- Algoritm of differencial diagnosis of Neonatal. Jaundice

Содержание
- 2. Neonatal Jaundice
- 3. Teaching Aids: NNF Neonatal Jaundice Visible form of bilirubinemia Adult sclera >2mg / dl Newborn skin
- 4. Teaching Aids: NNF What is the Neonatal Jaundice? Neonatal Jaundice(also called Newborn jaundice) is a condition
- 5. Teaching Aids: NNF Causes of Jaundice according to time of appearance 1.Appearing at birth or within
- 6. Teaching Aids: NNF 2.Appearing between 24-72 hours of life Physiological Sepsis neonatorum Plycythemia Concealed hemorrhages:cephalhematoma,subarachnoid bleed,IVN.
- 7. Teaching Aids: NNF 3.Appearing after 72 hrs and within 1st week Sepsis Syphilis Toxoplasmosis 4.Jaundice apearing
- 8. Teaching Aids: NNF Special characteristic in neonates 1)More billirubin produced Much more hemolysis The life-length of
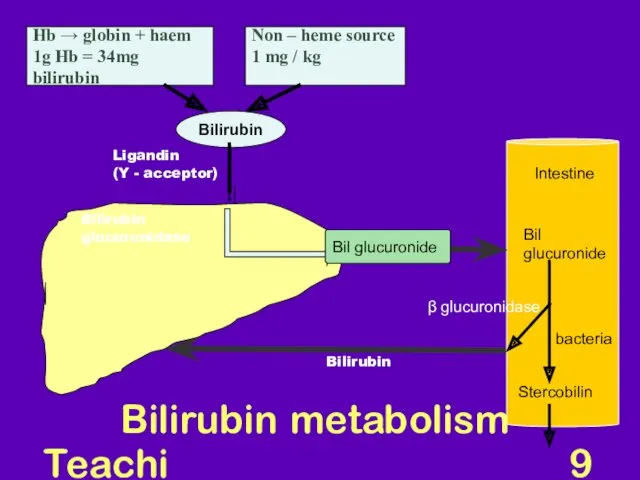
- 9. Teaching Aids: NNF Bilirubin metabolism Hb → globin + haem 1g Hb = 34mg bilirubin Non
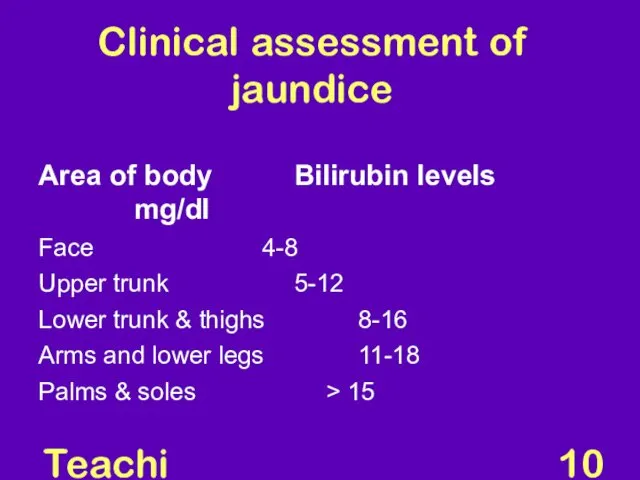
- 10. Teaching Aids: NNF Clinical assessment of jaundice Area of body Bilirubin levels mg/dl Face 4-8 Upper
- 11. Teaching Aids: NNF Physiological jaundice Characteristics Appears after 24 hours Maximum intensity by 4th-5th day in
- 12. Teaching Aids: NNF Why does physiological jaundice develop? Increased bilirubin load Defective uptake from plasma Defective
- 13. Course of physiological jaundice
- 14. Teaching Aids: NNF Pathological jaundice Appears within 24 hours of age Increase of bilirubin > 5
- 15. Teaching Aids: NNF Causes of jaundice Appearing within 24 hours of age Hemolytic disease of NB
- 16. Teaching Aids: NNF Causes of jaundice After 72 hours of age Sepsis Cephalhaematoma Neonatal hepatitis Extra-hepatic
- 17. Teaching Aids: NNF The general symptoms of Neonatal Jaundice Yellow skin Yellow eyes(sclera) Sleepiness Poor feeding
- 18. Teaching Aids: NNF Risk factors for jaundice JAUNDICE J - jaundice within first 24 hrs of
- 19. Teaching Aids: NNF Common causes Physiological Blood group incompatibility G6PD deficiency Bruising and cephalhaematoma Intrauterine and
- 20. Teaching Aids: NNF Approach to jaundiced baby Ascertain birth weight, gestation and postnatal age Assess clinical
- 21. Teaching Aids: NNF Workup Maternal & perinatal history Physical examination Laboratory tests (must in all)* Total
- 22. Teaching Aids: NNF Management Rationale: reduce level of serum bilirubin and prevent bilirubin toxicity Prevention of
- 23. Teaching Aids: NNF Principle of phototherapy Native bilirubin Photo isomers of bilirubin Insoluble Soluble 450-460nm of
- 24. Teaching Aids: NNF Phototherapy equipment White light tubes 6-8*/ 4 blue light tubes Cradle or incubator
- 25. Babies under phototherapy Baby under conventional phototherapy Baby under triple unit intense phototherapy
- 26. Teaching Aids: NNF Phototherapy Technique Perform hand wash Place baby naked in cradle or incubator Fix
- 27. Teaching Aids: NNF Phototherapy Frequent extra breast feeding every 2 hourly Turn baby after each feed
- 28. Teaching Aids: NNF Diffential Diagnoses Breast Milk Jaundice Cholestatis Dubin-Johnson Syndrome GalactoseMIA Hemolytic Disease of Newborn
- 29. Teaching Aids: NNF Side effects of phototherapy Increased insensible water loss Loose stools Skin rash Bronze
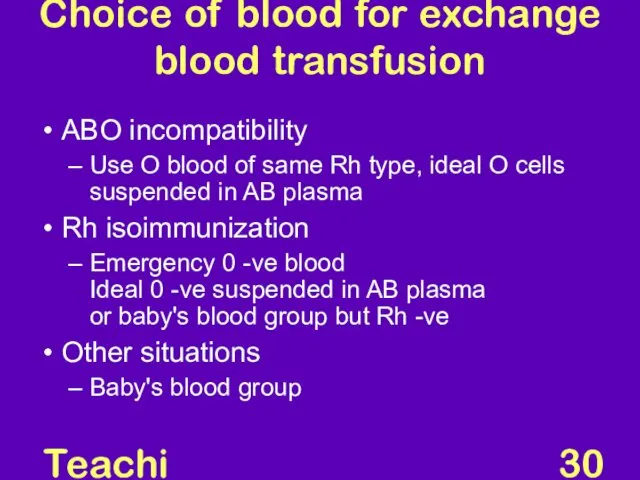
- 30. Teaching Aids: NNF Choice of blood for exchange blood transfusion ABO incompatibility Use O blood of
- 31. Maisel’s chart
- 32. Teaching Aids: NNF Prolonged indirect jaundice Causes Crigler Najjar syndrome Breast milk jaundice Hypothyroidism Pyloric stenosis
- 33. Teaching Aids: NNF Conjugated hyperbilirubinemia Suspect High colored urine White or clay colored stool Caution Always
- 34. Teaching Aids: NNF Conjugated hyperbilirubinemia Causes Idiopathic neonatal hepatitis Infections -Hepatitis B, TORCH, sepsis Biliary atresia,
- 36. Скачать презентацию

Neonatal Jaundice
Neonatal Jaundice
Teaching Aids: NNF
Neonatal Jaundice
Visible form of bilirubinemia
Adult sclera >2mg /
Teaching Aids: NNF
Neonatal Jaundice
Visible form of bilirubinemia
Adult sclera >2mg /
Teaching Aids: NNF
What is the Neonatal Jaundice?
Neonatal Jaundice(also called Newborn jaundice)
Teaching Aids: NNF
What is the Neonatal Jaundice?
Neonatal Jaundice(also called Newborn jaundice)
Teaching Aids: NNF
Causes of Jaundice according to time of appearance
1.Appearing at
Teaching Aids: NNF
Causes of Jaundice according to time of appearance
1.Appearing at
Teaching Aids: NNF
2.Appearing between 24-72 hours of life
Physiological
Sepsis neonatorum
Teaching Aids: NNF
2.Appearing between 24-72 hours of life
Physiological
Sepsis neonatorum
Teaching Aids: NNF
3.Appearing after 72 hrs and within 1st week
Sepsis
Syphilis
Teaching Aids: NNF
3.Appearing after 72 hrs and within 1st week
Sepsis
Syphilis
Teaching Aids: NNF
Special characteristic in neonates
1)More billirubin produced
Much more hemolysis
Teaching Aids: NNF
Special characteristic in neonates
1)More billirubin produced
Much more hemolysis
Teaching Aids: NNF
Bilirubin metabolism
Hb → globin + haem
1g Hb = 34mg
Teaching Aids: NNF
Bilirubin metabolism
Hb → globin + haem
1g Hb = 34mg
Teaching Aids: NNF
Clinical assessment of jaundice
Area of body Bilirubin levels mg/dl
Face 4-8
Upper
Teaching Aids: NNF
Clinical assessment of jaundice
Area of body Bilirubin levels mg/dl
Face 4-8
Upper
Teaching Aids: NNF
Physiological jaundice
Characteristics
Appears after 24 hours
Maximum intensity by 4th-5th day
Teaching Aids: NNF
Physiological jaundice
Characteristics
Appears after 24 hours
Maximum intensity by 4th-5th day
Teaching Aids: NNF
Why does physiological jaundice develop?
Increased bilirubin load
Defective uptake from
Teaching Aids: NNF
Why does physiological jaundice develop?
Increased bilirubin load
Defective uptake from
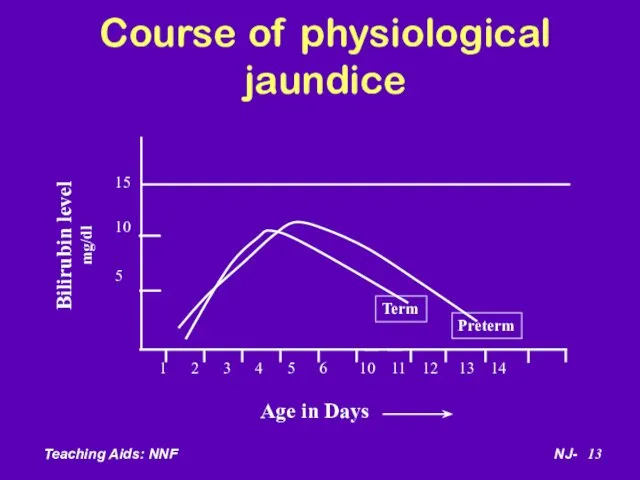
Course of physiological jaundice
Course of physiological jaundice
Teaching Aids: NNF
Pathological jaundice
Appears within 24 hours of age
Increase of bilirubin
Teaching Aids: NNF
Pathological jaundice
Appears within 24 hours of age
Increase of bilirubin
Teaching Aids: NNF
Causes of jaundice
Appearing within 24 hours of age
Hemolytic disease
Teaching Aids: NNF
Causes of jaundice
Appearing within 24 hours of age
Hemolytic disease
Teaching Aids: NNF
Causes of jaundice
After 72 hours of age
Sepsis
Cephalhaematoma
Neonatal hepatitis
Extra-hepatic biliary
Teaching Aids: NNF
Causes of jaundice
After 72 hours of age
Sepsis
Cephalhaematoma
Neonatal hepatitis
Extra-hepatic biliary
Teaching Aids: NNF
The general symptoms of Neonatal Jaundice
Yellow skin
Yellow eyes(sclera)
Sleepiness
Poor
Teaching Aids: NNF
The general symptoms of Neonatal Jaundice
Yellow skin
Yellow eyes(sclera)
Sleepiness
Poor
Teaching Aids: NNF
Risk factors for jaundice
JAUNDICE
J - jaundice within first
Teaching Aids: NNF
Risk factors for jaundice
JAUNDICE
J - jaundice within first
Teaching Aids: NNF
Common causes
Physiological
Blood group incompatibility
G6PD deficiency
Bruising and cephalhaematoma
Intrauterine and
Teaching Aids: NNF
Common causes
Physiological
Blood group incompatibility
G6PD deficiency
Bruising and cephalhaematoma
Intrauterine and
Teaching Aids: NNF
Approach to jaundiced baby
Ascertain birth weight, gestation and postnatal
Teaching Aids: NNF
Approach to jaundiced baby
Ascertain birth weight, gestation and postnatal
Teaching Aids: NNF
Workup
Maternal & perinatal history
Physical examination
Laboratory tests (must in all)*
Total
Teaching Aids: NNF
Workup
Maternal & perinatal history
Physical examination
Laboratory tests (must in all)*
Total
Teaching Aids: NNF
Management
Rationale: reduce level of serum bilirubin and prevent bilirubin
Teaching Aids: NNF
Management
Rationale: reduce level of serum bilirubin and prevent bilirubin
Teaching Aids: NNF
Principle of phototherapy
Native bilirubin Photo isomers of bilirubin
Insoluble Soluble
450-460nm
of
Teaching Aids: NNF
Principle of phototherapy
Native bilirubin Photo isomers of bilirubin
Insoluble Soluble
450-460nm
of
Teaching Aids: NNF
Phototherapy equipment
White light tubes 6-8*/ 4 blue light tubes
Cradle
Teaching Aids: NNF
Phototherapy equipment
White light tubes 6-8*/ 4 blue light tubes
Cradle
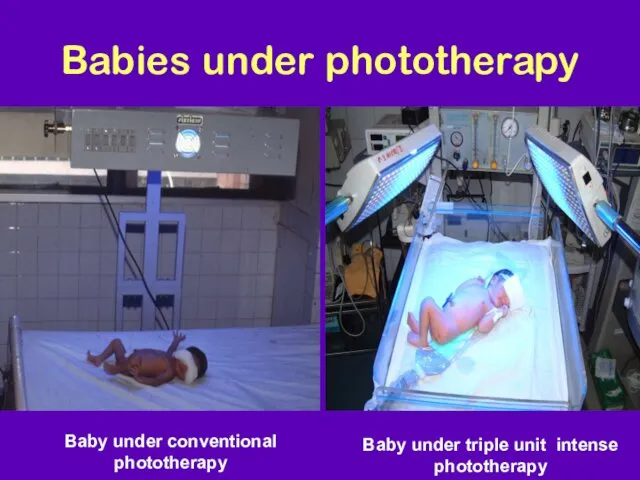
Babies under phototherapy
Baby under conventional phototherapy
Baby under triple unit intense phototherapy
Babies under phototherapy
Baby under conventional phototherapy
Baby under triple unit intense phototherapy
Teaching Aids: NNF
Phototherapy
Technique
Perform hand wash
Place baby naked in cradle or incubator
Fix
Teaching Aids: NNF
Phototherapy
Technique
Perform hand wash
Place baby naked in cradle or incubator
Fix
Teaching Aids: NNF
Phototherapy
Frequent extra breast feeding every 2 hourly
Turn baby after
Teaching Aids: NNF
Phototherapy
Frequent extra breast feeding every 2 hourly
Turn baby after

Teaching Aids: NNF
Diffential Diagnoses
Breast Milk Jaundice
Cholestatis
Dubin-Johnson Syndrome
GalactoseMIA
Teaching Aids: NNF
Diffential Diagnoses
Breast Milk Jaundice
Cholestatis
Dubin-Johnson Syndrome
GalactoseMIA
Teaching Aids: NNF
Side effects of phototherapy
Increased insensible water loss
Loose stools
Skin rash
Bronze
Teaching Aids: NNF
Side effects of phototherapy
Increased insensible water loss
Loose stools
Skin rash
Bronze
Teaching Aids: NNF
Choice of blood for exchange
blood transfusion
ABO incompatibility
Use O blood
Teaching Aids: NNF
Choice of blood for exchange
blood transfusion
ABO incompatibility
Use O blood
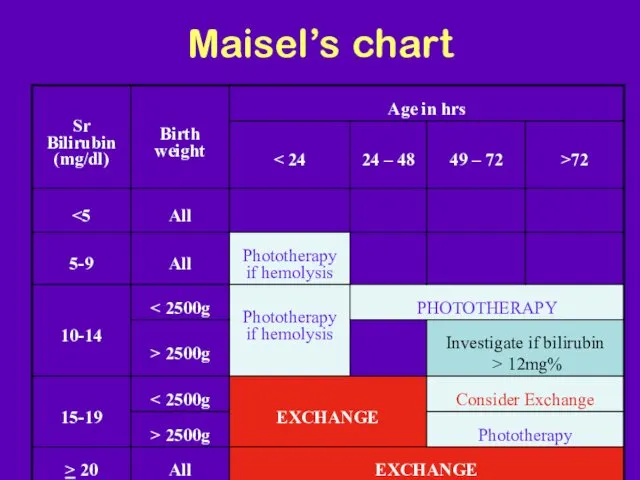
Maisel’s chart
Maisel’s chart
Teaching Aids: NNF
Prolonged indirect jaundice
Causes
Crigler Najjar syndrome
Breast milk jaundice
Hypothyroidism
Pyloric stenosis
Ongoing hemolysis,
Teaching Aids: NNF
Prolonged indirect jaundice
Causes
Crigler Najjar syndrome
Breast milk jaundice
Hypothyroidism
Pyloric stenosis
Ongoing hemolysis,
Teaching Aids: NNF
Conjugated hyperbilirubinemia
Suspect
High colored urine
White or clay colored stool
Teaching Aids: NNF
Conjugated hyperbilirubinemia
Suspect
High colored urine
White or clay colored stool
Teaching Aids: NNF
Conjugated hyperbilirubinemia
Causes
Idiopathic neonatal hepatitis
Infections -Hepatitis B, TORCH, sepsis
Biliary
Teaching Aids: NNF
Conjugated hyperbilirubinemia
Causes
Idiopathic neonatal hepatitis
Infections -Hepatitis B, TORCH, sepsis
Biliary
 Микотоксины. Действие микотоксинов в истории
Микотоксины. Действие микотоксинов в истории Общие принципы лечения абсцессов и флегмон лица и шеи. Физиотерапия и реабилитация больных
Общие принципы лечения абсцессов и флегмон лица и шеи. Физиотерапия и реабилитация больных Диспансерное наблюдение за детьми с хроническими заболеваниями
Диспансерное наблюдение за детьми с хроническими заболеваниями Хронические расстройства питания у детей
Хронические расстройства питания у детей Наследственные заболевания человека
Наследственные заболевания человека Геморрагический шок
Геморрагический шок Гипогликемическая и гипергликемическая комы
Гипогликемическая и гипергликемическая комы Пути введения лекарственных средств
Пути введения лекарственных средств Обзор и принципы реанимации новорожденных
Обзор и принципы реанимации новорожденных Современные алгоритмы лечения сахарного диабета 2 типа
Современные алгоритмы лечения сахарного диабета 2 типа Нейропсихологическая диагностика
Нейропсихологическая диагностика Общая характеристика группы инфекционных болезней с воздушнокапельным механизмом передачи. Грипп
Общая характеристика группы инфекционных болезней с воздушнокапельным механизмом передачи. Грипп Вагинальные инфекции при беременности
Вагинальные инфекции при беременности Federal State Educational Institution of Higher Education
Federal State Educational Institution of Higher Education Синдром наличия жидкости и газа в плевральной полости. Плевриты
Синдром наличия жидкости и газа в плевральной полости. Плевриты Холера. Эпидемиология
Холера. Эпидемиология Хронический пылевой бронхит
Хронический пылевой бронхит Легочное сердце
Легочное сердце Инфекционный мононуклеоз у детей
Инфекционный мононуклеоз у детей Понятие гиподинамии, гипердинамии
Понятие гиподинамии, гипердинамии Действия ассистента, осуществляемые до прихода врача-стоматолога, после прихода врача-стоматолога и после окончания лечения
Действия ассистента, осуществляемые до прихода врача-стоматолога, после прихода врача-стоматолога и после окончания лечения Митральные пороки сердца
Митральные пороки сердца Критерии и качества стоматологических материалов. Система международных и национальных стандартов
Критерии и качества стоматологических материалов. Система международных и национальных стандартов Введение в венерологию. История развития венерологии. Инфекции, передающиеся половым путем
Введение в венерологию. История развития венерологии. Инфекции, передающиеся половым путем Доказательная профилактика. Скрининговые программы
Доказательная профилактика. Скрининговые программы Endocrine system
Endocrine system Современные подходы к лечению эндометриоидных кист яичников
Современные подходы к лечению эндометриоидных кист яичников Дисфункционалдық жатырдан қан кету
Дисфункционалдық жатырдан қан кету