- Bipolar disorder

Содержание
- 2. Bipolar Disorder It is a spectrum of affective episodes including: Major depressive episode Manic episode Mixed
- 3. Bipolar Disorder may manifest itself only by its maniac or depressive phases (the monopolar course). In
- 4. Longitudinal Assessment of the Course of Bipolar Disorders Polarity of Symptoms Euthymia Depression Mania Subsyndromal Depression
- 5. Subtypes of Bipolar Disorder Bipolar I: Depression with Classic Mania Bipolar II: Depression with Hypomania Bipolar
- 6. Bipolar I or II Disorder ? What is the difference? Bipolar I 1+ manic or mixed
- 7. Prevalence Rates and Course Bipolar I Lifetime: 0.4-0.8 % = in men and women Men>manic episodes
- 8. Prevalence Rates and Course Bipolar II Lifetime: 0.5% May be more common in women than men
- 9. Causes
- 10. Genetics
- 11. Hereditary Factors 1st degree relatives have significantly higher rates Twin and adoption studies indicate genetic predisposition
- 12. Biochemical Hypothesis low level of norepinephrine Dopamine implicated in the study of mania and psychotic symptoms
- 13. Alterations in Brain Function: Neurotransmission (NT) Model Catecholamine hypothesis: Same hypothesis for schizophrenia & major depression
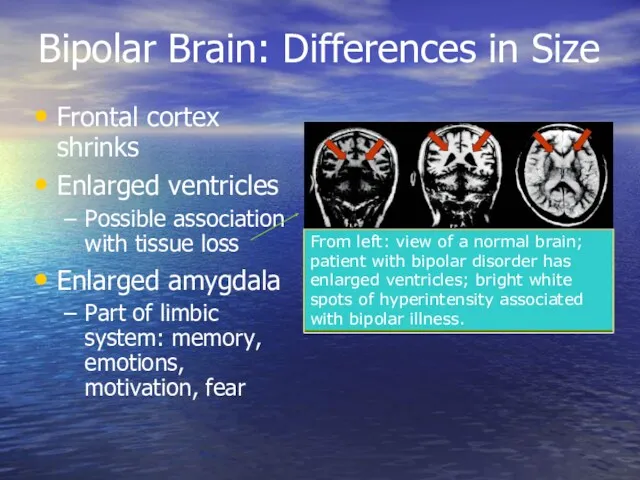
- 14. Bipolar Brain: Differences in Size Frontal cortex shrinks Enlarged ventricles Possible association with tissue loss Enlarged
- 15. The Limbic System
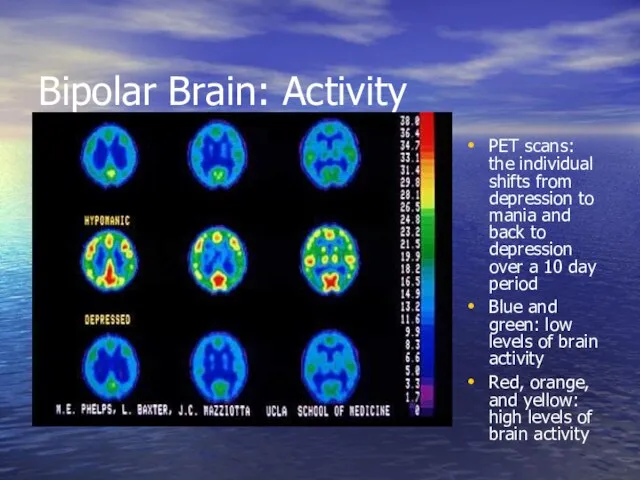
- 16. Bipolar Brain: Activity PET scans: the individual shifts from depression to mania and back to depression
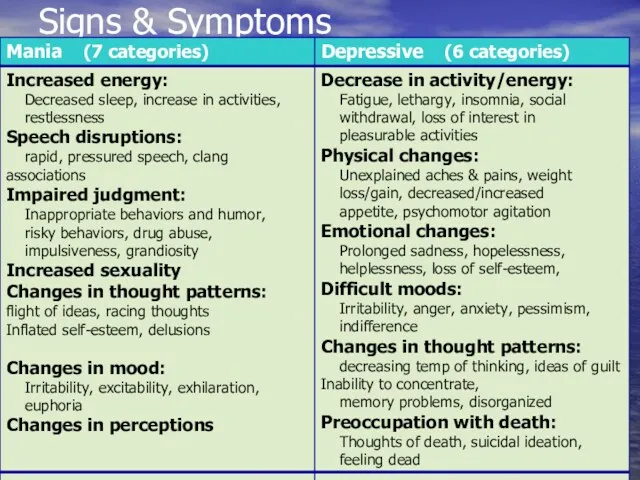
- 17. Signs & Symptoms
- 18. Depressive phase - Depressive syndrome sad and melancholic mood a delayed thinking a motor inhibition
- 19. Hypothymia Decreasing speed of Speech Hypoactivity 3 Signs in 3 Days The Unmistakable Triad of Depressive
- 20. Major Depressive Episode —Diagnostic Criteria Five or more of the following symptoms are present most of
- 21. Major Depressive Disorder —Diagnostic Criteria Five or more of the following symptoms are present most of
- 22. SUICIDE RISK Must Be Continually Monitored Suicide completion rates in patients with B.D. 10-15% Presence of
- 23. Diagnostic Criteria Hypomanic Episode: A. A distinct period of abnormally and persistently elevated, expansive, or irritable
- 24. Diagnostic Criteria Hypomanic Episode: 1) inflated self-esteem or grandiosity 2) decreased need for sleep ( feels
- 25. Diagnostic Criteria Hypomanic Episode: (continued) 4) flight of ideas or subjective experience that thoughts are racing
- 26. Diagnostic Criteria Hypomanic Episode: (continued) 7) excessive involvement in pleasurable activities that have a high potential
- 27. Manic Episode - Manic syndrome inadequately high spirits acceleration of associative processes a motor excitement
- 28. Euphoria Pressured Speech Hyperactivity 3 Signs in 3 Days The Unmistakable Triad of Manic Episode
- 29. Diagnostic Criteria Manic Episode: A. A distinct period of abnormally and persistently elevated, expansive, or irritable
- 30. Diagnostic Criteria Manic Episode: (continued) C. The symptoms do not meet criteria for a Mixed Episode.
- 31. Diagnostic Criteria Manic Episode: (continued) E. The symptoms are not connected with the direct physiological effects
- 32. Mixed Episode Rapidly alternating moods (sadness, irritability, euphoria) accompanied by criteria for both a Manic Episode
- 33. Dysthymic Disorder Major Depressive Disorder Cyclothymic Disorder Bipolar I Disorder Bipolar II Disorder
- 34. Treatment options for bipolar depression Normothymics Psychotherapy Electroconvulsive Therapy (ECT) Antidepressants Antipsychotics
- 35. Medications for Bipolar Disorder Mood Stabilizers Divalproex DR Divalproex ER Carbamazepine ER Lamotrigine - M Lithium
- 36. Lithium Much often recommended treatment for Bipolar Disorder 60-80% success in reducing acute manic and hypomanic
- 37. Side Effects and Toxicity of Lithium Lithium demonstrates a narrow therapeutic window- close to toxic dose
- 38. Lithium Doesn’t Work? 40% of patients with Bipolar disorder are resistant to lithium or side effects
- 39. Valproic Acid (Depakote) An anti-epileptic, it is probably the more often used anti-manic drug Best for
- 40. Carbamazepine (Tegretol) Superior to lithium for rapid-cycling, regarded as a second-line treatment for mania Side effects
- 41. Blood Monitoring Blood level monitoring required for Tegretol and Depakote. Weekly and then every 3 months.
- 42. Atypical Antipsychotics: Don’t be afraid of the word “antipsychotic”
- 43. Medications for Bipolar Disorder Second Generation Antipsychotics Aripiprazole - M Olanzapine - M Quetiapine - Depr
- 44. Atypical Antipsychotics (AAPs) Olanzapine (Zyprexa) 2.5mg-20mg/day Quetiapine (Seroquel) 12.5-600mg/day Risperidone (Risperdal) 0.25mg-6mg/d Ziprasidone (Geodon) 20-160mg a
- 45. Atypical Anti-psychotics No support for use as primary first-line agents 4 types that more often used
- 46. ECT 1] Mania very severe and not responding to medications. 2] Patient prefers ECT 3] Pregnant
- 47. Classic & New Antidepressants Tricyclics, Tetracyclics (TCA) 5-HT Reuptake Inhibitors (SSRI) Fluoxetine (& R-FLX), Paroxetine, Sertraline,
- 48. SSRIs Dosage Fluoxetine [Prozac] 10-80 mg/d Paroxetine [Paxil] 10-50 mg/d Sertraline [Zoloft] 25-200 mg/d Fluvoxamine [Luvox]
- 49. Evidence-based, psychosocial treatments for bipolar disorder Cognitive-behavioral therapy (CBT) Interpersonal and Social rhythm psychotherapy (IPSRT) Family-focused
- 50. Psychoeducation 21 groups sessions of 90 minutes each Topics include: Awareness of the disorder (6 sessions)
- 51. Schizoaffective Disorder
- 52. Schizoaffective disorder Endogenic psychosis Mixed symptoms of schizophrenia and mood disorder (manic or depression) Intense periods
- 53. Schizoaffective Disorder Difficulty in conceptualization Risk for suicide (attempts in 23 to 42%) Less common than
- 54. schizoaffective disorder patients meets diagnostic criteria for both schizophrenia and an affective (mood) disorder— depression or
- 55. Etiology Possible causes of schizoaffective disorder are similar to those of schizophrenia (lust lecture)
- 56. Biologic Theories of Causation Genetic predisposition Neuropathologic changes Overactivity of dopamine system Positive symptoms of schizoaffective
- 57. Classification Schizoaffective disorder. Depressions type Schizoaffective disorder. Manic type Schizoaffective disorder. Mixed type
- 58. Diagnostic Criteria for Schizoaffective Disorder At least two symptoms of psychosis from among the following, present
- 59. Diagnostic Criteria for Schizoaffective Disorder Delusions or hallucinations have occurred for at least two weeks in
- 60. Signs and symptoms of schizoaffective disorder may include Strange or unusual thoughts or perceptions Paranoid thoughts
- 61. Treatment Normothymics are a mainstay of treatment for bipolar disorders and would be expected to be
- 62. Treatment Antipsychotics (neuroleptics) to treat psychotic symptoms, such as delusions and hallucinations. paliperidone (Invega) clozapine (Clozaril,
- 63. Treatment Antidepressants. When depression is the main mood disorder, antidepressants Fluoxetine [Prozac] 10-80 mg/d Paroxetine [Paxil]
- 65. Скачать презентацию
Bipolar Disorder
It is a spectrum of affective episodes including:
Major depressive episode
Manic
Bipolar Disorder
It is a spectrum of affective episodes including:
Major depressive episode
Manic
Bipolar Disorder
may manifest itself only by its maniac or depressive phases
Bipolar Disorder
may manifest itself only by its maniac or depressive phases
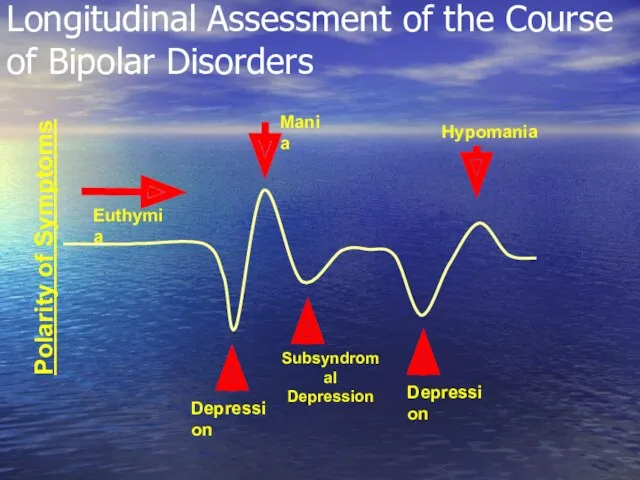
Longitudinal Assessment of the Course of Bipolar Disorders
Polarity of Symptoms
Euthymia
Depression
Mania
Subsyndromal
Depression
Depression
Hypomania
Longitudinal Assessment of the Course of Bipolar Disorders
Polarity of Symptoms
Euthymia
Depression
Mania
Subsyndromal
Depression
Depression
Hypomania
Subtypes of Bipolar Disorder
Bipolar I: Depression with Classic Mania
Bipolar II:
Subtypes of Bipolar Disorder
Bipolar I: Depression with Classic Mania
Bipolar II:
Bipolar I or II Disorder ?
What is the difference?
Bipolar I
1+ manic
Bipolar I or II Disorder ?
What is the difference?
Bipolar I
1+ manic
Prevalence Rates and Course
Bipolar I
Lifetime: 0.4-0.8 %
= in men and women
Men>manic
Prevalence Rates and Course
Bipolar I
Lifetime: 0.4-0.8 %
= in men and women
Men>manic
Prevalence Rates and Course
Bipolar II
Lifetime: 0.5%
May be more common in women
Prevalence Rates and Course
Bipolar II
Lifetime: 0.5%
May be more common in women
Causes
Causes
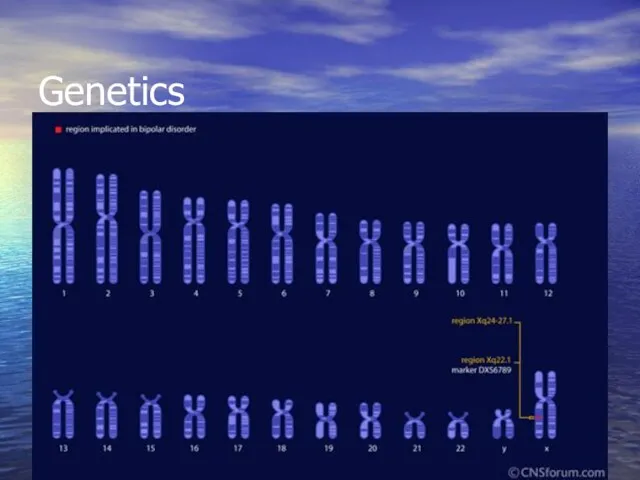
Genetics
Genetics
Hereditary Factors
1st degree relatives have significantly higher rates
Twin and adoption studies
Hereditary Factors
1st degree relatives have significantly higher rates
Twin and adoption studies
Biochemical Hypothesis
low level of norepinephrine
Dopamine implicated in the study of mania
Biochemical Hypothesis
low level of norepinephrine
Dopamine implicated in the study of mania
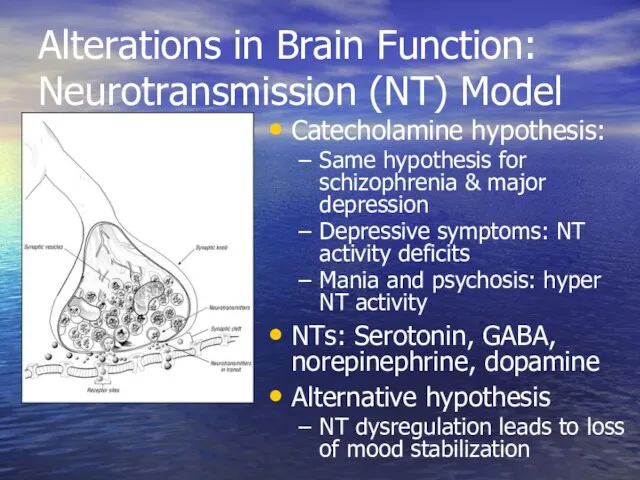
Alterations in Brain Function: Neurotransmission (NT) Model
Catecholamine hypothesis:
Same hypothesis for schizophrenia
Alterations in Brain Function: Neurotransmission (NT) Model
Catecholamine hypothesis:
Same hypothesis for schizophrenia
Bipolar Brain: Differences in Size
Frontal cortex shrinks
Enlarged ventricles
Possible association with tissue
Bipolar Brain: Differences in Size
Frontal cortex shrinks
Enlarged ventricles
Possible association with tissue
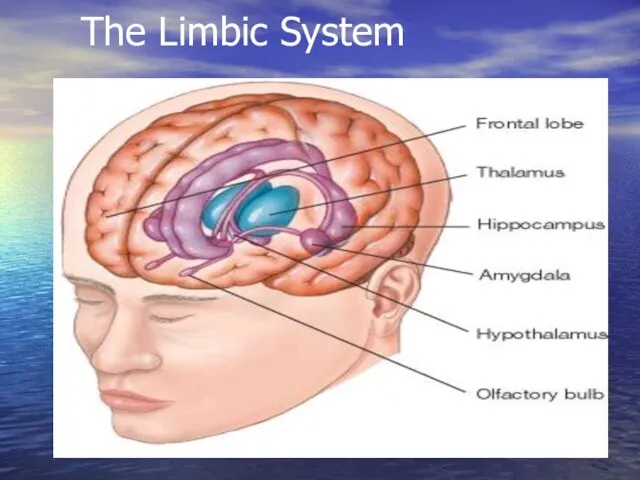
The Limbic System
The Limbic System
Bipolar Brain: Activity
PET scans: the individual shifts from depression to mania
Bipolar Brain: Activity
PET scans: the individual shifts from depression to mania
Signs & Symptoms
Signs & Symptoms
Depressive phase - Depressive syndrome
sad and melancholic mood
a delayed
Depressive phase - Depressive syndrome
sad and melancholic mood
a delayed

Hypothymia
Decreasing speed of Speech Hypoactivity
3 Signs in 3 Days
The Unmistakable Triad
Hypothymia
Decreasing speed of Speech Hypoactivity
3 Signs in 3 Days
The Unmistakable Triad
Major Depressive Episode
—Diagnostic Criteria
Five or more of the following symptoms are
Major Depressive Episode
—Diagnostic Criteria
Five or more of the following symptoms are
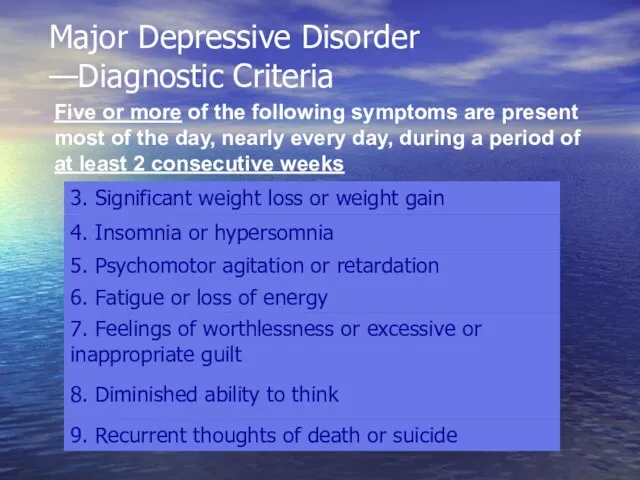
Major Depressive Disorder
—Diagnostic Criteria
Five or more of the following symptoms are
Major Depressive Disorder
—Diagnostic Criteria
Five or more of the following symptoms are
SUICIDE RISK
Must Be Continually Monitored
Suicide completion rates in patients with
SUICIDE RISK
Must Be Continually Monitored
Suicide completion rates in patients with
Diagnostic Criteria
Hypomanic Episode:
A. A distinct period of abnormally and persistently
Diagnostic Criteria
Hypomanic Episode:
A. A distinct period of abnormally and persistently
Diagnostic Criteria
Hypomanic Episode:
1) inflated self-esteem or grandiosity
2) decreased need for
Diagnostic Criteria
Hypomanic Episode:
1) inflated self-esteem or grandiosity
2) decreased need for
Diagnostic Criteria
Hypomanic Episode: (continued)
4) flight of ideas or subjective experience that
Diagnostic Criteria
Hypomanic Episode: (continued)
4) flight of ideas or subjective experience that
Diagnostic Criteria
Hypomanic Episode: (continued)
7) excessive involvement in pleasurable activities that have
Diagnostic Criteria
Hypomanic Episode: (continued)
7) excessive involvement in pleasurable activities that have
Manic Episode - Manic syndrome
inadequately high spirits
acceleration of associative processes
Manic Episode - Manic syndrome
inadequately high spirits
acceleration of associative processes

Euphoria
Pressured Speech Hyperactivity
3 Signs in 3 Days
The Unmistakable Triad of Manic
Euphoria
Pressured Speech Hyperactivity
3 Signs in 3 Days
The Unmistakable Triad of Manic
Diagnostic Criteria
Manic Episode:
A. A distinct period of abnormally and persistently elevated,
Diagnostic Criteria
Manic Episode:
A. A distinct period of abnormally and persistently elevated,
Diagnostic Criteria
Manic Episode: (continued)
C. The symptoms do not meet criteria for
Diagnostic Criteria
Manic Episode: (continued)
C. The symptoms do not meet criteria for
Diagnostic Criteria
Manic Episode: (continued)
E. The symptoms are not connected with the
Diagnostic Criteria
Manic Episode: (continued)
E. The symptoms are not connected with the
Mixed Episode
Rapidly alternating moods (sadness, irritability, euphoria) accompanied by criteria for
Mixed Episode
Rapidly alternating moods (sadness, irritability, euphoria) accompanied by criteria for
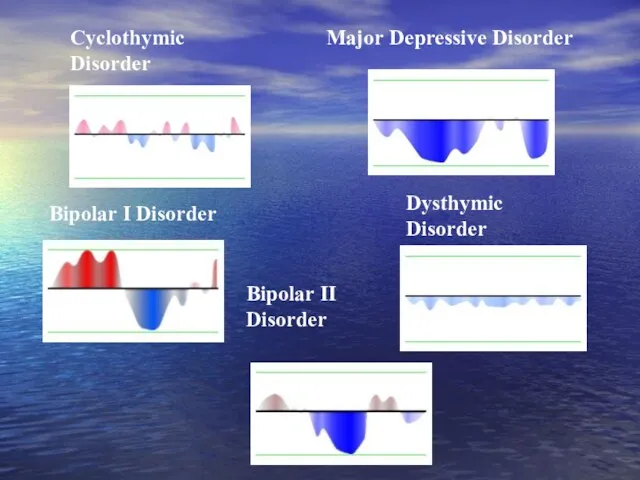
Dysthymic Disorder
Major Depressive Disorder
Cyclothymic Disorder
Bipolar I Disorder
Bipolar II Disorder
Dysthymic Disorder
Major Depressive Disorder
Cyclothymic Disorder
Bipolar I Disorder
Bipolar II Disorder
Treatment options for bipolar depression
Normothymics
Psychotherapy
Electroconvulsive Therapy (ECT)
Antidepressants
Antipsychotics
Treatment options for bipolar depression
Normothymics
Psychotherapy
Electroconvulsive Therapy (ECT)
Antidepressants
Antipsychotics
Medications for Bipolar Disorder
Mood Stabilizers
Divalproex DR Divalproex ER
Carbamazepine ER
Lamotrigine
Medications for Bipolar Disorder
Mood Stabilizers
Divalproex DR Divalproex ER
Carbamazepine ER
Lamotrigine
Lithium
Much often recommended treatment for Bipolar Disorder
60-80% success in reducing acute
Lithium
Much often recommended treatment for Bipolar Disorder
60-80% success in reducing acute
Side Effects and Toxicity of Lithium
Lithium demonstrates a narrow therapeutic window-
Side Effects and Toxicity of Lithium
Lithium demonstrates a narrow therapeutic window-
Lithium Doesn’t Work?
40% of patients with Bipolar disorder are resistant to
Lithium Doesn’t Work?
40% of patients with Bipolar disorder are resistant to
Valproic Acid (Depakote)
An anti-epileptic, it is probably the more often used
Valproic Acid (Depakote)
An anti-epileptic, it is probably the more often used
Carbamazepine (Tegretol)
Superior to lithium for rapid-cycling, regarded as a second-line treatment
Carbamazepine (Tegretol)
Superior to lithium for rapid-cycling, regarded as a second-line treatment
Blood Monitoring
Blood level monitoring required for Tegretol and Depakote.
Weekly and then
Blood Monitoring
Blood level monitoring required for Tegretol and Depakote.
Weekly and then
Atypical Antipsychotics:
Don’t be afraid of the word “antipsychotic”
Atypical Antipsychotics:
Don’t be afraid of the word “antipsychotic”
Medications for Bipolar Disorder
Second Generation Antipsychotics
Aripiprazole - M
Olanzapine - M
Quetiapine
Medications for Bipolar Disorder
Second Generation Antipsychotics
Aripiprazole - M
Olanzapine - M
Quetiapine
Atypical Antipsychotics (AAPs)
Olanzapine (Zyprexa) 2.5mg-20mg/day
Quetiapine (Seroquel) 12.5-600mg/day
Risperidone (Risperdal) 0.25mg-6mg/d
Ziprasidone (Geodon) 20-160mg
Atypical Antipsychotics (AAPs)
Olanzapine (Zyprexa) 2.5mg-20mg/day
Quetiapine (Seroquel) 12.5-600mg/day
Risperidone (Risperdal) 0.25mg-6mg/d
Ziprasidone (Geodon) 20-160mg
Atypical Anti-psychotics
No support for use as primary first-line agents
4 types that
Atypical Anti-psychotics
No support for use as primary first-line agents
4 types that
![ECT 1] Mania very severe and not responding to medications.](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/428749/slide-45.jpg)
ECT
1] Mania very severe and not responding to medications.
2] Patient prefers
ECT
1] Mania very severe and not responding to medications.
2] Patient prefers

Classic & New Antidepressants
Tricyclics, Tetracyclics (TCA)
5-HT Reuptake Inhibitors (SSRI)
Fluoxetine (& R-FLX),
Classic & New Antidepressants
Tricyclics, Tetracyclics (TCA)
5-HT Reuptake Inhibitors (SSRI)
Fluoxetine (& R-FLX),
![SSRIs Dosage Fluoxetine [Prozac] 10-80 mg/d Paroxetine [Paxil] 10-50 mg/d](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/428749/slide-47.jpg)
SSRIs Dosage
Fluoxetine [Prozac] 10-80 mg/d
Paroxetine [Paxil] 10-50 mg/d
Sertraline [Zoloft] 25-200 mg/d
Fluvoxamine
SSRIs Dosage
Fluoxetine [Prozac] 10-80 mg/d
Paroxetine [Paxil] 10-50 mg/d
Sertraline [Zoloft] 25-200 mg/d
Fluvoxamine
Evidence-based, psychosocial treatments
for bipolar disorder
Cognitive-behavioral therapy (CBT)
Interpersonal and Social rhythm psychotherapy
Evidence-based, psychosocial treatments
for bipolar disorder
Cognitive-behavioral therapy (CBT)
Interpersonal and Social rhythm psychotherapy
Psychoeducation
21 groups sessions of 90 minutes each
Topics include:
Awareness of the disorder
Psychoeducation
21 groups sessions of 90 minutes each
Topics include:
Awareness of the disorder
Schizoaffective Disorder
Schizoaffective Disorder
Schizoaffective disorder
Endogenic psychosis
Mixed symptoms of schizophrenia and mood disorder (manic or
Schizoaffective disorder
Endogenic psychosis
Mixed symptoms of schizophrenia and mood disorder (manic or
Schizoaffective Disorder
Difficulty in conceptualization
Risk for suicide (attempts in 23 to 42%)
Less
Schizoaffective Disorder
Difficulty in conceptualization
Risk for suicide (attempts in 23 to 42%)
Less
schizoaffective disorder
patients meets diagnostic criteria for both schizophrenia and an affective
schizoaffective disorder
patients meets diagnostic criteria for both schizophrenia and an affective
Etiology
Possible causes of schizoaffective disorder are similar to those of schizophrenia
(lust
Etiology
Possible causes of schizoaffective disorder are similar to those of schizophrenia
(lust
Biologic Theories of Causation
Genetic predisposition
Neuropathologic changes
Overactivity of dopamine system
Positive symptoms of
Biologic Theories of Causation
Genetic predisposition
Neuropathologic changes
Overactivity of dopamine system
Positive symptoms of
Classification
Schizoaffective disorder. Depressions type
Schizoaffective disorder.
Manic type
Schizoaffective disorder.
Mixed
Classification
Schizoaffective disorder. Depressions type
Schizoaffective disorder.
Manic type
Schizoaffective disorder.
Mixed
Diagnostic Criteria for Schizoaffective Disorder
At least two symptoms of psychosis from
Diagnostic Criteria for Schizoaffective Disorder
At least two symptoms of psychosis from
Diagnostic Criteria for Schizoaffective Disorder
Delusions or hallucinations have occurred for at
Diagnostic Criteria for Schizoaffective Disorder
Delusions or hallucinations have occurred for at
Signs and symptoms of schizoaffective disorder may include
Strange or unusual thoughts
Signs and symptoms of schizoaffective disorder may include
Strange or unusual thoughts
Treatment
Normothymics are a mainstay of treatment for bipolar disorders and would
Treatment
Normothymics are a mainstay of treatment for bipolar disorders and would
Treatment
Antipsychotics (neuroleptics)
to treat psychotic symptoms, such as delusions and hallucinations.
paliperidone (Invega)
clozapine
Treatment
Antipsychotics (neuroleptics)
to treat psychotic symptoms, such as delusions and hallucinations.
paliperidone (Invega)
clozapine
Treatment
Antidepressants.
When depression is the main mood disorder, antidepressants
Fluoxetine [Prozac] 10-80
Treatment
Antidepressants.
When depression is the main mood disorder, antidepressants
Fluoxetine [Prozac] 10-80
 Аритмия. Нарушения ритма сердца
Аритмия. Нарушения ритма сердца Илік заттар (немесе тұтқыр заттар), тітіркендіруші заттар.қаптаушы заттар, адсорбциялаушы заттар
Илік заттар (немесе тұтқыр заттар), тітіркендіруші заттар.қаптаушы заттар, адсорбциялаушы заттар Гипоталамо-гипофизарлы семіздіктің визуалды диагностикасы
Гипоталамо-гипофизарлы семіздіктің визуалды диагностикасы Реабилитация недоношенных детей: особенности оценки физического развития и питания после выписки из стационара
Реабилитация недоношенных детей: особенности оценки физического развития и питания после выписки из стационара Organizations of different kinds of therapeutic-and-prophylactic help to population
Organizations of different kinds of therapeutic-and-prophylactic help to population Typhoid
Typhoid Meningococcal infection
Meningococcal infection Преднизолон. Фармакотерапевтическая группа
Преднизолон. Фармакотерапевтическая группа Протоколы реабилитации коленного сустава: от предоперационной подготовки до возврата к прежнему уровню спортивной активности
Протоколы реабилитации коленного сустава: от предоперационной подготовки до возврата к прежнему уровню спортивной активности Статеві гормони. Гормони наднирників. Гормони щитовидної залози. Гормони нейрогипофиза
Статеві гормони. Гормони наднирників. Гормони щитовидної залози. Гормони нейрогипофиза Инфекционные и неинфекционные заболевания. Профилактика
Инфекционные и неинфекционные заболевания. Профилактика Исследование мочи: физические и химические свойства
Исследование мочи: физические и химические свойства Сестринский уход за недоношенными детьми
Сестринский уход за недоношенными детьми Инфекционная безопасность в гибкой эндоскопии
Инфекционная безопасность в гибкой эндоскопии Рекомбинантные белки как лекарственные средства
Рекомбинантные белки как лекарственные средства Питающие устройства. Виды питающих устройств. Дозаторы.Питатели. Транспортные устройства и механизмы подачи
Питающие устройства. Виды питающих устройств. Дозаторы.Питатели. Транспортные устройства и механизмы подачи Расстройства кровообращения
Расстройства кровообращения Сестринский процесс при ревматоидном артрите, деформирующем остеоартрозе
Сестринский процесс при ревматоидном артрите, деформирующем остеоартрозе Пневмонии новорожденных. Этиология, патогенез, классификация, клиника
Пневмонии новорожденных. Этиология, патогенез, классификация, клиника Инфузионно-трансфузионная терапия. Показания и противопоказания
Инфузионно-трансфузионная терапия. Показания и противопоказания Ортодонтиялық емдеудің негізгі принциптер
Ортодонтиялық емдеудің негізгі принциптер Тыныс алу жүйесінің өмірге қауіпті зақымдануларының диагностикасы және жедел көмек көрсету алгоритмі
Тыныс алу жүйесінің өмірге қауіпті зақымдануларының диагностикасы және жедел көмек көрсету алгоритмі Особенности питания беременных женщин
Особенности питания беременных женщин Остановка наружного кровотечения
Остановка наружного кровотечения Системы здравоохранения. Задачи законодательства Российской Федерации об охране здоровья граждан
Системы здравоохранения. Задачи законодательства Российской Федерации об охране здоровья граждан Семиотика и диагностика заболеваний женской половой системы
Семиотика и диагностика заболеваний женской половой системы Glomerulonephritis in children chronic kidney failure
Glomerulonephritis in children chronic kidney failure Генные заболевания
Генные заболевания