- Diagnosis and mangement of abnormal labour

Содержание
- 2. Labor refers to uterine contractions resulting in progressive dilation and effacement of the cervix, and accompanied
- 3. Abnormal labor, dystocia, and failure to progress are imprecise terms that have been used to describe
- 4. A better classification is to characterize labor abnormalities as protraction disorders (ie, slower than normal progress)
- 5. Approximately 20 percent of labors involve either protraction or arrest disorders A labor abnormality is the
- 6. NORMAL LABOR Friedman, in his classic studies, divided labor into three stages First stage: time from
- 7. NORMAL LABOR Third stage: time from expulsion of the fetus to expulsion of the placenta The
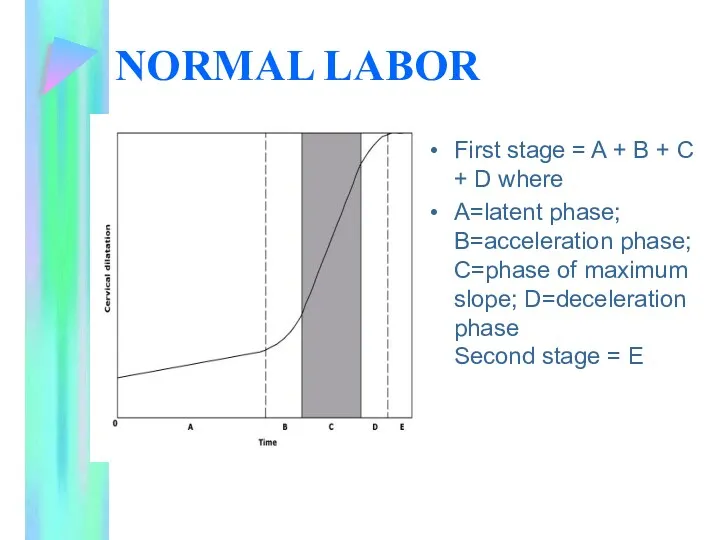
- 8. NORMAL LABOR First stage = A + B + C + D where A=latent phase; B=acceleration
- 9. Latent phase The onset of the latent phase of labor begins when the mother perceives regular
- 10. Latent phase This phase is typically characterized by mild infrequent contractions and a gradual change in
- 11. Latent phase The average duration of latent phase in nulliparous and multiparous women is 6.4 and
- 12. Latent phase An abnormally long latent phase is defined as 20 hours for the nullipara and
- 13. Active phase The beginning of the active phase typically occurs when the cervix has reached 3
- 14. Active phase The active phase is characterized by painful contractions of increasing frequency, intensity, and duration
- 15. Active phase The average duration of the active phase in nulliparous and parous women is 4.6
- 16. Active phase An abnormally long active phase is defined as 12 hours for the nullipara and
- 17. Second stage The mean duration of the second stage of labor in nulliparous and multiparous women
- 18. Second stage abnormally long second stage as three hours for the nulliparous and one hour for
- 19. Second stage Neuraxial anesthesia, duration of the first stage, parity, maternal size, birth weight, and station
- 20. Second stage (ACOG) recommends that the normal duration of second stage of labor be based upon
- 21. Normal uterine activity Uterine activity can be monitored by palpation, external tocodynamometry, or internal uterine pressure
- 22. Normal uterine activity External and intrauterine monitoring devices appear to perform equally well, although the latter
- 23. Normal uterine activity Ninety-five percent of women in active labor will have three to five contractions
- 24. Normal uterine activity Montevideo units (ie, the peak strength of contractions in mmHg measured by an
- 25. Normal uterine activity 91 percent of women in spontaneous active labor achieved contractile activity greater than
- 26. CLASSIFICATION AND DIAGNOSIS OF LABOR ABNORMALITIES
- 27. Diagnostic criteria for abnormal patterns in active labor Values represent approximately two standard deviations from the
- 28. Protraction and arrest disorders occur in both the first and second stages of labor The incidence
- 29. In the first stage of labor progressive dilatation slower than the rate shown in the table
- 30. An arrest disorder can be diagnosed when the cervix ceases to dilate after reaching four or
- 31. second stage of labor protracted labor is defined as a second stage longer than two hours
- 32. An arrest of descent can be diagnosed after one hour if there is no descent, despite
- 33. labor can be too fast as well as too slow The term precipitous labor refers to
- 34. ETIOLOGY Abnormal labor can be the result of one or more abnormalities of the cervix, uterus,
- 35. Risk factors for abnormal labor
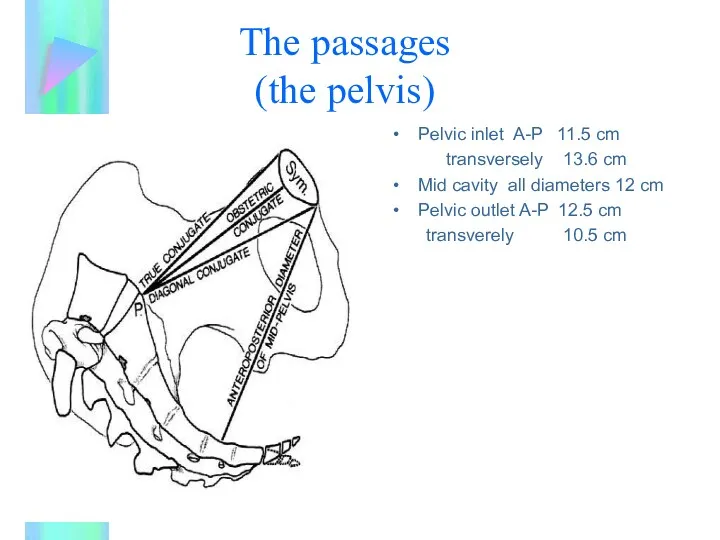
- 36. The passages (the pelvis) Pelvic inlet A-P 11.5 cm transversely 13.6 cm Mid cavity all diameters
- 37. The passages (the pelvis) The clinician's ability to predict maternal pelvis-fetal size discordance (cephalopelvic disproportion) leading
- 38. Clinical or radiologic assessment of the maternal pelvis (ie, pelvimetry) is associated with poor predictive value
- 39. The passenger Fetal weight, larger babies will have greater difficulty in passing through the pelvis Unfavorable
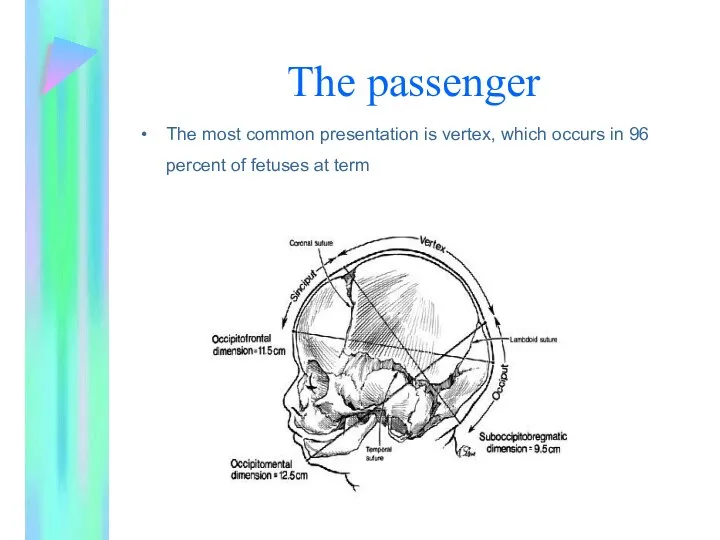
- 40. The passenger The most common presentation is vertex, which occurs in 96 percent of fetuses at
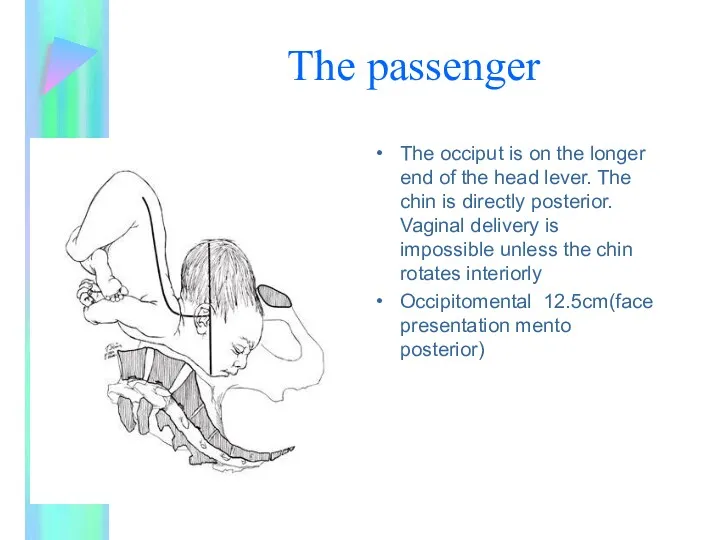
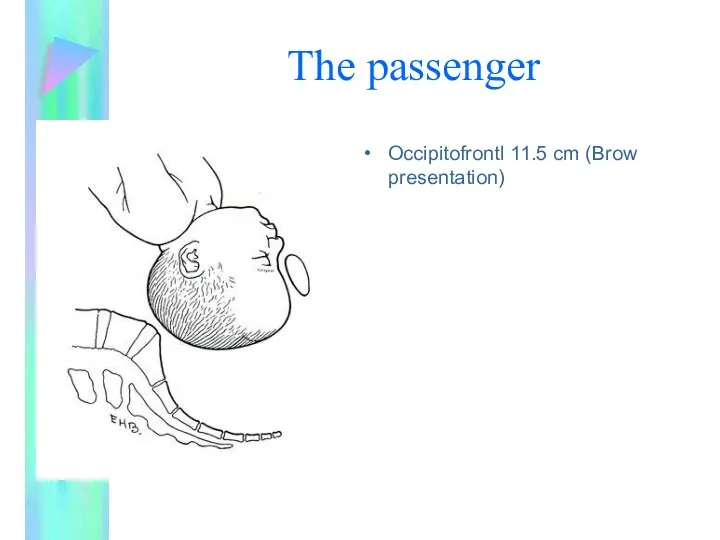
- 41. The passenger The occiput is on the longer end of the head lever. The chin is
- 42. The passenger Occipitofrontl 11.5 cm (Brow presentation)
- 43. The powers Hypocontractile uterine activity is the most common cause of protraction or arrest disorders in
- 44. The powers This entity refers to uterine activity that is either not sufficiently strong or not
- 45. The powers It occurs in 3 to 8 percent of parturients and can be quantified as
- 46. The powers Neuraxial anesthesia neuraxial anesthesia is associated with an increased duration of the first and
- 47. The powers Neuraxial anesthesia has not been proven to increase the rate of cesarean delivery
- 48. The powers It is possible that changes in neuraxial technique or drugs (eg, use of narcotics
- 49. The powers The consequences of withdrawing the block before the second stage of labor, appropriate use
- 50. MANAGEMENT disciplined approach to the diagnosis of labor, assessment of maternal and fetal well-being, and careful
- 51. Advancement of cervical dilation charted on a partogram.
- 52. MANAGEMENT Poor progression in the first stage Hypocontractile uterine activity is treated with oxytocin, which is
- 53. MANAGEMENT Other — Other interventions, such as ambulation and continuous labor support, may increase the comfort
- 54. MANAGEMENT Poor progression in the second stage Three options: Continued observation Attempt at operative vaginal delivery
- 56. Скачать презентацию
Labor refers to uterine contractions resulting in progressive dilation and effacement
Labor refers to uterine contractions resulting in progressive dilation and effacement
Abnormal labor, dystocia, and failure to progress are imprecise terms that
Abnormal labor, dystocia, and failure to progress are imprecise terms that
A better classification is to characterize labor abnormalities as protraction disorders
A better classification is to characterize labor abnormalities as protraction disorders
Approximately 20 percent of labors involve either protraction or arrest disorders
A
Approximately 20 percent of labors involve either protraction or arrest disorders
A
NORMAL LABOR
Friedman, in his classic studies, divided labor into three
NORMAL LABOR
Friedman, in his classic studies, divided labor into three
NORMAL LABOR
Third stage: time from expulsion of the fetus to expulsion
NORMAL LABOR
Third stage: time from expulsion of the fetus to expulsion
NORMAL LABOR
First stage = A + B + C + D
NORMAL LABOR
First stage = A + B + C + D
Latent phase
The onset of the latent phase of labor begins
Latent phase
The onset of the latent phase of labor begins
Latent phase
This phase is typically characterized by mild infrequent contractions and
Latent phase
This phase is typically characterized by mild infrequent contractions and
Latent phase
The average duration of latent phase in nulliparous and multiparous
Latent phase
The average duration of latent phase in nulliparous and multiparous
Latent phase
An abnormally long latent phase is defined as 20 hours
Latent phase
An abnormally long latent phase is defined as 20 hours
Active phase
The beginning of the active phase typically occurs when
Active phase
The beginning of the active phase typically occurs when
Active phase
The active phase is characterized by painful contractions of increasing
Active phase
The active phase is characterized by painful contractions of increasing
Active phase
The average duration of the active phase in nulliparous and
Active phase
The average duration of the active phase in nulliparous and
Active phase
An abnormally long active phase is defined as 12 hours
Active phase
An abnormally long active phase is defined as 12 hours
Second stage
The mean duration of the second stage of labor
Second stage
The mean duration of the second stage of labor
Second stage
abnormally long second stage as three hours for the nulliparous
Second stage
abnormally long second stage as three hours for the nulliparous
Second stage
Neuraxial anesthesia, duration of the first stage, parity, maternal size,
Second stage
Neuraxial anesthesia, duration of the first stage, parity, maternal size,
Second stage
(ACOG) recommends that the normal duration of second stage of
Second stage
(ACOG) recommends that the normal duration of second stage of
Normal uterine activity
Uterine activity can be monitored by palpation, external
Normal uterine activity
Uterine activity can be monitored by palpation, external
Normal uterine activity
External and intrauterine monitoring devices appear to perform equally
Normal uterine activity
External and intrauterine monitoring devices appear to perform equally
Normal uterine activity
Ninety-five percent of women in active labor will have
Normal uterine activity
Ninety-five percent of women in active labor will have
Normal uterine activity
Montevideo units (ie, the peak strength of contractions in
Normal uterine activity
Montevideo units (ie, the peak strength of contractions in
Normal uterine activity
91 percent of women in spontaneous active labor achieved
Normal uterine activity
91 percent of women in spontaneous active labor achieved
CLASSIFICATION AND DIAGNOSIS OF LABOR ABNORMALITIES
CLASSIFICATION AND DIAGNOSIS OF LABOR ABNORMALITIES
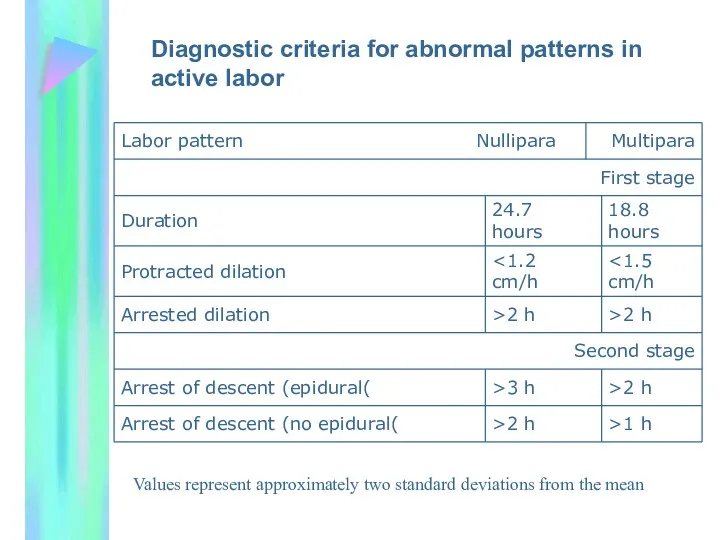
Diagnostic criteria for abnormal patterns in active labor
Values represent approximately
Diagnostic criteria for abnormal patterns in active labor
Values represent approximately
Protraction and arrest disorders occur in both the first and second
Protraction and arrest disorders occur in both the first and second
In the first stage of labor
progressive dilatation slower than the
In the first stage of labor
progressive dilatation slower than the
An arrest disorder can be diagnosed when the cervix ceases to
An arrest disorder can be diagnosed when the cervix ceases to
second stage of labor
protracted labor is defined as a second stage
second stage of labor
protracted labor is defined as a second stage
An arrest of descent can be diagnosed after one hour if
An arrest of descent can be diagnosed after one hour if
labor can be too fast as well as too slow
labor can be too fast as well as too slow
ETIOLOGY
Abnormal labor can be the result of one or more
ETIOLOGY
Abnormal labor can be the result of one or more
Risk factors for abnormal labor
Risk factors for abnormal labor
The passages
(the pelvis)
Pelvic inlet A-P 11.5 cm
transversely 13.6 cm
Mid cavity
The passages
(the pelvis)
Pelvic inlet A-P 11.5 cm
transversely 13.6 cm
Mid cavity
The passages
(the pelvis)
The clinician's ability to predict maternal pelvis-fetal size discordance
The passages
(the pelvis)
The clinician's ability to predict maternal pelvis-fetal size discordance
Clinical or radiologic assessment of the maternal pelvis (ie, pelvimetry) is
Clinical or radiologic assessment of the maternal pelvis (ie, pelvimetry) is
The passenger
Fetal weight, larger babies will have greater difficulty in passing
The passenger
Fetal weight, larger babies will have greater difficulty in passing
The passenger
The most common presentation is vertex, which occurs in 96
The passenger
The most common presentation is vertex, which occurs in 96
The passenger
The occiput is on the longer end of the head
The passenger
The occiput is on the longer end of the head
The passenger
Occipitofrontl 11.5 cm (Brow presentation)
The passenger
Occipitofrontl 11.5 cm (Brow presentation)
The powers
Hypocontractile uterine activity is the most common cause of protraction
The powers
Hypocontractile uterine activity is the most common cause of protraction
The powers
This entity refers to uterine activity that is either not
The powers
This entity refers to uterine activity that is either not
The powers
It occurs in 3 to 8 percent of parturients and
The powers
It occurs in 3 to 8 percent of parturients and
The powers
Neuraxial anesthesia
neuraxial anesthesia is associated with an increased duration
The powers
Neuraxial anesthesia
neuraxial anesthesia is associated with an increased duration
The powers
Neuraxial anesthesia has not been proven to increase the rate
The powers
Neuraxial anesthesia has not been proven to increase the rate
The powers
It is possible that changes in neuraxial technique or drugs
The powers
It is possible that changes in neuraxial technique or drugs
The powers
The consequences of withdrawing the block before the second stage
The powers
The consequences of withdrawing the block before the second stage

MANAGEMENT
disciplined approach to the diagnosis of labor, assessment of maternal
MANAGEMENT
disciplined approach to the diagnosis of labor, assessment of maternal
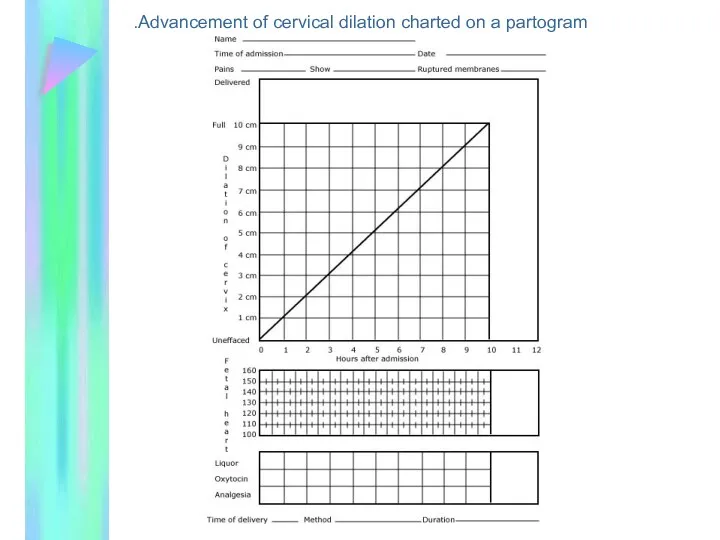
Advancement of cervical dilation charted on a partogram.
Advancement of cervical dilation charted on a partogram.
MANAGEMENT
Poor progression in the first stage
Hypocontractile uterine activity is treated
MANAGEMENT
Poor progression in the first stage
Hypocontractile uterine activity is treated
MANAGEMENT
Other — Other interventions, such as ambulation and continuous labor support, may increase
MANAGEMENT
Other — Other interventions, such as ambulation and continuous labor support, may increase
MANAGEMENT
Poor progression in the second stage
Three options:
Continued observation
Attempt at
MANAGEMENT
Poor progression in the second stage
Three options:
Continued observation
Attempt at
 Инфузионная терапия
Инфузионная терапия Мышцы тазового пояса и свободной нижней конечности. (Лекция 8)
Мышцы тазового пояса и свободной нижней конечности. (Лекция 8) Симптомы и методы обследования при заболеваниях почек
Симптомы и методы обследования при заболеваниях почек Презентация Шестакова Ф-21
Презентация Шестакова Ф-21 Травмы. Повреждения головы, груди, живота
Травмы. Повреждения головы, груди, живота Миома матки. Эндометриоз
Миома матки. Эндометриоз Вопросы женского здоровья и профилактики онкологических заболеваний
Вопросы женского здоровья и профилактики онкологических заболеваний Эндокринная система. Структурная организация эндокринной системы. Гормоны. Механизмы действия гормонов
Эндокринная система. Структурная организация эндокринной системы. Гормоны. Механизмы действия гормонов Қан ферменттерін анықтаудың клиникалық маңызы
Қан ферменттерін анықтаудың клиникалық маңызы Қағанақ суының босануға дейін ағып кетуі
Қағанақ суының босануға дейін ағып кетуі Эффективность применения Меркурида над химиотерапией в лечении острого лимфобластного лейкоза у детей
Эффективность применения Меркурида над химиотерапией в лечении острого лимфобластного лейкоза у детей Полипы органов желудочно-кишечного тракта. Этиология. Патогенез
Полипы органов желудочно-кишечного тракта. Этиология. Патогенез Энергозатраты организма
Энергозатраты организма Клиника дифференцированных олигофрении
Клиника дифференцированных олигофрении История развития патофизиологии
История развития патофизиологии Патогенные клостридии
Патогенные клостридии Гериатрия. Современные теории старения
Гериатрия. Современные теории старения Суд над комп’ютером. Вплив комп'ютера на здоров'я людини
Суд над комп’ютером. Вплив комп'ютера на здоров'я людини ЛС, применяемые в аллергологии
ЛС, применяемые в аллергологии Аллергия. Аллергические реакции
Аллергия. Аллергические реакции Фасции таза. Дефекты тазовой фасции и способы их коррекции
Фасции таза. Дефекты тазовой фасции и способы их коррекции Организация личной гигиены
Организация личной гигиены Методы лабораторной, инструментальной диагностики заболеваний ЖКТ
Методы лабораторной, инструментальной диагностики заболеваний ЖКТ Особенности лечения различных клинических вариантов аллергического ринита у детей раннего возраста
Особенности лечения различных клинических вариантов аллергического ринита у детей раннего возраста Оценка и классификация больного ребенка по кашлю или затрудненному дыханию
Оценка и классификация больного ребенка по кашлю или затрудненному дыханию Топографическая анатомия и оперативная хирургия головы
Топографическая анатомия и оперативная хирургия головы ЖРДС. Этиология мен патогенез, клиникасы, диагностикасы, емі
ЖРДС. Этиология мен патогенез, клиникасы, диагностикасы, емі Нейропсихологический анализ нарушений эмоционально-личностной сферы при локальных поражениях мозга
Нейропсихологический анализ нарушений эмоционально-личностной сферы при локальных поражениях мозга