- Common Laboratory Tests

Содержание
- 2. Let’s look at some nuances of 3 of most commonly ordered lab tests CBC (Complete Blood
- 3. CBC Complete blood count With or without differential Peripheral venous blood is collected in a lavendar
- 4. What is measured? Red blood cell data Total red blood cell count (RBC) Hemoglobin (Hgb) Hematocrit
- 5. Total Red Blood Cell Count Count of the number of circulating red blood cells in 1mm3
- 6. Hemoglobin The hemoglobin concentration is a measure of the amount of Hgb in the peripheral blood,
- 7. Hematocrit Hematocrit is a measure of the percentage of the total blood volume that is made
- 8. Centrifuged blood (normal) Red blood cells Buffy coat (WBCs and Platelets) Plasma Normal Hct in adult
- 9. Centrifuged blood (adult male or female) What is your diagnosis? Anemia – there is a low
- 10. Calculating the Hematocrit More commonly the Hct is calculated directly from the RBC and MCV Hematocrit
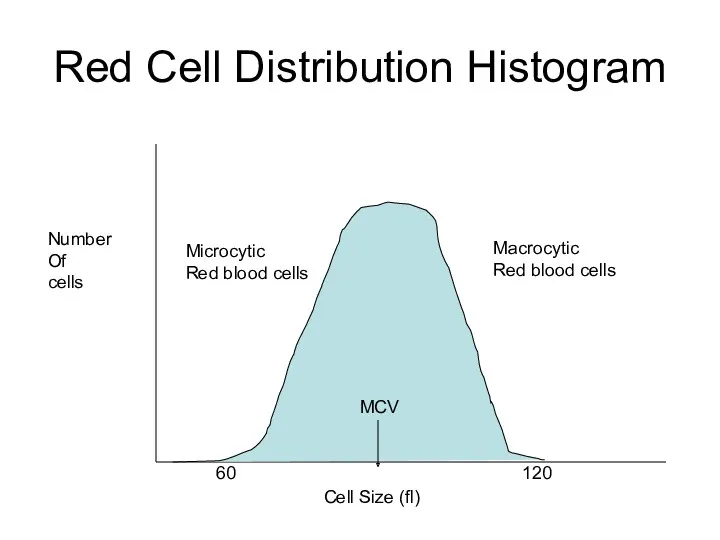
- 11. Mean Corpuscular Volume The MCV is a measure of the average volume, or size, of an
- 12. Cell Size (fl) Number Of cells 60 120 MCV Red Cell Distribution Histogram
- 13. Use of MCV Result The MCV is important in classifying anemias Normal MCV = normocytic anemia
- 14. Cell Size (fl) Number Of cells 60 120 MCV Red Cell Distribution Histogram Microcytic Red blood
- 15. Red Blood Cell Distribution Width RDW is an indication of the variation in the RBC size
- 16. White Blood Cell Count A count of the total WBC, or leukocyte, count in 1mm3 of
- 17. WBC Differential When a differential is ordered, the percentage of each type of leukocyte present in
- 18. Manual Differentials “Manual” WBC differentials are performed by trained medical technologists who count and categorize typically100
- 19. Automated Differentials The clinical laboratory may perform an “automated differential” Via instruments with the capability of
- 20. Platelet Count (PLT) A count of the number of platelets (thrombocytes) per cubic milliliter of blood
- 21. CBC as reported by LUMC Lab in the EPIC EMR Component Value Flag Low High Units
- 22. MCH and MCHC Note: Both MCH and MCHC are of little clinical diagnostic use in the
- 23. Interpretation? Essentially normal CBC WBC, Hgb, Hct, MCV, RDW, PLT count values are all within the
- 24. Absolute numbers (#) of various cell types are calculated by multiplying the percentage (%) of the
- 25. Interpret this CBC CBC WBC 19.5 [4.0-10.0] k/ul RBC 3.49 [3.60-5.50] m/ul Hgb 10.4 [12.0-16.0] gm/dl
- 26. Common Clinical Uses of CBC CBC demonstrates Leukocytosis Microcytic anemia with elevated red cell distribution width
- 27. One final CBC pearl Clinicians have a short-hand way to report CBC values: If we look
- 28. BMP (Basic Metabolic Panel)
- 29. BMP The BMP is a chemistry panel where multiple chemistry tests are grouped as a single
- 30. BMP Peripheral venous blood can be collected in several types of tube Light Green PST Plasma
- 31. Sodium Sodium is the major cation in the extracellular space where serum levels of approximately 140mmol/L
- 32. Potassium Potassium is the major intracellular cation with levels of ~ 4 mmol/L found in serum
- 33. Chloride Chloride is the major extracellular anion with serum concentration of ~ 100 mmol/L Hyperchloremia and
- 34. Carbon Dioxide Content The carbon dioxide content (CO2) measures the H2CO3, dissolved CO2 and bicarbonate ion
- 35. Blood Urea Nitrogen The BUN measures the amount of urea nitrogen in the blood. Urea is
- 36. Creatinine The creatinine test measures the amount of creatinine in the blood. Creatinine is a catabolic
- 37. Glucose Plasma glucose levels should be evaluated in relation to a patient’s meal i.e., postprandial vs
- 38. Diagnosing Diabetes The criteria for the diagnosis of diabetes: Fasting Plasma Glucose ≥126 mg/dL 2 hour
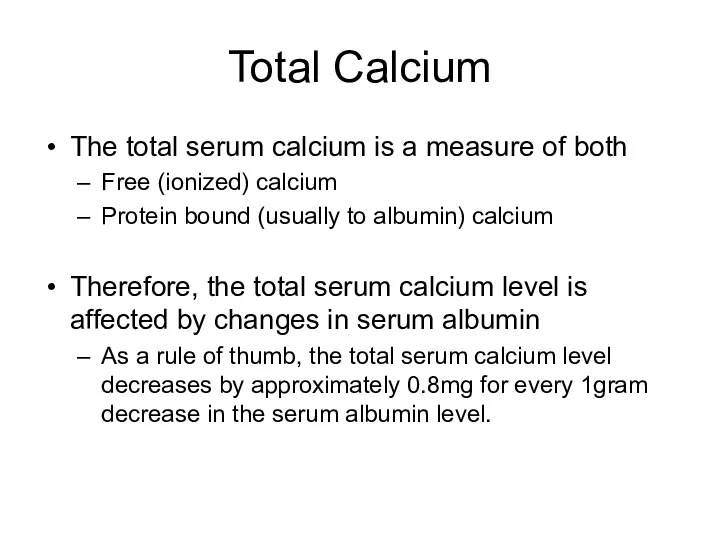
- 39. Total Calcium The total serum calcium is a measure of both Free (ionized) calcium Protein bound
- 40. BMP as reported by LUMC Lab in the EPIC EMR Component Value Flag Low High Units
- 41. Your Interpretation? This patient has mild hypocalcemia Any other test you would like to order? Serum
- 42. One final BMP pearl Clinicians have a short-hand way to report BMP values: If we look
- 43. CMP (Complete Metabolic Panel)
- 44. Complete Metabolic Panel The CMP provides a more extensive laboratory evaluation of organ dysfunction and includes:
- 45. Total Protein Albumin and globulin constitute most of the protein within the body and are measured
- 46. Albumin Albumin comprises ~ 60% of the total protein within the extracellular portion of the blood
- 47. Alkaline Phosphatase (Alk Phos or ALP) Alkaline phosphatase is an enzyme present in a number of
- 48. Bilirubin, Total The total serum bilirubin level is the sum of the conjugated (direct) and unconjugated
- 49. Aspartate Aminotransferase (AST) AST is an enzyme that is present in hepatocytes and myocytes (both skeletal
- 50. The following CMP is from a patient who presented with systolic congestive heart failure exacerbation Complete
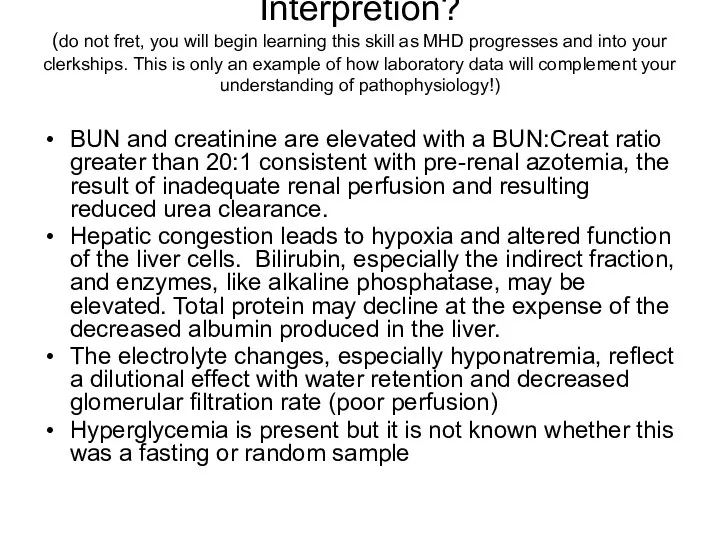
- 51. Interpretion? (do not fret, you will begin learning this skill as MHD progresses and into your
- 52. Final Comments… Excessive laboratory tests can cause iatrogenic anemia! Although the goal of ordering any “blood
- 53. Final Comments… No laboratory test should ever be ordered unless it is medically necessary
- 55. Скачать презентацию
Let’s look at some nuances of 3 of most commonly ordered
Let’s look at some nuances of 3 of most commonly ordered
CBC
Complete blood count
With or without differential
Peripheral venous blood is collected in
CBC
Complete blood count
With or without differential
Peripheral venous blood is collected in
What is measured?
Red blood cell data
Total red blood cell count (RBC)
Hemoglobin
What is measured?
Red blood cell data
Total red blood cell count (RBC)
Hemoglobin
Total Red Blood Cell Count
Count of the number of circulating red
Total Red Blood Cell Count
Count of the number of circulating red
Hemoglobin
The hemoglobin concentration is a measure of the amount of Hgb
Hemoglobin
The hemoglobin concentration is a measure of the amount of Hgb
Hematocrit
Hematocrit is a measure of the percentage of the total blood
Hematocrit
Hematocrit is a measure of the percentage of the total blood
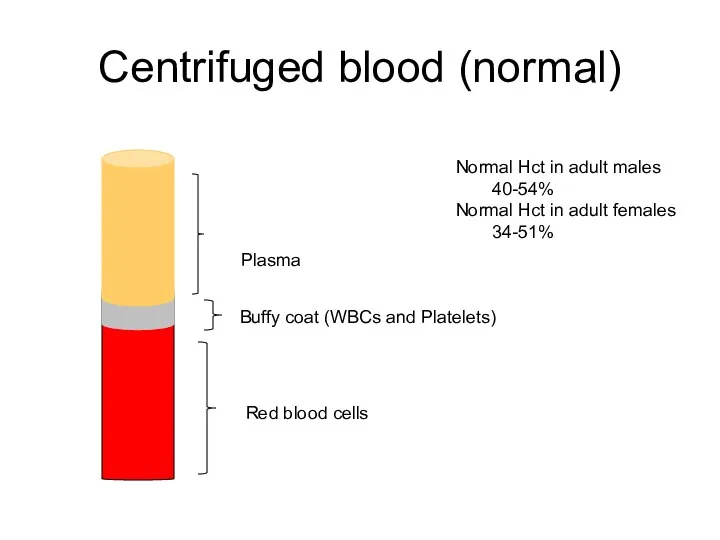
Centrifuged blood (normal)
Red blood cells
Buffy coat (WBCs and Platelets)
Plasma
Normal Hct
Centrifuged blood (normal)
Red blood cells
Buffy coat (WBCs and Platelets)
Plasma
Normal Hct
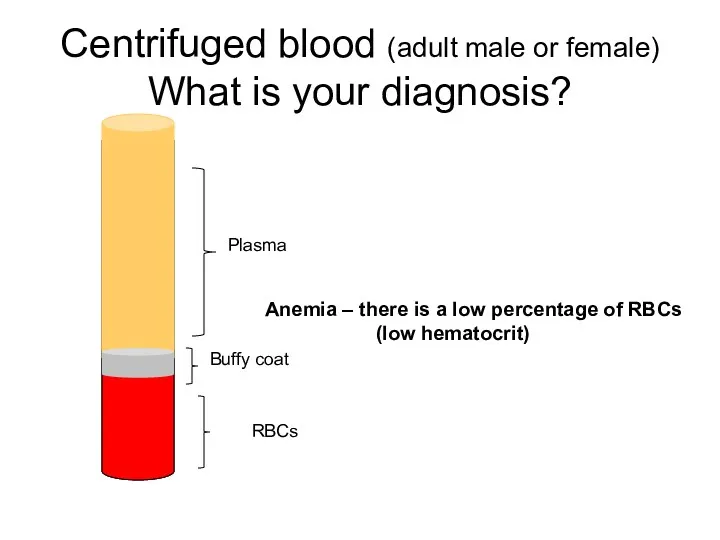
Centrifuged blood (adult male or female)
What is your diagnosis?
Anemia – there
Centrifuged blood (adult male or female)
What is your diagnosis?
Anemia – there
Calculating the Hematocrit
More commonly the Hct is calculated directly from
Calculating the Hematocrit
More commonly the Hct is calculated directly from
Mean Corpuscular Volume
The MCV is a measure of the average volume,
Mean Corpuscular Volume
The MCV is a measure of the average volume,
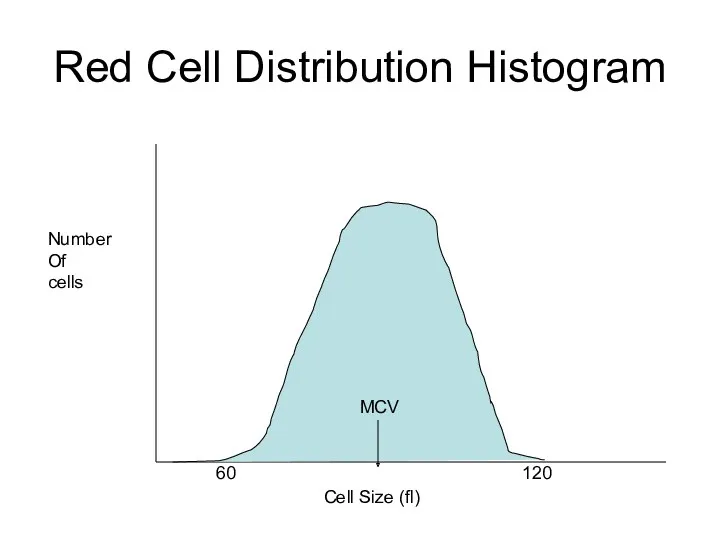
Cell Size (fl)
Number
Of
cells
60
120
MCV
Red Cell Distribution Histogram
Cell Size (fl)
Number
Of
cells
60
120
MCV
Red Cell Distribution Histogram
Use of MCV Result
The MCV is important in classifying anemias
Normal MCV
Use of MCV Result
The MCV is important in classifying anemias
Normal MCV
Cell Size (fl)
Number
Of
cells
60
120
MCV
Red Cell Distribution Histogram
Microcytic
Red blood cells
Macrocytic
Red
Cell Size (fl)
Number
Of
cells
60
120
MCV
Red Cell Distribution Histogram
Microcytic
Red blood cells
Macrocytic
Red
Red Blood Cell Distribution Width
RDW is an indication of the variation
Red Blood Cell Distribution Width
RDW is an indication of the variation
White Blood Cell Count
A count of the total WBC, or leukocyte,
White Blood Cell Count
A count of the total WBC, or leukocyte,
WBC Differential
When a differential is ordered, the percentage of each type
WBC Differential
When a differential is ordered, the percentage of each type
Manual Differentials
“Manual” WBC differentials are performed by trained medical technologists who
Manual Differentials
“Manual” WBC differentials are performed by trained medical technologists who
Automated Differentials
The clinical laboratory may perform an “automated differential”
Via instruments
Automated Differentials
The clinical laboratory may perform an “automated differential”
Via instruments
Platelet Count (PLT)
A count of the number of platelets (thrombocytes) per
Platelet Count (PLT)
A count of the number of platelets (thrombocytes) per
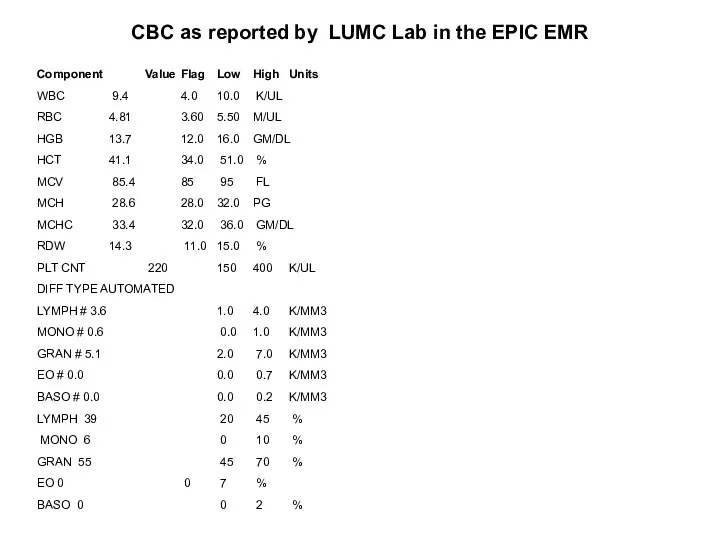
CBC as reported by LUMC Lab in the EPIC EMR
Component Value
CBC as reported by LUMC Lab in the EPIC EMR
Component Value
MCH and MCHC
Note:
Both MCH and MCHC are of little clinical diagnostic
MCH and MCHC
Note:
Both MCH and MCHC are of little clinical diagnostic
Interpretation?
Essentially normal CBC
WBC, Hgb, Hct, MCV, RDW, PLT count values are
Interpretation?
Essentially normal CBC
WBC, Hgb, Hct, MCV, RDW, PLT count values are
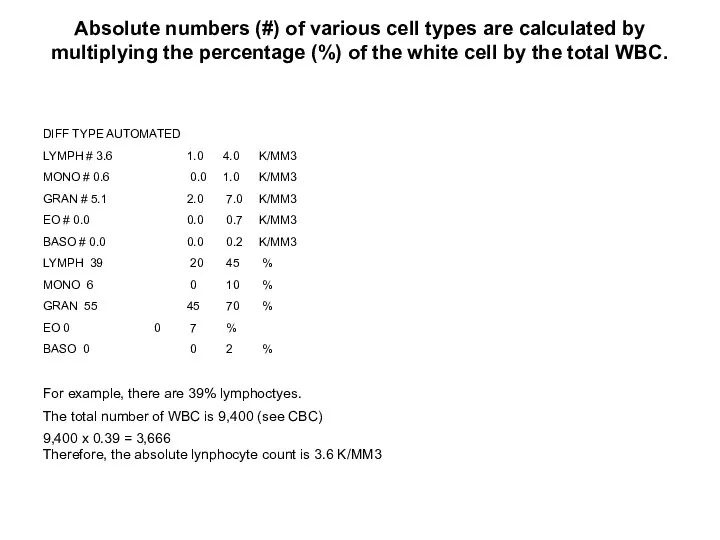
Absolute numbers (#) of various cell types are calculated by multiplying
Absolute numbers (#) of various cell types are calculated by multiplying
![Interpret this CBC CBC WBC 19.5 [4.0-10.0] k/ul RBC 3.49](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/409094/slide-24.jpg)
Interpret this CBC
CBC
WBC 19.5 [4.0-10.0] k/ul
RBC 3.49 [3.60-5.50] m/ul
Hgb 10.4
Interpret this CBC
CBC
WBC 19.5 [4.0-10.0] k/ul
RBC 3.49 [3.60-5.50] m/ul
Hgb 10.4
Common Clinical Uses of CBC
CBC demonstrates
Leukocytosis
Microcytic anemia with elevated red cell
Common Clinical Uses of CBC
CBC demonstrates
Leukocytosis
Microcytic anemia with elevated red cell
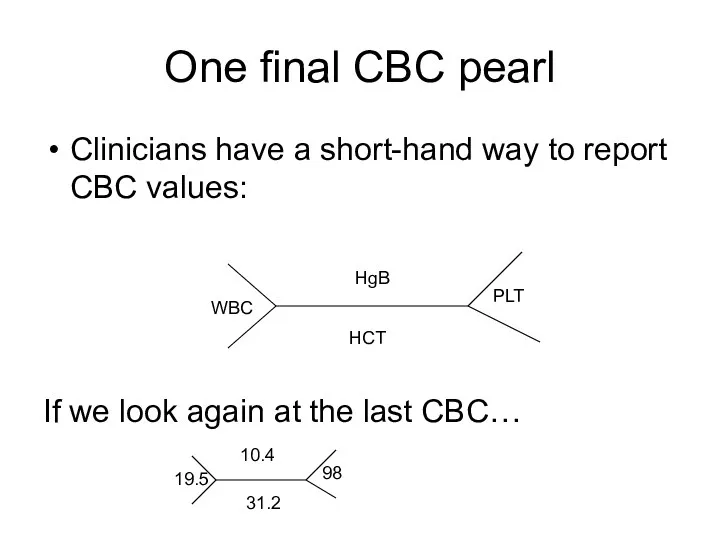
One final CBC pearl
Clinicians have a short-hand way to report CBC
One final CBC pearl
Clinicians have a short-hand way to report CBC
BMP
(Basic Metabolic Panel)
BMP
(Basic Metabolic Panel)
BMP
The BMP is a chemistry panel where multiple chemistry tests are
BMP
The BMP is a chemistry panel where multiple chemistry tests are
BMP
Peripheral venous blood can be collected in several types of tube
Light
BMP
Peripheral venous blood can be collected in several types of tube
Light
Sodium
Sodium is the major cation in the extracellular space where serum
Sodium
Sodium is the major cation in the extracellular space where serum
Potassium
Potassium is the major intracellular cation with levels of ~ 4
Potassium
Potassium is the major intracellular cation with levels of ~ 4
Chloride
Chloride is the major extracellular anion with serum concentration of ~
Chloride
Chloride is the major extracellular anion with serum concentration of ~
Carbon Dioxide Content
The carbon dioxide content (CO2) measures the H2CO3, dissolved
Carbon Dioxide Content
The carbon dioxide content (CO2) measures the H2CO3, dissolved
Blood Urea Nitrogen
The BUN measures the amount of urea nitrogen in
Blood Urea Nitrogen
The BUN measures the amount of urea nitrogen in
Creatinine
The creatinine test measures the amount of creatinine in the blood.
Creatinine
Creatinine
The creatinine test measures the amount of creatinine in the blood.
Creatinine
Glucose
Plasma glucose levels should be evaluated in relation to a patient’s
Glucose
Plasma glucose levels should be evaluated in relation to a patient’s
Diagnosing Diabetes
The criteria for the diagnosis of diabetes:
Fasting Plasma Glucose ≥126
Diagnosing Diabetes
The criteria for the diagnosis of diabetes:
Fasting Plasma Glucose ≥126
Total Calcium
The total serum calcium is a measure of both
Free (ionized)
Total Calcium
The total serum calcium is a measure of both
Free (ionized)
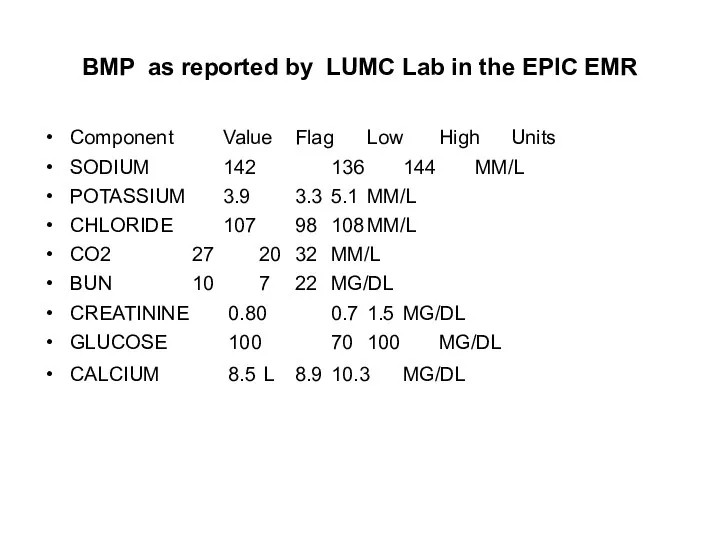
BMP as reported by LUMC Lab in the EPIC EMR
Component Value
BMP as reported by LUMC Lab in the EPIC EMR
Component Value
Your Interpretation?
This patient has mild hypocalcemia
Any other test you would like
Your Interpretation?
This patient has mild hypocalcemia
Any other test you would like
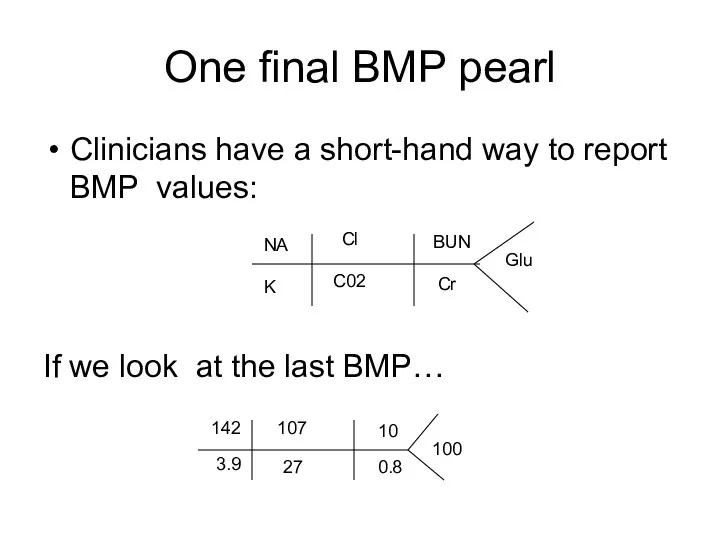
One final BMP pearl
Clinicians have a short-hand way to report BMP
One final BMP pearl
Clinicians have a short-hand way to report BMP
CMP
(Complete Metabolic Panel)
CMP
(Complete Metabolic Panel)
Complete Metabolic Panel
The CMP provides a more extensive laboratory evaluation of
Complete Metabolic Panel
The CMP provides a more extensive laboratory evaluation of
Total Protein
Albumin and globulin constitute most of the protein within the
Total Protein
Albumin and globulin constitute most of the protein within the
Albumin
Albumin comprises ~ 60% of the total protein within the extracellular
Albumin
Albumin comprises ~ 60% of the total protein within the extracellular
Alkaline Phosphatase
(Alk Phos or ALP)
Alkaline phosphatase is an enzyme present
Alkaline Phosphatase
(Alk Phos or ALP)
Alkaline phosphatase is an enzyme present
Bilirubin, Total
The total serum bilirubin level is the sum of the
Bilirubin, Total
The total serum bilirubin level is the sum of the
Aspartate Aminotransferase
(AST)
AST is an enzyme that is present in hepatocytes and
Aspartate Aminotransferase
(AST)
AST is an enzyme that is present in hepatocytes and
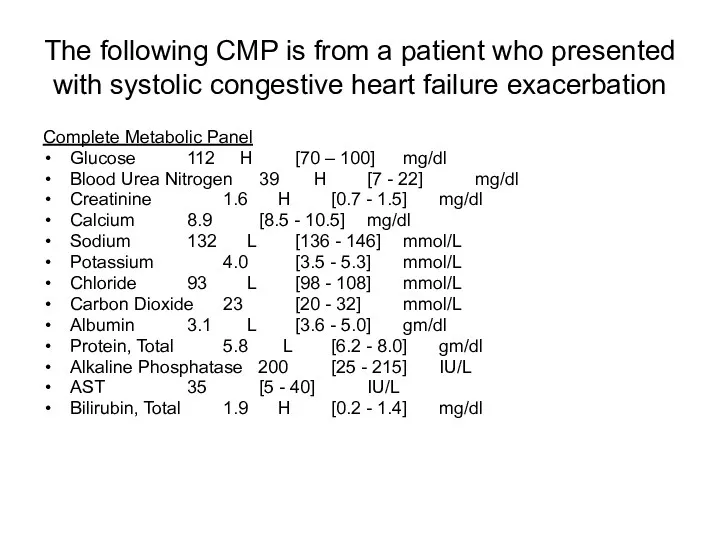
The following CMP is from a patient who presented with systolic
The following CMP is from a patient who presented with systolic
Interpretion?
(do not fret, you will begin learning this skill as MHD
Interpretion? (do not fret, you will begin learning this skill as MHD
Final Comments…
Excessive laboratory tests can cause iatrogenic anemia!
Although the goal of
Final Comments…
Excessive laboratory tests can cause iatrogenic anemia!
Although the goal of
Final Comments…
No laboratory test should ever be ordered unless it is
Final Comments…
No laboratory test should ever be ordered unless it is
 Бүйрек аурулары
Бүйрек аурулары Нейропсихологические синдромы нарушения памяти. Методы нейропсихологического обследования. Восстановительная работа
Нейропсихологические синдромы нарушения памяти. Методы нейропсихологического обследования. Восстановительная работа Гостра серцева недостатність
Гостра серцева недостатність Всемирный день иммунитета
Всемирный день иммунитета The final impression
The final impression Рак шейки и тела матки
Рак шейки и тела матки Симптоматология острого и хронического гломерулонефрита, пиелонефрита, почечной недостаточности
Симптоматология острого и хронического гломерулонефрита, пиелонефрита, почечной недостаточности Анатомия пәні және мақсаты. Тіндерге, ағзаларға және ағзалар жүйесіне жалпы сипаттама. Адам эмбриогенезінің алғашқы сатысы
Анатомия пәні және мақсаты. Тіндерге, ағзаларға және ағзалар жүйесіне жалпы сипаттама. Адам эмбриогенезінің алғашқы сатысы Лекарственные препараты
Лекарственные препараты Eating Disorders
Eating Disorders ОРВИ и грипп
ОРВИ и грипп Twins diagnostic methods
Twins diagnostic methods Принципы терапии острой почечной недостаточности. Патогенетические сдвиги, клиническая картина
Принципы терапии острой почечной недостаточности. Патогенетические сдвиги, клиническая картина Вывихи и переломы зубов, альвеолярного отростка. Методы лечения
Вывихи и переломы зубов, альвеолярного отростка. Методы лечения Жүктілік және Туберкулез
Жүктілік және Туберкулез Основные аспекты содержания и методики АФК. Адаптивная физическая культура
Основные аспекты содержания и методики АФК. Адаптивная физическая культура Воспаление. Этиология. Медиаторы. Виды. Острое воспаление
Воспаление. Этиология. Медиаторы. Виды. Острое воспаление Павел Захарович Кондоиди (1710-1760)
Павел Захарович Кондоиди (1710-1760) Лабораторная диагностика стафилококковой инфекции
Лабораторная диагностика стафилококковой инфекции Анафилактикалық және гиповолемиялық шок
Анафилактикалық және гиповолемиялық шок Клиническая фармакология лекарственных средств, влияющих на гемостаз
Клиническая фармакология лекарственных средств, влияющих на гемостаз First aid
First aid Жүктілік кезіндегі жатыр мойнының рагі
Жүктілік кезіндегі жатыр мойнының рагі Патофизиология опухолевого роста
Патофизиология опухолевого роста СП при раке желудка
СП при раке желудка Краснуха
Краснуха Возрождение, медицина
Возрождение, медицина Лечение огнестрельных ранений живота
Лечение огнестрельных ранений живота