- Peptic ulcer diseases: treatment

Содержание
- 2. Introduction Peptic ulcer disease (PUD) is a common disorder that affects millions of individuals worldwide It
- 3. Introduction Major advances have been made in the understanding PUD pathophysiology, particularly the role of Helicobacter
- 4. Definitions Ulcer: A lesion on an epithelial surface (skin or mucous membrane) caused by superficial loss
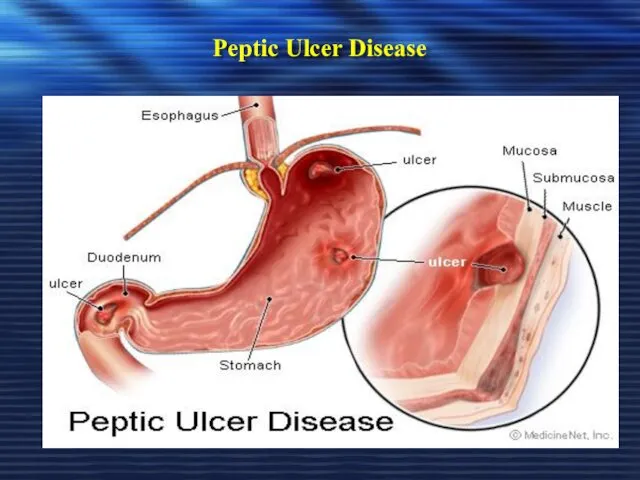
- 5. Definitions Peptic Ulcer An ulcer of the alimentary tract mucosa, usually in the stomach or duodenum,
- 6. Peptic Ulcer Disease
- 7. Gastric Mucosa & Secretions The inside of the stomach is bathed in about 2 liters of
- 8. Gastric Mucosa & Secretions The Defensive Forces Bicarbonate Mucus layer Mucosal blood flow Prostaglandins Growth factors
- 9. Negative Feedback Regulation of Acid Secretion Antral distention Protein content intragastric PH Gastrin release somatostatin secretion
- 10. Pathophysiology A peptic ulcer is a mucosal break, 3 mm or greater in size with depth,
- 11. Pathophysiology Two major variants in peptic ulcers are commonly encountered in the clinical practice: Duodenal Ulcer
- 12. Pathophysiology DU result from increased acid load to the duodenum due to: Increased acid secretion because
- 13. Pathophysiology DU result from increased acid load to the duodenum due to: Smoking impairing gastric mucosal
- 14. Pathophysiology GU results from the break down of gastric mucosa: Associated with gastritis affecting the body
- 15. Etiology The two most common causes of PUD are: Helicobacter pylori infection ( 70-80%) Non-steroidal anti-inflammatory
- 16. Etiology Other uncommon causes include: Gastrinoma (Gastrin secreting tumor) Stress ulceration (trauma, burns, critical illness) Viral
- 17. 1. Etiology – Helicobacter pylori
- 18. H.pylori Epidemiology One half of world’s population has H.pylori infection, with an estimated prevalence of 80-90
- 19. H.pylori as a cause of PUD The majority of PUD patients are H. pylori infected
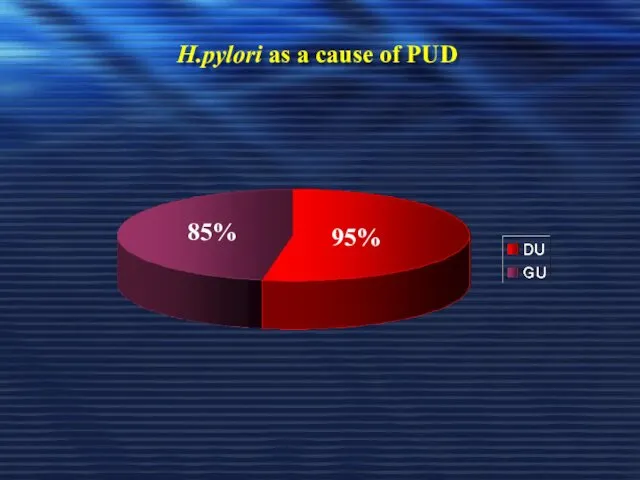
- 20. H.pylori as a cause of PUD 95% 85%
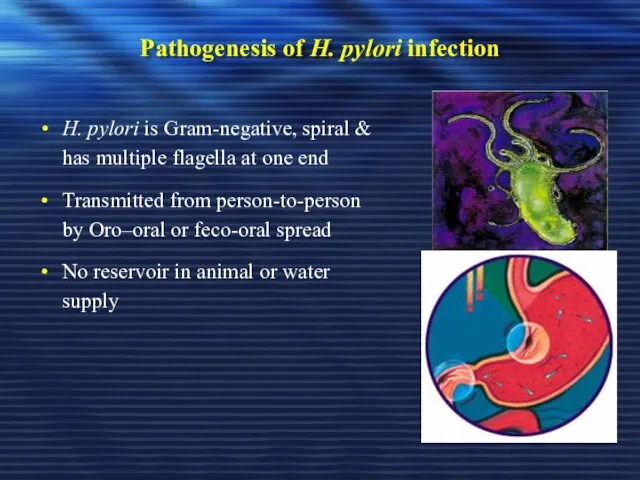
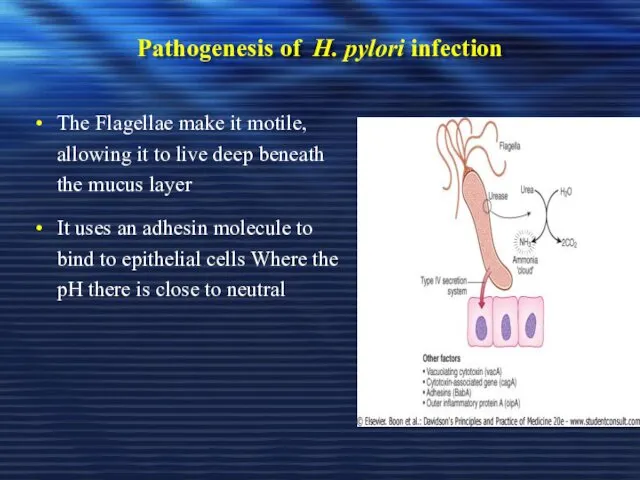
- 21. Pathogenesis of H. pylori infection H. pylori is Gram-negative, spiral & has multiple flagella at one
- 22. Pathogenesis of H. pylori infection The Flagellae make it motile, allowing it to live deep beneath
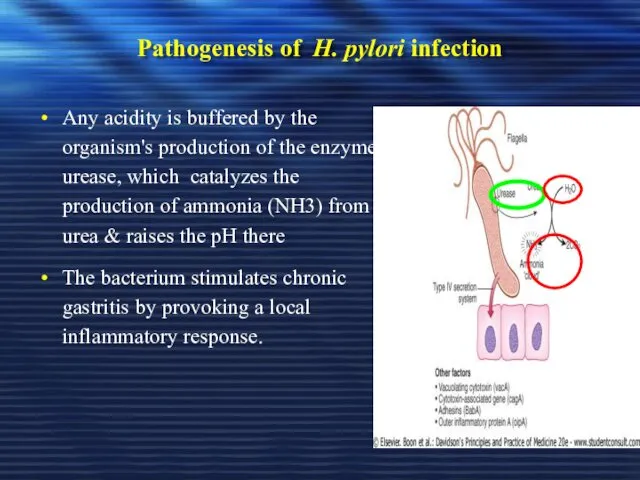
- 23. Pathogenesis of H. pylori infection Any acidity is buffered by the organism's production of the enzyme
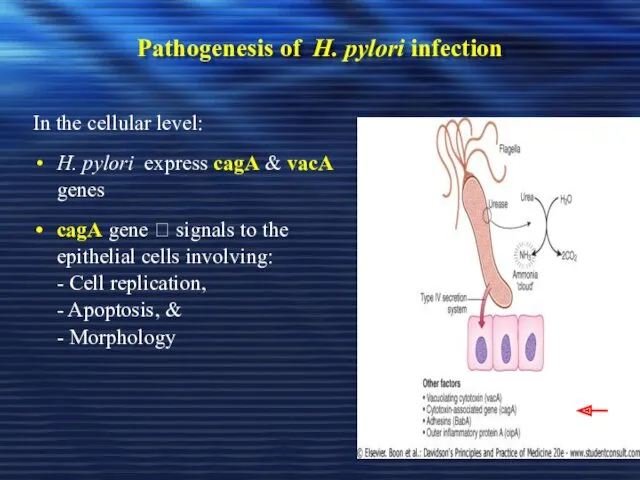
- 24. Pathogenesis of H. pylori infection In the cellular level: H. pylori express cagA & vacA genes
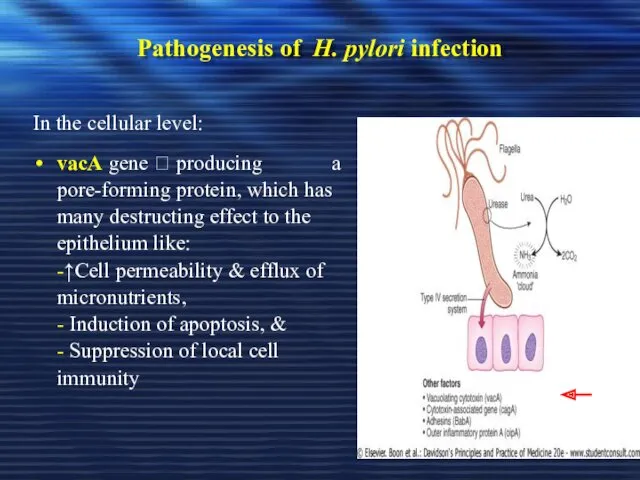
- 25. Pathogenesis of H. pylori infection In the cellular level: vacA gene ? producing a pore-forming protein,
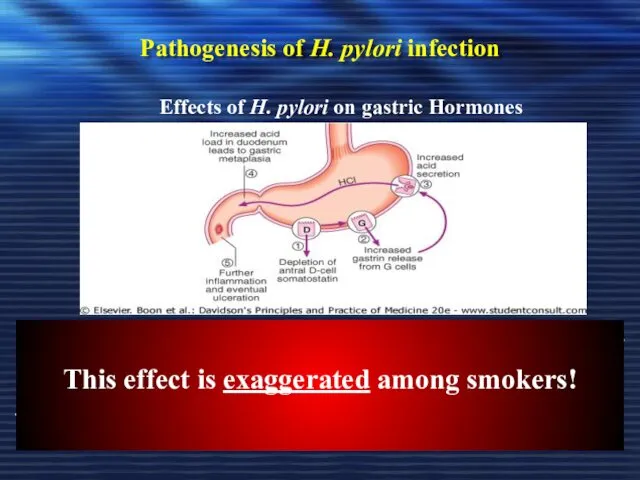
- 26. Pathogenesis of H. pylori infection - ↓ Somatostatin production from antral D-cells due to antral gastritis
- 27. Carcinogenic effect of H. pylori H. pylori Host Factors Other environmental Factors Antral gastritis Pangastritis DU
- 28. Carcinogenic effect of H. pylori Epidemiologic evidence suggests that infection with HP is associated with >2
- 29. For persons at high risk for gastric cancer (e.g., first degree relatives) screening can be considered
- 30. 2. Etiology -Non-Steroidal Anti-inflammatory Drugs (NSAIDS)
- 31. NSAIDS Symptomatic GI ulceration occurs in 2% - 4% of patients treated with NSAIDs for 1
- 32. NSAIDS Inhibits the production of prostaglandins precursor from membrane fatty acids resulting in: 1. Decrease mucus
- 33. NSAIDS Gastric acid probably aggravates NSAID-induce mucosal injury by - Converting superficial injury to deeper mucosal
- 34. NSAIDS Users of NSAIDs are at approximately 3 times greater relative risk of serious adverse gastrointestinal
- 35. NSAIDS Identify risk factors: Age > 65 years (3.5-fold increased risk) Smoking Previous history of GI
- 36. Type of NSAID & Risk of Ulcer
- 37. Does H. pylori Influence the Ulcer Risk in NSAID Users?
- 38. Does H. pylori Influence the Ulcer Risk in NSAID Users? Many investigators had attempted to address
- 39. Does H. pylori Influence the Ulcer Risk in NSAID Users? These conflicting results can be largely
- 40. Recommendations for H.pylori Testing & Eradication in NSAID Users 1- Patients who have a history of
- 41. Recommendations for H.pylori Testing & Eradication in NSAID Users 3- Patients who are about to start
- 42. Clinical Presentation Recurrent epigastric pain (the most common symptom) Burning Occurs 1-3 hours after meals Relieved
- 43. Clinical Presentation Nausea, Vomiting Dyspepsia, fatty food intolerance Chest discomfort Anorexia, weight loss especially in GU
- 44. Diagnosis of PUD
- 45. Peptic Ulcer Disease Diagnosis: Diagnosis of ulcer Diagnosis of H. pylori
- 46. Diagnosis of PUD In most patients routine laboratory tests are usually unhelpful Diagnosis of PUD depends
- 47. Doudenal Ulcer on Endoscopy Doudenal Ulcer Normal doudenal bulb
- 48. Gastric Ulcer on Endoscopy Chronic Gastric Ulcers
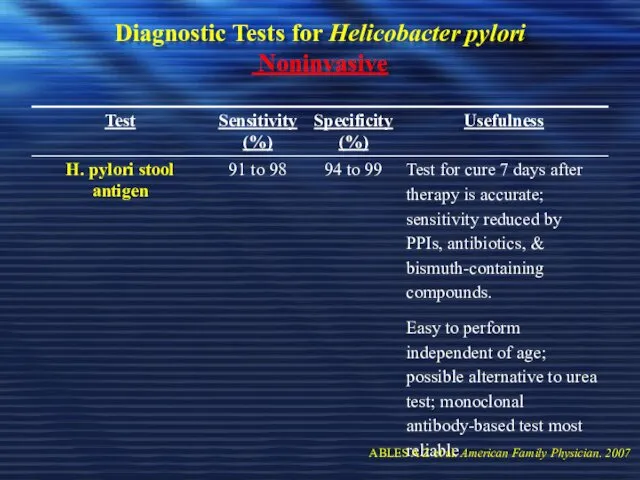
- 49. Diagnosis of H. pylori Non-invasive C13 or C14 Urea Breath Test Stool antigen test H. pylori
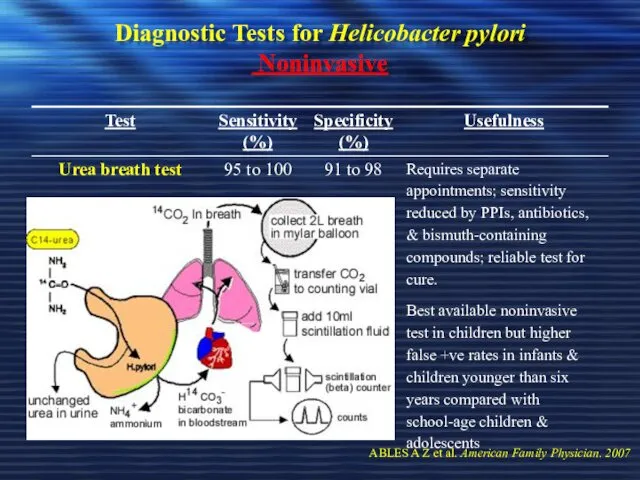
- 50. Diagnosis of H. pylori Non-invasive 1. C13 or C14 Urea Breath Test The best test for
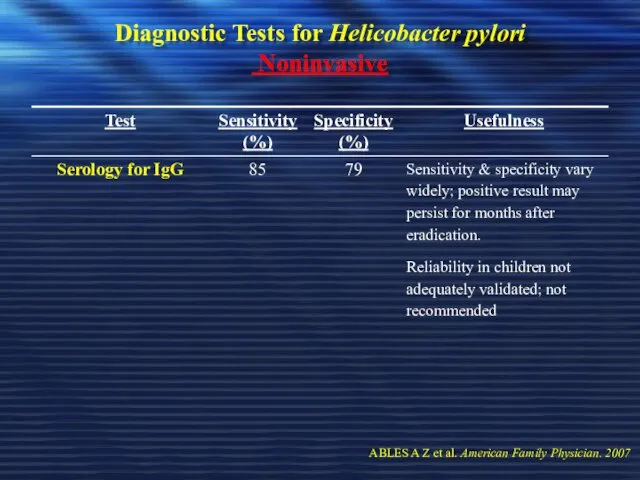
- 51. Diagnosis of H. pylori Non-invasive Serology for H pylori Serum Antibodies (IgG) to H pylori (Not
- 52. Diagnosis of H. pylori Invasive Upper GI endoscopy Highly sensitive test Patient needs sedation Has both
- 53. Diagnosis of H. pylori Invasive (endoscopy) Diagnostic: Detect the site and the size of the ulcer,
- 54. Diagnosis of H. pylori Invasive (endoscopy) Rapid urease test ( RUT) Considered the endoscopic diagnostic test
- 55. Diagnosis of H. pylori Invasive (endoscopy) * Histopathology Done if the rapid urease test result is
- 56. Diagnostic Tests for Helicobacter pylori Invasive ABLES A Z et al. American Family Physician. 2007
- 57. Diagnostic Tests for Helicobacter pylori Noninvasive ABLES A Z et al. American Family Physician. 2007
- 58. Diagnostic Tests for Helicobacter pylori Noninvasive ABLES A Z et al. American Family Physician. 2007
- 59. Diagnostic Tests for Helicobacter pylori Noninvasive ABLES A Z et al. American Family Physician. 2007
- 60. Testing to Document HP Eradication Since treatment is not effective is some cases (> 20%), individuals
- 61. Testing to Document HP Eradication Should be confirmed after end of therapy; noninvasive testing with UBT
- 62. Diagnosis of H. pylori in patients with bleeding PU It is limited by the decreased sensitivity
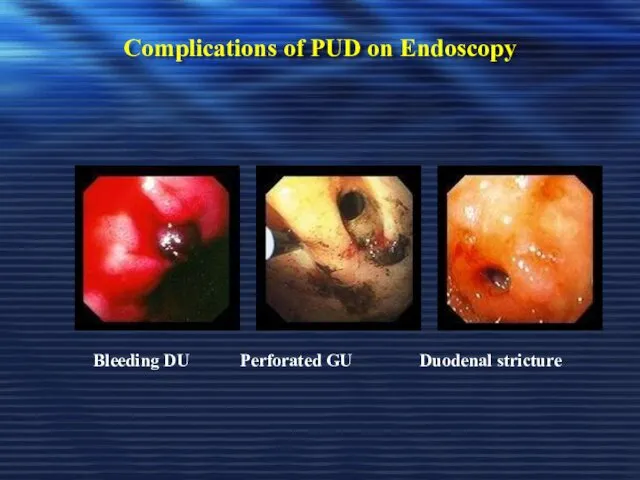
- 63. PUD – Complications Bleeding Perforation Gastric outlet or duodenal obstruction Chronic anemia
- 64. Complications of PUD on Endoscopy Bleeding DU Perforated GU Duodenal stricture
- 65. PUD Treatment
- 66. Treatment Goals Rapid relief of symptoms Healing of ulcer Preventing ulcer recurrences Reducing ulcer-related complications Reduce
- 67. General Strategy Treat complications aggressively if present Determine the etiology of ulcer Discontinue NSAID use if
- 68. General Strategy Smoking cessation should be encouraged If DU is diagnosed by endoscopy, RU testing of
- 69. Drugs Therapy H2-Receptors antagonists Proton pump inhibitors Cyto-protective agents Prostaglandin agonists Antacids Antibiotics for H. pylori
- 70. Management of NSAIDs Ulcers
- 71. Management of NSAIDs Ulcers This can be considered under two headings: The healing of an ulcer
- 72. Healing the Established NSAIDs-Associated Ulcer If possible, NSAID should be stopped, as healing with a histamine
- 73. Best Prevention & Treatment for Upper GI Lesions Induced by NSAIDs There is conclusive evidence that
- 74. The Astronaut Study Ranitidine 150 mg twice daily Vs. Omeprazole 20 or 40 mg daily Gastroduodenal
- 75. Are Better Results Obtained if Additional Inhibition of Gastric Acid Secretion is Achieved? The healing rate
- 76. Reducing Risk of NSAIDs Ulcers by Choice of Agent Choose, where possible, an NSAID from the
- 77. Reducing Risk of NSAIDs Ulcers by Choice of Agent Use highly selective COX-2 inhibitors (whether to
- 78. Reducing Risk of NSAIDs Ulcers by Choice of Agent In low-risk patients such as young -
- 79. Preventing NSAIDs Ulcers with Co-Prescribed Gastric Protectants Patients who continue to require NSAIDs should receive either
- 80. Drugs Therapy for Treatment of PUD 1- H2-Receptors antagonists 2- H+, K+ ATPase: Proton pump inhibitors
- 81. Peptic Ulcer Disease - Treatment
- 82. Degree of Acid Inhibition to Heal an Ulcer It has been reported that a sustained increase
- 83. The Purpose of Inhibiting Gastric Acid Secretion in cases of Upper GI Bleeding In upper GI
- 84. The Ideal Drug to Achieve Potent Acid inhibition Ideal drug should be able to maintain pH
- 85. Drugs Therapy for Treatment of PUD 1- H2-Receptors Antagonists These agents are capable of 90% reduction
- 86. Drugs Therapy for Treatment of PUD 1- H2-Receptors Antagonists Previous recommendations were to administer these agents
- 87. Drugs Therapy for Treatment of PUD 1- H2-Receptors Antagonists Agents Cimetidine 800mg OD or 400mg BID
- 88. Drugs Therapy for Treatment of PUD 1- H2-Receptors Antagonists Pharmacokinetics Rapidly absorbed 1-3 hrs to peak
- 89. Drugs Therapy for Treatment of PUD 1- H2-Receptors Antagonists Side Effects Usually minor; include headache, dizziness,
- 90. Drugs Therapy for Treatment of PUD 1- H2-Receptors Antagonists Drug Interactions Cimetidine slows microsomal metabolism of
- 91. Drugs Therapy for Treatment of PUD 1- H2-Receptors Antagonists Drug Interactions Famotidine & Nizatidine has no
- 92. Drugs Therapy for Treatment of PUD 2- Proton Pump Inhibitors (PPIs) Same Acid Inhibition as Anti-H2??
- 93. Drugs Therapy for Treatment of PUD 2- Proton Pump Inhibitors (PPIs) Same Acid Inhibition as Anti-H2??
- 94. Drugs Therapy for Treatment of PUD 2- Proton Pump Inhibitors (PPIs) Agents Omeprazole Lansoprazole Pantoprazole Rabeprazole
- 95. Drugs Therapy for Treatment of PUD 2- Proton Pump Inhibitors (PPIs) Pharmacological Effect PPIs dose-dependently inhibit
- 96. Drugs Therapy for Treatment of PUD 2- Proton Pump Inhibitors (PPIs) Comparative Anti-secretory Efficacy of the
- 97. Drugs Therapy for Treatment of PUD 2- Proton Pump Inhibitors (PPIs) Side Effects No evidence that
- 98. Drugs Therapy for Treatment of PUD 2- Proton Pump Inhibitors (PPIs) PPIs & Vitamin B12 Deficiency
- 99. Drugs Therapy for Treatment of PUD 2- Proton Pump Inhibitors (PPIs) Time of Administration Should by
- 100. Drugs Therapy for Treatment of PUD 2- Proton Pump Inhibitors (PPIs) Pharmacokinetics How can PPIs have
- 101. Drugs Therapy for Treatment of PUD 2- Proton Pump Inhibitors (PPIs) Pharmacokinetics Metabolism PPIs undergo extensive
- 102. Drugs Therapy for Treatment of PUD 2- Proton Pump Inhibitors (PPIs) Pharmacokinetics What is Esomeprazoie? It
- 103. Drugs Therapy for Treatment of PUD 2- Proton Pump Inhibitors (PPIs) Dose Adjustment in Liver Failure
- 104. Drugs Therapy for Treatment of PUD 2- Proton Pump Inhibitors (PPIs) Drug Interactions Theoretically, their influence
- 105. Drugs Therapy for Treatment of PUD 2- Proton Pump Inhibitors (PPIs) Presence of H. Pylori influence
- 106. Drugs Therapy for Treatment of PUD 2- Proton Pump Inhibitors (PPIs) Do PPIs Have Direct Action
- 107. Drugs Therapy for Treatment of PUD 2- Proton Pump Inhibitors (PPIs) Do PPI Promote Actions of
- 108. Drugs Therapy for Treatment of PUD 3- Cyto-Protective Agent ( Sucalfate) Sucralfate = complex of Aluminum
- 109. Drugs Therapy for Treatment of PUD 3- Cyto-Protective Agent ( Sucalfate) Administration Should not be given
- 110. Drugs Therapy for Treatment of PUD 3- Cyto-Protective Agent ( Sucalfate) Side Effects Constipation; black stool
- 111. Drugs Therapy for Treatment of PUD 4- Prostaglandin Agonists (PGE1) Misoprostol Inhibits secretion of HCl &
- 112. Drugs Therapy for Treatment of PUD 4- Prostaglandin Agonists (PGE1) Misoprostol Optimal role in ulcer treatment
- 113. Drugs Therapy for Treatment of PUD 4- Prostaglandin Agonists (PGE1) Misoprostol Administration Should be given 4
- 114. Drugs Therapy for Treatment of PUD 5- Antacids Weak bases that react with gastric acid to
- 115. Drugs Therapy for Treatment of PUD 5- Antacids Antacids contain either Sodium-bicarbonate, Aluminum-hydroxide, magnesium-hydroxide & calcium
- 116. Drugs Therapy for Treatment of PUD 5- Antacids Very inconvenient to administer Tablet antacids are generally
- 117. Drugs Therapy for Treatment of PUD 5- Antacids Side Effects Cation absorption (sodium, magnesium, aluminum, calcium)
- 118. Drugs Therapy for Treatment of PUD 5- Antacids Side Effects Aluminum hydroxide may be constipating, Magnesium
- 119. The Mechanism & Side Effects of Various Acid Suppressive Medications
- 120. Drugs Therapy for Treatment of PUD 6- Antibiotics for H. Pylori Eradication H. pylori eradication significantly
- 121. To Select Therapy for H. pylori Eradication Duration of treatment & adverse effects should be considered
- 122. Duration of H. Pylori Eradication Therapy Until recently, the recommended duration of therapy for H.pylori eradication
- 123. Adverse Effects The most commonly reported adverse events were nausea, vomiting, & diarrhea A bitter or
- 124. Selected Long-Duration Regimens for H. pylori Eradication ABLES A Z et al. American Family Physician. 2007
- 125. Short-Course Therapy for Eradication of Helicobacter pylori ABLES A Z et al. American Family Physician. 2007
- 126. Short-Course Therapy for Eradication of Helicobacter pylori ABLES A Z et al. American Family Physician. 2007
- 127. Short-Course Therapy for Eradication of Helicobacter pylori ABLES A Z et al. American Family Physician. 2007
- 128. Resistance Resistant H. pylori has been documented in cases of failed eradication therapy based on biopsy
- 129. Resistance Resistance rate to clarithromycin is currently 2-30% & to metronidazole 15-66% Primary resistance to clarithromycin
- 130. Resistance 70 % of patients failing one or more regimens responded well to triple-drug therapy that
- 131. Resistance A meta-analysis of current literature on treatment of resistant H. pylori showed benefit in using
- 132. Recurrence Recurrence of H. pylori infection is defined by: A positive result on urea breath or
- 133. Recurrence Risk factors for recurrence include: Non-ulcer dyspepsia Persistence of chronic gastritis after eradication therapy Female
- 134. Recurrence Recurrence rates worldwide vary but lower in developed countries In the primary care setting, physicians
- 136. Скачать презентацию
Introduction
Peptic ulcer disease (PUD) is a common disorder that affects
Introduction
Peptic ulcer disease (PUD) is a common disorder that affects
Introduction
Major advances have been made in the understanding PUD pathophysiology,
Introduction
Major advances have been made in the understanding PUD pathophysiology,
Definitions
Ulcer:
A lesion on an epithelial surface (skin or mucous membrane) caused
Definitions
Ulcer:
A lesion on an epithelial surface (skin or mucous membrane) caused
Definitions
Peptic Ulcer
An ulcer of the alimentary tract mucosa, usually in the
Definitions
Peptic Ulcer
An ulcer of the alimentary tract mucosa, usually in the
Peptic Ulcer Disease
Peptic Ulcer Disease
Gastric Mucosa & Secretions
The inside of the stomach is bathed in
Gastric Mucosa & Secretions
The inside of the stomach is bathed in
Gastric Mucosa & Secretions
The Defensive Forces
Bicarbonate
Mucus layer
Mucosal blood flow
Prostaglandins
Growth factors
The
Gastric Mucosa & Secretions
The Defensive Forces
Bicarbonate
Mucus layer
Mucosal blood flow
Prostaglandins
Growth factors
The
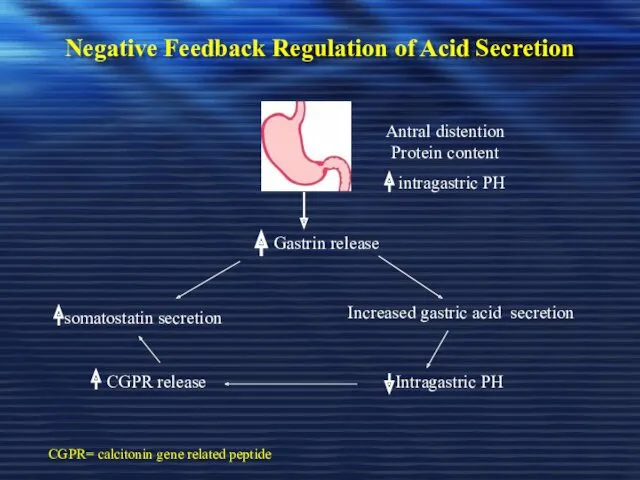
Negative Feedback Regulation of Acid Secretion
Antral distention Protein content
Negative Feedback Regulation of Acid Secretion
Antral distention Protein content
Pathophysiology
A peptic ulcer is a mucosal break, 3 mm or greater
Pathophysiology
A peptic ulcer is a mucosal break, 3 mm or greater
Pathophysiology
Two major variants in peptic ulcers are commonly encountered in the
Pathophysiology
Two major variants in peptic ulcers are commonly encountered in the
Pathophysiology
DU result from increased acid load to the duodenum due to:
Increased
Pathophysiology
DU result from increased acid load to the duodenum due to:
Increased
Pathophysiology
DU result from increased acid load to the duodenum due to:
Smoking
Pathophysiology
DU result from increased acid load to the duodenum due to:
Smoking
Pathophysiology
GU results from the break down of gastric mucosa:
Associated with gastritis
Pathophysiology
GU results from the break down of gastric mucosa:
Associated with gastritis
Etiology
The two most common causes of PUD are:
Helicobacter pylori infection
Etiology
The two most common causes of PUD are:
Helicobacter pylori infection
Etiology
Other uncommon causes include:
Gastrinoma (Gastrin secreting tumor)
Stress ulceration (trauma, burns, critical
Etiology
Other uncommon causes include:
Gastrinoma (Gastrin secreting tumor)
Stress ulceration (trauma, burns, critical
1. Etiology – Helicobacter pylori
1. Etiology – Helicobacter pylori
H.pylori Epidemiology
One half of world’s population has H.pylori infection, with an
H.pylori Epidemiology
One half of world’s population has H.pylori infection, with an
H.pylori as a cause of PUD
The majority of PUD patients
H.pylori as a cause of PUD
The majority of PUD patients
H.pylori as a cause of PUD
95%
85%
H.pylori as a cause of PUD
95%
85%
Pathogenesis of H. pylori infection
H. pylori is Gram-negative, spiral &
Pathogenesis of H. pylori infection
H. pylori is Gram-negative, spiral &
Pathogenesis of H. pylori infection
The Flagellae make it motile, allowing it
Pathogenesis of H. pylori infection
The Flagellae make it motile, allowing it
Pathogenesis of H. pylori infection
Any acidity is buffered by the organism's
Pathogenesis of H. pylori infection
Any acidity is buffered by the organism's
Pathogenesis of H. pylori infection
In the cellular level:
H. pylori express cagA
Pathogenesis of H. pylori infection
In the cellular level:
H. pylori express cagA
Pathogenesis of H. pylori infection
In the cellular level:
vacA gene ? producing
Pathogenesis of H. pylori infection
In the cellular level:
vacA gene ? producing
Pathogenesis of H. pylori infection
- ↓ Somatostatin production from antral D-cells
Pathogenesis of H. pylori infection
- ↓ Somatostatin production from antral D-cells
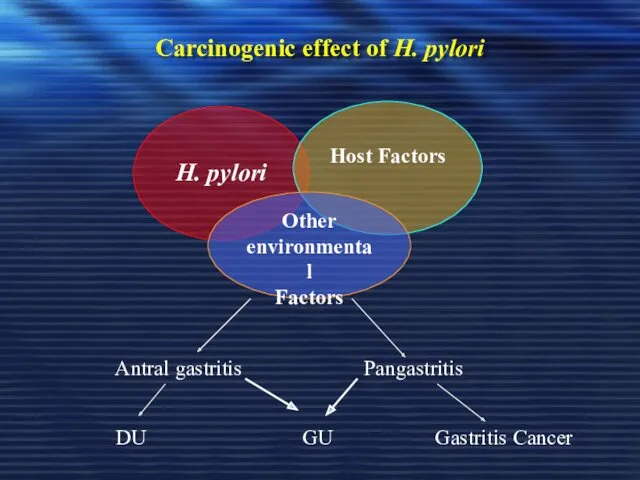
Carcinogenic effect of H. pylori
H. pylori
Host Factors
Other environmental
Factors
Antral
Carcinogenic effect of H. pylori
H. pylori
Host Factors
Other environmental
Factors
Antral
Carcinogenic effect of H. pylori
Epidemiologic evidence suggests that infection with HP
Carcinogenic effect of H. pylori
Epidemiologic evidence suggests that infection with HP
For persons at high risk for gastric cancer (e.g., first degree
For persons at high risk for gastric cancer (e.g., first degree

2. Etiology -Non-Steroidal Anti-inflammatory Drugs (NSAIDS)
2. Etiology -Non-Steroidal Anti-inflammatory Drugs (NSAIDS)
NSAIDS
Symptomatic GI ulceration occurs in 2% - 4% of patients treated
NSAIDS
Symptomatic GI ulceration occurs in 2% - 4% of patients treated
NSAIDS
Inhibits the production of prostaglandins precursor from membrane fatty acids resulting
NSAIDS
Inhibits the production of prostaglandins precursor from membrane fatty acids resulting
NSAIDS
Gastric acid probably aggravates NSAID-induce mucosal injury by
- Converting
NSAIDS
Gastric acid probably aggravates NSAID-induce mucosal injury by
- Converting
NSAIDS
Users of NSAIDs are at approximately 3 times greater relative risk
NSAIDS
Users of NSAIDs are at approximately 3 times greater relative risk
NSAIDS
Identify risk factors:
Age > 65 years (3.5-fold increased
NSAIDS
Identify risk factors:
Age > 65 years (3.5-fold increased
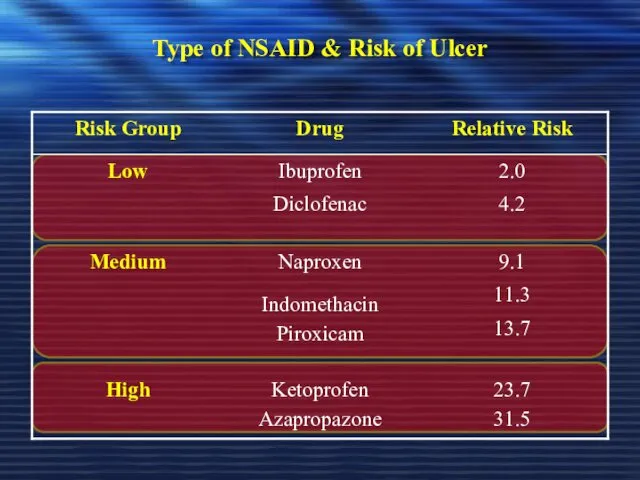
Type of NSAID & Risk of Ulcer
Type of NSAID & Risk of Ulcer
Does H. pylori Influence the Ulcer Risk in NSAID Users?
Does H. pylori Influence the Ulcer Risk in NSAID Users?
Many investigators
Does H. pylori Influence the Ulcer Risk in NSAID Users?
Many investigators
Does H. pylori Influence the Ulcer Risk in NSAID Users?
These conflicting
Does H. pylori Influence the Ulcer Risk in NSAID Users?
These conflicting
Recommendations for H.pylori Testing & Eradication in NSAID Users
1- Patients who
Recommendations for H.pylori Testing & Eradication in NSAID Users
1- Patients who
Recommendations for H.pylori Testing & Eradication in NSAID Users
3- Patients who
Recommendations for H.pylori Testing & Eradication in NSAID Users
3- Patients who
Clinical Presentation
Recurrent epigastric pain (the most common symptom)
Burning
Occurs 1-3 hours after
Clinical Presentation
Recurrent epigastric pain (the most common symptom)
Burning
Occurs 1-3 hours after
Clinical Presentation
Nausea, Vomiting
Dyspepsia, fatty food intolerance
Chest discomfort
Anorexia, weight loss especially in
Clinical Presentation
Nausea, Vomiting
Dyspepsia, fatty food intolerance
Chest discomfort
Anorexia, weight loss especially in
Diagnosis of PUD
Diagnosis of PUD
Peptic Ulcer Disease
Diagnosis:
Diagnosis of ulcer
Diagnosis of H. pylori
Peptic Ulcer Disease
Diagnosis:
Diagnosis of ulcer
Diagnosis of H. pylori
Diagnosis of PUD
In most patients routine laboratory tests are usually
Diagnosis of PUD
In most patients routine laboratory tests are usually
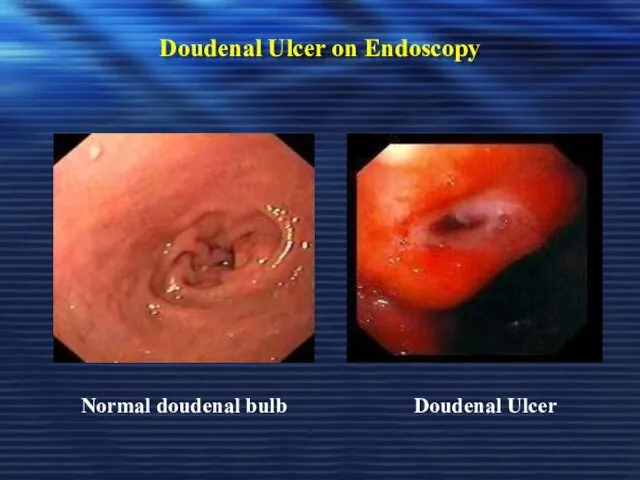
Doudenal Ulcer on Endoscopy
Doudenal Ulcer
Normal doudenal bulb
Doudenal Ulcer on Endoscopy
Doudenal Ulcer
Normal doudenal bulb
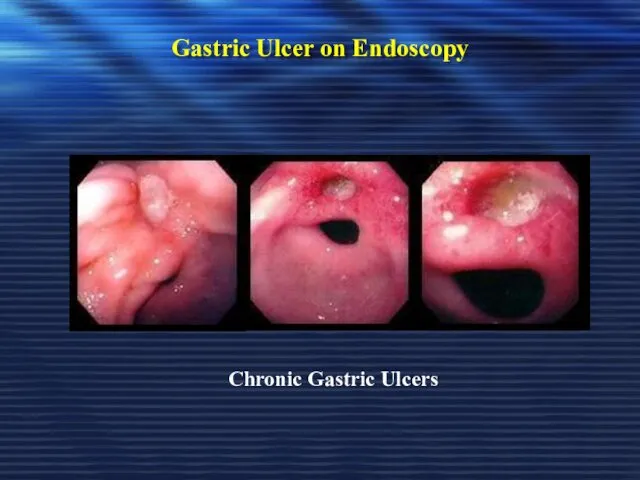
Gastric Ulcer on Endoscopy
Chronic Gastric Ulcers
Gastric Ulcer on Endoscopy
Chronic Gastric Ulcers
Diagnosis of H. pylori
Non-invasive
C13 or C14 Urea Breath Test
Stool antigen test
H.
Diagnosis of H. pylori
Non-invasive
C13 or C14 Urea Breath Test
Stool antigen test
H.
Diagnosis of H. pylori
Non-invasive
1. C13 or C14 Urea Breath
Diagnosis of H. pylori
Non-invasive
1. C13 or C14 Urea Breath
Diagnosis of H. pylori
Non-invasive
Serology for H pylori
Serum Antibodies (IgG) to
Diagnosis of H. pylori
Non-invasive
Serology for H pylori
Serum Antibodies (IgG) to
Diagnosis of H. pylori
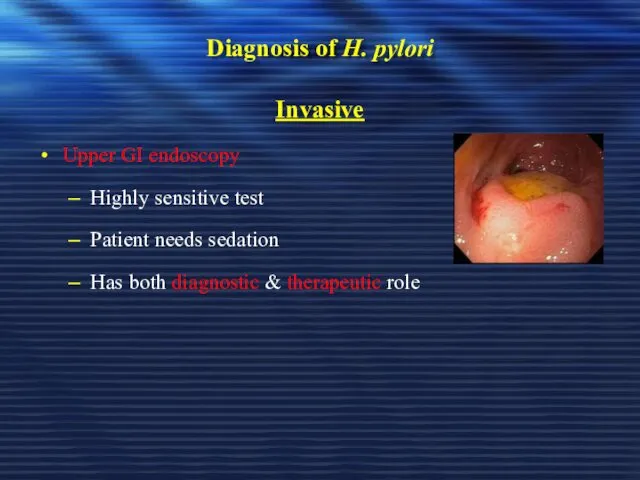
Invasive
Upper GI endoscopy
Highly sensitive test
Patient needs sedation
Has both
Diagnosis of H. pylori
Invasive
Upper GI endoscopy
Highly sensitive test
Patient needs sedation
Has both

Diagnosis of H. pylori
Invasive (endoscopy)
Diagnostic:
Detect the site and the size of
Diagnosis of H. pylori
Invasive (endoscopy)
Diagnostic:
Detect the site and the size of
Diagnosis of H. pylori
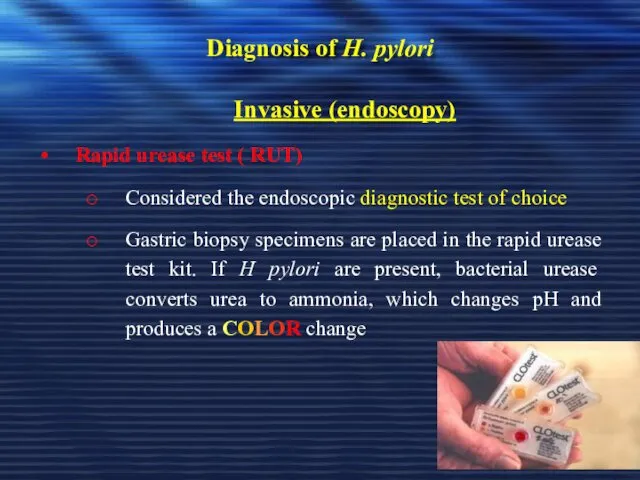
Invasive (endoscopy)
Rapid urease test ( RUT)
Considered the endoscopic
Diagnosis of H. pylori
Invasive (endoscopy)
Rapid urease test ( RUT)
Considered the endoscopic
Diagnosis of H. pylori
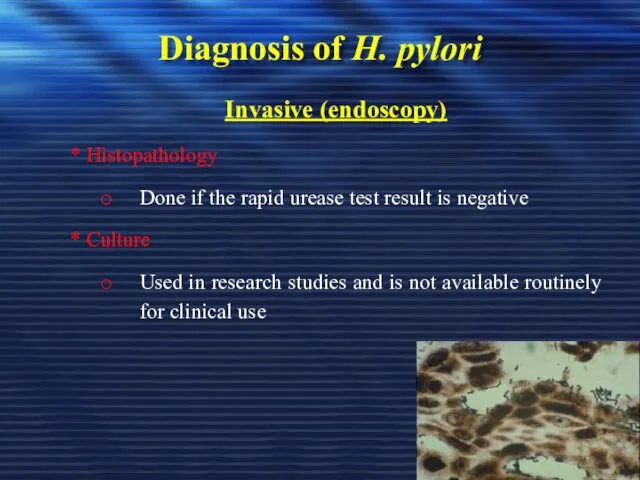
Invasive (endoscopy)
* Histopathology
Done if the rapid urease test
Diagnosis of H. pylori
Invasive (endoscopy)
* Histopathology
Done if the rapid urease test
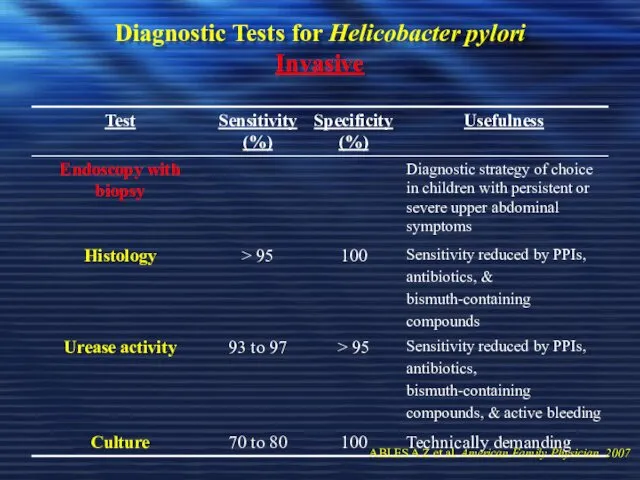
Diagnostic Tests for Helicobacter pylori
Invasive
ABLES A Z et al.
Diagnostic Tests for Helicobacter pylori
Invasive
ABLES A Z et al.
Diagnostic Tests for Helicobacter pylori
Noninvasive
ABLES A Z et
Diagnostic Tests for Helicobacter pylori
Noninvasive
ABLES A Z et
Diagnostic Tests for Helicobacter pylori
Noninvasive
ABLES A Z et
Diagnostic Tests for Helicobacter pylori
Noninvasive
ABLES A Z et
Diagnostic Tests for Helicobacter pylori
Noninvasive
ABLES A Z et
Diagnostic Tests for Helicobacter pylori
Noninvasive
ABLES A Z et
Testing to Document HP Eradication
Since treatment is not effective is some
Testing to Document HP Eradication
Since treatment is not effective is some
Testing to Document HP Eradication
Should be confirmed after end of therapy;
Testing to Document HP Eradication
Should be confirmed after end of therapy;
Diagnosis of H. pylori in patients with bleeding PU
It is limited
Diagnosis of H. pylori in patients with bleeding PU
It is limited
PUD – Complications
Bleeding
Perforation
Gastric outlet or duodenal obstruction
Chronic anemia
PUD – Complications
Bleeding
Perforation
Gastric outlet or duodenal obstruction
Chronic anemia
Complications of PUD on Endoscopy
Bleeding DU Perforated GU Duodenal stricture
Complications of PUD on Endoscopy
Bleeding DU Perforated GU Duodenal stricture
PUD Treatment
Treatment Goals
Rapid relief of symptoms
Healing of ulcer
Preventing ulcer recurrences
Reducing ulcer-related
Treatment Goals
Rapid relief of symptoms
Healing of ulcer
Preventing ulcer recurrences
Reducing ulcer-related
General Strategy
Treat complications aggressively if present
Determine the etiology of ulcer
Discontinue
General Strategy
Treat complications aggressively if present
Determine the etiology of ulcer
Discontinue
General Strategy
Smoking cessation should be encouraged
If DU is diagnosed by
General Strategy
Smoking cessation should be encouraged
If DU is diagnosed by
Drugs Therapy
H2-Receptors antagonists
Proton pump inhibitors
Cyto-protective agents
Prostaglandin agonists
Antacids
Antibiotics for
Drugs Therapy
H2-Receptors antagonists
Proton pump inhibitors
Cyto-protective agents
Prostaglandin agonists
Antacids
Antibiotics for
Management of NSAIDs Ulcers
Management of NSAIDs Ulcers
This can be considered under two headings:
The
Management of NSAIDs Ulcers
This can be considered under two headings:
The
Healing the Established NSAIDs-Associated Ulcer
If possible, NSAID should be stopped, as
Healing the Established NSAIDs-Associated Ulcer
If possible, NSAID should be stopped, as
Best Prevention & Treatment for Upper GI Lesions Induced by NSAIDs
There
Best Prevention & Treatment for Upper GI Lesions Induced by NSAIDs
There
The Astronaut Study
Ranitidine 150 mg twice daily Vs. Omeprazole 20 or
The Astronaut Study
Ranitidine 150 mg twice daily Vs. Omeprazole 20 or
Are Better Results Obtained if Additional Inhibition of Gastric Acid Secretion
Are Better Results Obtained if Additional Inhibition of Gastric Acid Secretion
Reducing Risk of NSAIDs Ulcers by Choice of Agent
Choose, where possible,
Reducing Risk of NSAIDs Ulcers by Choice of Agent
Choose, where possible,
Reducing Risk of NSAIDs Ulcers by Choice of Agent
Use highly selective
Reducing Risk of NSAIDs Ulcers by Choice of Agent
Use highly selective
Reducing Risk of NSAIDs Ulcers by Choice of Agent
In low-risk patients
Reducing Risk of NSAIDs Ulcers by Choice of Agent
In low-risk patients
Preventing NSAIDs Ulcers with Co-Prescribed Gastric Protectants
Patients who continue to require
Preventing NSAIDs Ulcers with Co-Prescribed Gastric Protectants
Patients who continue to require
Drugs Therapy for Treatment of PUD
1- H2-Receptors antagonists
2- H+, K+
Drugs Therapy for Treatment of PUD
1- H2-Receptors antagonists
2- H+, K+
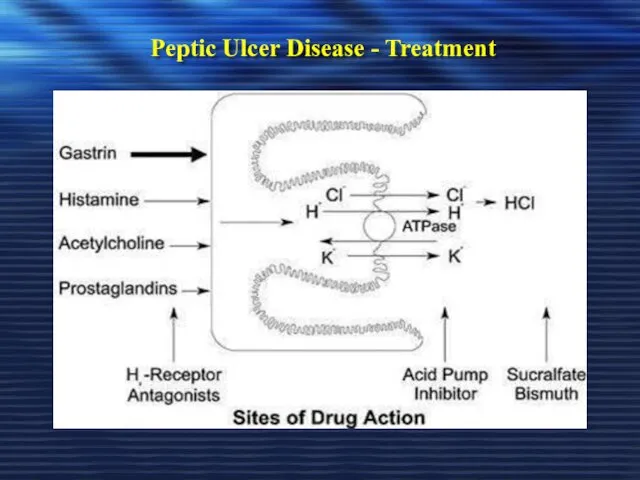
Peptic Ulcer Disease - Treatment
Peptic Ulcer Disease - Treatment
Degree of Acid Inhibition to Heal an Ulcer
It has been reported
Degree of Acid Inhibition to Heal an Ulcer
It has been reported
The Purpose of Inhibiting Gastric Acid Secretion in cases of Upper
The Purpose of Inhibiting Gastric Acid Secretion in cases of Upper
The Ideal Drug to Achieve Potent Acid inhibition
Ideal drug should be
The Ideal Drug to Achieve Potent Acid inhibition
Ideal drug should be
Drugs Therapy for Treatment of PUD
1- H2-Receptors Antagonists
These agents are capable
Drugs Therapy for Treatment of PUD
1- H2-Receptors Antagonists
These agents are capable
Drugs Therapy for Treatment of PUD
1- H2-Receptors Antagonists
Previous recommendations were to
Drugs Therapy for Treatment of PUD
1- H2-Receptors Antagonists
Previous recommendations were to
Drugs Therapy for Treatment of PUD
1- H2-Receptors Antagonists
Agents
Cimetidine 800mg OD or
Drugs Therapy for Treatment of PUD
1- H2-Receptors Antagonists
Agents
Cimetidine 800mg OD or
Drugs Therapy for Treatment of PUD
1- H2-Receptors Antagonists
Pharmacokinetics
Rapidly absorbed 1-3 hrs
Drugs Therapy for Treatment of PUD
1- H2-Receptors Antagonists
Pharmacokinetics
Rapidly absorbed 1-3 hrs
Drugs Therapy for Treatment of PUD
1- H2-Receptors Antagonists
Side Effects
Usually minor; include
Drugs Therapy for Treatment of PUD
1- H2-Receptors Antagonists
Side Effects
Usually minor; include
Drugs Therapy for Treatment of PUD
1- H2-Receptors Antagonists
Drug Interactions
Cimetidine slows microsomal
Drugs Therapy for Treatment of PUD
1- H2-Receptors Antagonists
Drug Interactions
Cimetidine slows microsomal
Drugs Therapy for Treatment of PUD
1- H2-Receptors Antagonists
Drug Interactions
Famotidine & Nizatidine
Drugs Therapy for Treatment of PUD
1- H2-Receptors Antagonists
Drug Interactions
Famotidine & Nizatidine
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Same Acid
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Same Acid
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Same Acid
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Same Acid
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Agents
Omeprazole
Lansoprazole
Pantoprazole
Rabeprazole
Esomeprazole
1st
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Agents
Omeprazole
Lansoprazole
Pantoprazole
Rabeprazole
Esomeprazole
1st
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Pharmacological Effect
PPIs
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Pharmacological Effect
PPIs
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Comparative Anti-secretory
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Comparative Anti-secretory
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Side Effects
No
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Side Effects
No
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
PPIs &
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
PPIs &
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Time of
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Time of
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Pharmacokinetics
How can
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Pharmacokinetics
How can
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Pharmacokinetics
Metabolism
PPIs undergo
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Pharmacokinetics
Metabolism
PPIs undergo
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Pharmacokinetics
What is
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Pharmacokinetics
What is
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Dose Adjustment
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Dose Adjustment
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Drug Interactions
Theoretically,
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Drug Interactions
Theoretically,
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Presence of
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Presence of
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Do PPIs
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Do PPIs
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Do PPI
Drugs Therapy for Treatment of PUD
2- Proton Pump Inhibitors (PPIs)
Do PPI
Drugs Therapy for Treatment of PUD
3- Cyto-Protective Agent ( Sucalfate)
Sucralfate =
Drugs Therapy for Treatment of PUD
3- Cyto-Protective Agent ( Sucalfate)
Sucralfate =
Drugs Therapy for Treatment of PUD
3- Cyto-Protective Agent ( Sucalfate)
Administration
Should not
Drugs Therapy for Treatment of PUD
3- Cyto-Protective Agent ( Sucalfate)
Administration
Should not
Drugs Therapy for Treatment of PUD
3- Cyto-Protective Agent ( Sucalfate)
Side Effects
Constipation;
Drugs Therapy for Treatment of PUD
3- Cyto-Protective Agent ( Sucalfate)
Side Effects
Constipation;
Drugs Therapy for Treatment of PUD
4- Prostaglandin Agonists (PGE1) Misoprostol
Inhibits secretion
Drugs Therapy for Treatment of PUD
4- Prostaglandin Agonists (PGE1) Misoprostol
Inhibits secretion
Drugs Therapy for Treatment of PUD
4- Prostaglandin Agonists (PGE1) Misoprostol
Optimal role
Drugs Therapy for Treatment of PUD
4- Prostaglandin Agonists (PGE1) Misoprostol
Optimal role
Drugs Therapy for Treatment of PUD
4- Prostaglandin Agonists (PGE1) Misoprostol
Administration
Should be
Drugs Therapy for Treatment of PUD
4- Prostaglandin Agonists (PGE1) Misoprostol
Administration
Should be
Drugs Therapy for Treatment of PUD
5- Antacids
Weak bases that react with
Drugs Therapy for Treatment of PUD
5- Antacids
Weak bases that react with
Drugs Therapy for Treatment of PUD
5- Antacids
Antacids contain either Sodium-bicarbonate, Aluminum-hydroxide,
Drugs Therapy for Treatment of PUD
5- Antacids
Antacids contain either Sodium-bicarbonate, Aluminum-hydroxide,
Drugs Therapy for Treatment of PUD
5- Antacids
Very inconvenient to administer
Tablet antacids
Drugs Therapy for Treatment of PUD
5- Antacids
Very inconvenient to administer
Tablet antacids
Drugs Therapy for Treatment of PUD
5- Antacids
Side Effects
Cation absorption (sodium, magnesium,
Drugs Therapy for Treatment of PUD
5- Antacids
Side Effects
Cation absorption (sodium, magnesium,
Drugs Therapy for Treatment of PUD
5- Antacids
Side Effects
Aluminum hydroxide may be
Drugs Therapy for Treatment of PUD
5- Antacids
Side Effects
Aluminum hydroxide may be
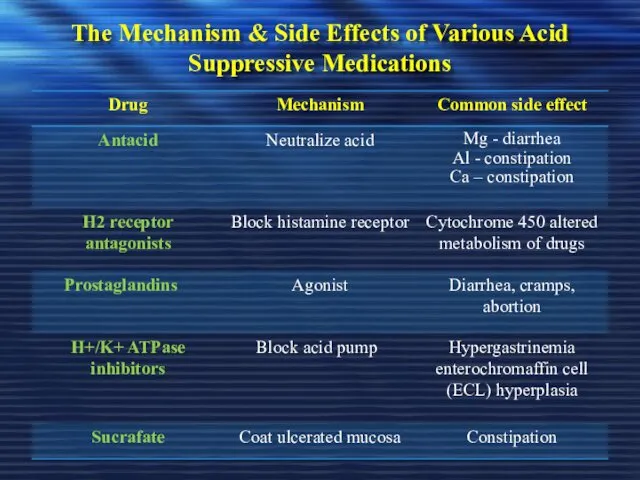
The Mechanism & Side Effects of Various Acid Suppressive Medications
The Mechanism & Side Effects of Various Acid Suppressive Medications
Drugs Therapy for Treatment of PUD
6- Antibiotics for H. Pylori Eradication
Drugs Therapy for Treatment of PUD
6- Antibiotics for H. Pylori Eradication
To Select Therapy for H. pylori Eradication
Duration of treatment &
To Select Therapy for H. pylori Eradication
Duration of treatment &
Duration of H. Pylori Eradication Therapy
Until recently, the recommended duration
Duration of H. Pylori Eradication Therapy
Until recently, the recommended duration
Adverse Effects
The most commonly reported adverse events were nausea, vomiting,
Adverse Effects
The most commonly reported adverse events were nausea, vomiting,
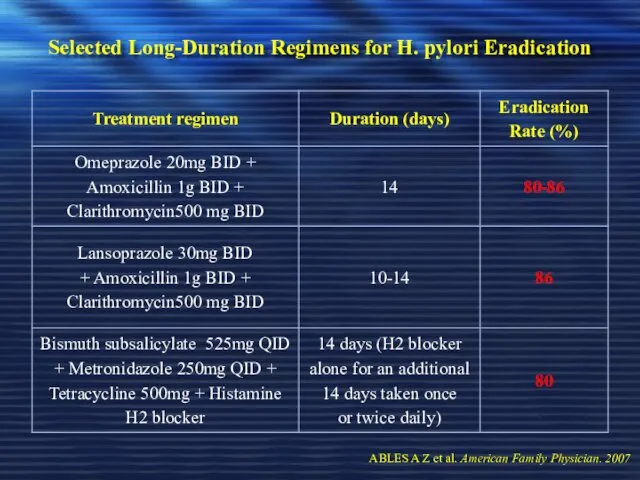
Selected Long-Duration Regimens for H. pylori Eradication
ABLES A Z et
Selected Long-Duration Regimens for H. pylori Eradication
ABLES A Z et
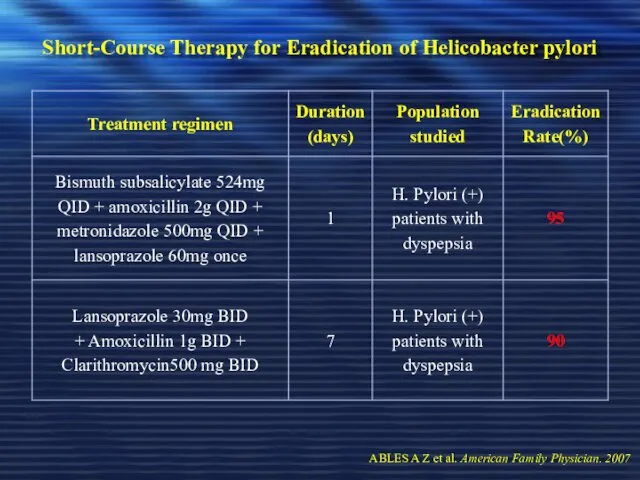
Short-Course Therapy for Eradication of Helicobacter pylori
ABLES A Z et
Short-Course Therapy for Eradication of Helicobacter pylori
ABLES A Z et
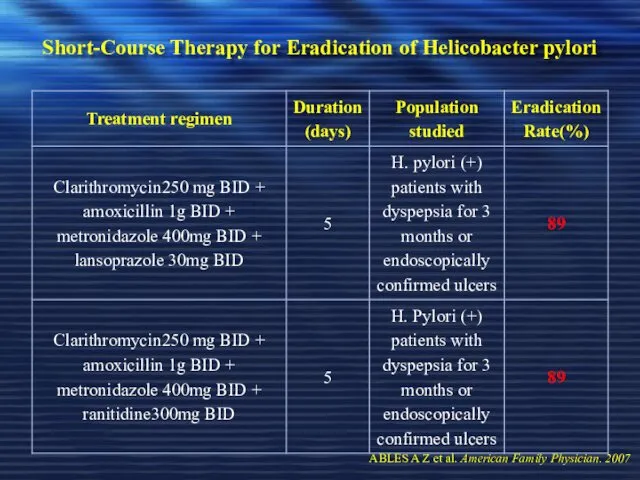
Short-Course Therapy for Eradication of Helicobacter pylori
ABLES A Z et
Short-Course Therapy for Eradication of Helicobacter pylori
ABLES A Z et
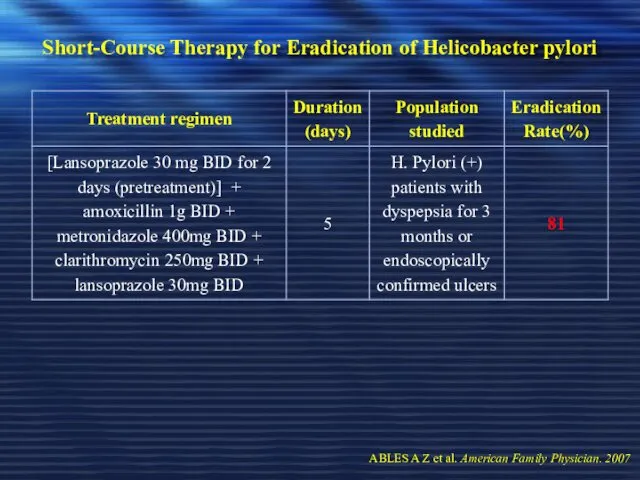
Short-Course Therapy for Eradication of Helicobacter pylori
ABLES A Z et
Short-Course Therapy for Eradication of Helicobacter pylori
ABLES A Z et
Resistance
Resistant H. pylori has been documented in cases of failed
Resistance
Resistant H. pylori has been documented in cases of failed
Resistance
Resistance rate to clarithromycin is currently 2-30% & to metronidazole
Resistance
Resistance rate to clarithromycin is currently 2-30% & to metronidazole
Resistance
70 % of patients failing one or more regimens responded
Resistance
70 % of patients failing one or more regimens responded
Resistance
A meta-analysis of current literature on treatment of resistant H.
Resistance
A meta-analysis of current literature on treatment of resistant H.
Recurrence
Recurrence of H. pylori infection is defined by:
A positive
Recurrence
Recurrence of H. pylori infection is defined by:
A positive
Recurrence
Risk factors for recurrence include:
Non-ulcer dyspepsia
Persistence of chronic gastritis after
Recurrence
Risk factors for recurrence include:
Non-ulcer dyspepsia
Persistence of chronic gastritis after
Recurrence
Recurrence rates worldwide vary but lower in developed countries
In the
Recurrence
Recurrence rates worldwide vary but lower in developed countries
In the
 Желтухи новорождённых
Желтухи новорождённых Methods of examination in gynecology
Methods of examination in gynecology Кодекс Республики Казахстан О здоровье народа и системе здравоохранения. Статьи Кодекса о профилактике инфекционных болезней
Кодекс Республики Казахстан О здоровье народа и системе здравоохранения. Статьи Кодекса о профилактике инфекционных болезней Оказание неотложной помощи детям
Оказание неотложной помощи детям Мочевыделительная система
Мочевыделительная система Инфузионная терапия и парентеральное питание
Инфузионная терапия и парентеральное питание Химические реакции с участием макромолекул
Химические реакции с участием макромолекул Кешенді медициналық ақпараттық жүйе (КМИС)
Кешенді медициналық ақпараттық жүйе (КМИС) Повреждения при выстреле из дробового оружия. Определение дистанции выстрела
Повреждения при выстреле из дробового оружия. Определение дистанции выстрела Вибрациялық аурулар. Профилактикасының принціптері
Вибрациялық аурулар. Профилактикасының принціптері Дезинфекция. Методы дезинфекции
Дезинфекция. Методы дезинфекции Лимфа айналысы. Морфологиялық және функциональдық ерекшеліктері
Лимфа айналысы. Морфологиялық және функциональдық ерекшеліктері Қазақ халық медицинасы
Қазақ халық медицинасы Проблемы наркомании и алкоголизма в России
Проблемы наркомании и алкоголизма в России Общие принципы диагностики и лечения профессиональных заболеваний
Общие принципы диагностики и лечения профессиональных заболеваний Дифференциальная диагностика суставного синдрома
Дифференциальная диагностика суставного синдрома Заболевания ЖКТ
Заболевания ЖКТ Основы конструирования ортодонтических аппаратов
Основы конструирования ортодонтических аппаратов Гестационный пиелонефрит
Гестационный пиелонефрит Сбалансированная инфузионная терапия при тяжелых огнестрельных ранениях
Сбалансированная инфузионная терапия при тяжелых огнестрельных ранениях Классификация, мониторирование, лечение бронхиальной астмы у детей
Классификация, мониторирование, лечение бронхиальной астмы у детей ҰлпАның қабынбалы аурулары
ҰлпАның қабынбалы аурулары Қызыл жалпақ теміреткі. Жүйелі қызыл жегі. Күлдіреуікше. Ауыз қуысындағы көрінісі
Қызыл жалпақ теміреткі. Жүйелі қызыл жегі. Күлдіреуікше. Ауыз қуысындағы көрінісі Аномалии родовой деятельности. Классификация аномалий сократительной деятельности матки
Аномалии родовой деятельности. Классификация аномалий сократительной деятельности матки Предмет и задачи медтоксикологии
Предмет и задачи медтоксикологии Haemolytic disease of the fetus and newborn. Rh isoimmunization
Haemolytic disease of the fetus and newborn. Rh isoimmunization Тромботический синдром
Тромботический синдром Методы лечения аномалий прикуса в периоде смешанных зубах
Методы лечения аномалий прикуса в периоде смешанных зубах