hypoventilation on Cardiovascular Function
Hypoventilation: breathing too
23.8a Effects of Hyperventilation and Hypoventilation on Cardiovascular Function
Hypoventilation (continued)
May result
23.8a Effects of Hyperventilation and Hypoventilation on Cardiovascular Function
Hypoventilation (continued)
May result
23.8b Breathing and Exercise
While exercising, breathing shows hyperpnea to meet increased
23.8b Breathing and Exercise
While exercising, breathing shows hyperpnea to meet increased
 Разнообразие растительного мира на Земле
Разнообразие растительного мира на Земле Животные семейства кошачьих (фотографии)
Животные семейства кошачьих (фотографии) Генетика. Наследственность
Генетика. Наследственность Строение и функции кожи. 8 класс
Строение и функции кожи. 8 класс Происхождение и эволюция человека
Происхождение и эволюция человека Высшая нервная деятельность человека
Высшая нервная деятельность человека Основы разведения животных
Основы разведения животных Структурная и экологическая морфология растений. Часть 1
Структурная и экологическая морфология растений. Часть 1 Адаптация человека к различным природным условиям
Адаптация человека к различным природным условиям Пленки Лэнгмюра - Блоджетт
Пленки Лэнгмюра - Блоджетт Физико-химические основы патологии клетки. Митохондрии и апоптоз
Физико-химические основы патологии клетки. Митохондрии и апоптоз Классификация и строение микроорганизмов. Микробиология
Классификация и строение микроорганизмов. Микробиология Дыхание, его значение. Строение и функции органов дыхания
Дыхание, его значение. Строение и функции органов дыхания Определение содержания аскорбиновой кислоты (витамина С) в различных сортах яблок
Определение содержания аскорбиновой кислоты (витамина С) в различных сортах яблок Сучасні критерії виду
Сучасні критерії виду Биофизика. Первый закон термодинамики для живых систем. Закон Гесса
Биофизика. Первый закон термодинамики для живых систем. Закон Гесса Отдел папоротниковидные. Подотдел папоротники
Отдел папоротниковидные. Подотдел папоротники Класс пресмыкающиеся или рептилии. Отряд чешуйчатые
Класс пресмыкающиеся или рептилии. Отряд чешуйчатые Генетика микроорганизмов. Изменчивость в микробных популяциях
Генетика микроорганизмов. Изменчивость в микробных популяциях Белый медведь
Белый медведь Адаптации жирафа к среде обитания
Адаптации жирафа к среде обитания Бактериофаги (или просто фаги) – вирусы бактерий
Бактериофаги (или просто фаги) – вирусы бактерий Нуклеиновые кислоты. ДНК и РНК
Нуклеиновые кислоты. ДНК и РНК Слюнные железы
Слюнные железы Ткани растений
Ткани растений презентации к циклу уроков по природоведению в 5 классе Кто чем питается по программе Природа.Введение в биологию и экологию Т.С. Сухова, В.И. Строганов
презентации к циклу уроков по природоведению в 5 классе Кто чем питается по программе Природа.Введение в биологию и экологию Т.С. Сухова, В.И. Строганов Перенос дыхательных газов кровью
Перенос дыхательных газов кровью Тип Моллюски. Общая характеристика
Тип Моллюски. Общая характеристика