- Pleural Effusions and Pneumothorax

Содержание
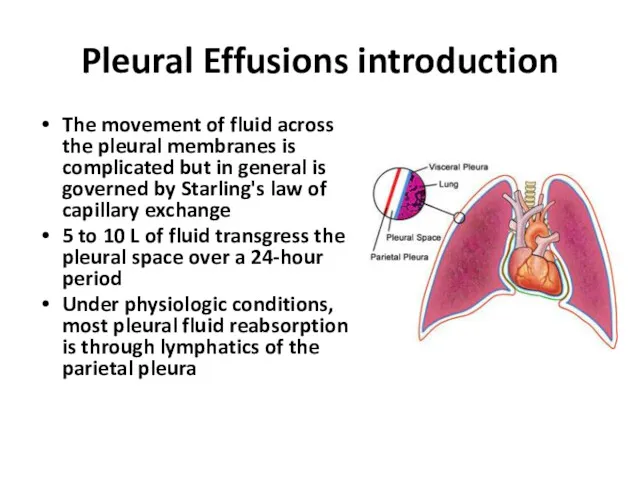
- 2. Pleural Effusions introduction The movement of fluid across the pleural membranes is complicated but in general
- 3. Pleural Effusions introduction imbalance of accumulation and absorption of pleural fluid will lead to the development
- 4. Pleural Effusions introduction About 300 mL of fluid is required for the development of costophrenic angle
- 5. Transudative Vs. Exudative Effusions Criteria: 1. Pleural fluid protein/serum protein greater than 0.5 2. Pleural fluid
- 6. Diagnostic Approach The leading causes of transudative pleural effusions in the United States are left-ventricular failure
- 7. Pleural fluid analysis Gross appearance (pus- Empyema, black- Aspergillus, green- Biliothorax, white- Chylothorax) Very high LDH-
- 9. Effusion Due to Heart Failure A diagnostic thoracentesis should be performed if the effusions are not
- 10. Hepatic Hydrothorax Pleural effusions occur in ~5% of patients with cirrhosis and ascites effusion is usually
- 11. Parapneumonic Effusion Parapneumonic effusions are associated with bacterial pneumonia, lung abscess, or bronchiectasis and are probably
- 12. Parapneumonic Effusion Patients with aerobic bacterial pneumonia and pleural effusion present with an acute febrile illness
- 13. Uncomplicated Vs. Complicated parapneumonic effusion An uncomplicated parapneumonic effusion has "exudative" chemistries, normal pH and glucose,
- 14. Indication for pleural drainage Loculated pleural fluid Pleural fluid pH Pleural fluid glucose Positive Gram stain
- 15. Before and after driange
- 16. Treatment of parapneumonic effusion An empiric, broad spectrum antibiotic that includes coverage for anaerobic organisms In
- 17. Effusion Secondary to Malignancy Malignant pleural effusions secondary to metastatic disease are the second most common
- 18. Effusion Secondary to Malignancy The diagnosis usually is made via cytology of the pleural fluid If
- 19. Treatment of Malignant pleural effusion If the patient's lifestyle is compromised by dyspnea and if the
- 20. Pneumothorax introduction Pneumothorax is the accumulation of air within the pleural space Pneumothorax can be spontaneous
- 21. Pneumothorax introduction Patients with pneumothorax most commonly present with chest pain (sharp and pleuritic) and dyspnea
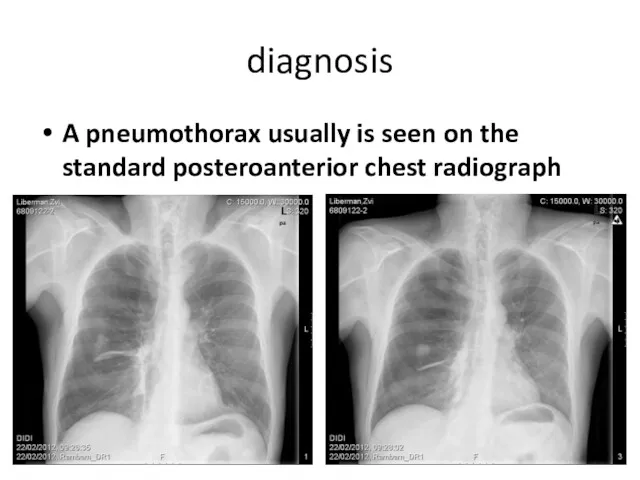
- 22. diagnosis A pneumothorax usually is seen on the standard posteroanterior chest radiograph
- 23. Hydropneumothorax
- 24. Classifications of Pneumothorax Spontaneous Primary Secondary Traumatic Iatrogenic Esophageal perforation
- 25. primary spontaneous pneumothorax A primary spontaneous pneumothorax occurs in the absence of underlying lung disease Patients
- 26. Treatment of primary spontaneous pneumothorax Small pneumothoraces ( Indications for intervention include progressive pneumothorax, delayed pulmonary
- 27. Treatment of primary spontaneous pneumothorax Moderate (20%-40%) and large (>40%) pneumothoraces nearly always are associated with
- 28. Treatment of primary spontaneous pneumothorax Complications of chest tube insertion for pneumothorax are infrequent but include
- 29. Indication for Surgical intervention in spontaneous pneumothorax Air leak that persist for more than 72 hours
- 30. Surgical intervention for spontaneous pneumothorax Apical blebs are resected. The parietal pleura over the apex of
- 31. Secondary spontaneous pneumothorax Most secondary pneumothoraxes are due to chronic obstructive pulmonary disease Pneumothorax in patients
- 32. Preventing recurrence smoking cessation VATS pleurodesis- The rate of recurrent pneumothorax is less than 5 percent
- 33. Traumatic pneumothoraxes Traumatic pneumothoraxes can result from both penetrating and blunt chest trauma Some times when
- 34. Traumatic pneumothoraxes
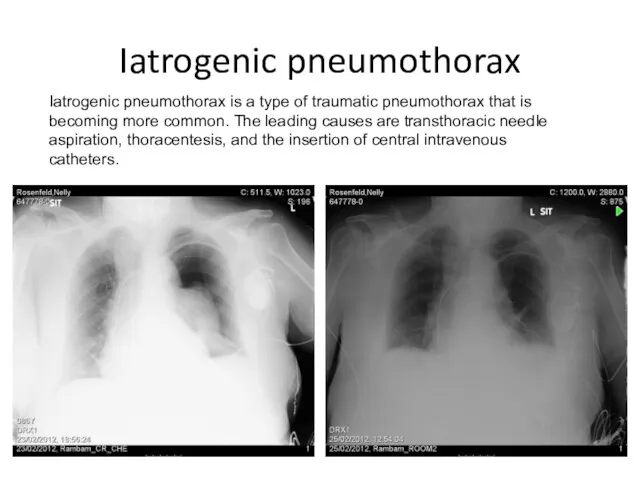
- 35. Iatrogenic pneumothorax Iatrogenic pneumothorax is a type of traumatic pneumothorax that is becoming more common. The
- 36. tension pneumothorax hemodynamic collapse (decreased venous return to the heart and reduced cardiac output) severe respiratory
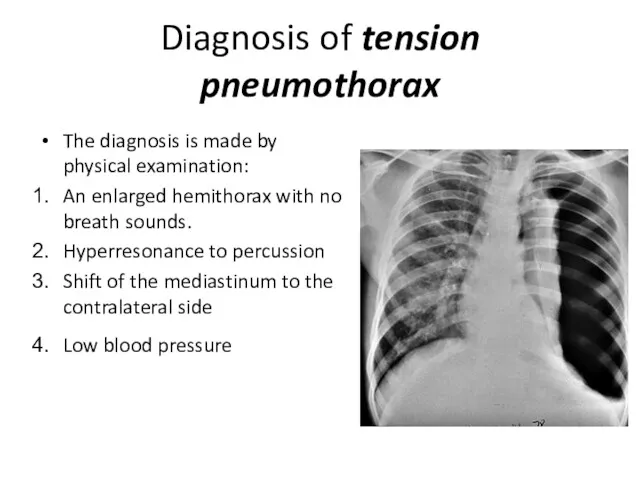
- 37. Diagnosis of tension pneumothorax The diagnosis is made by physical examination: An enlarged hemithorax with no
- 39. Скачать презентацию
Pleural Effusions introduction
The movement of fluid across the pleural membranes is
Pleural Effusions introduction
The movement of fluid across the pleural membranes is
Pleural Effusions introduction
imbalance of accumulation and absorption of pleural fluid will
Pleural Effusions introduction
imbalance of accumulation and absorption of pleural fluid will
Pleural Effusions introduction
About 300 mL of fluid is required for the
Pleural Effusions introduction
About 300 mL of fluid is required for the
Transudative Vs. Exudative Effusions
Criteria:
1. Pleural fluid protein/serum protein greater
Transudative Vs. Exudative Effusions
Criteria:
1. Pleural fluid protein/serum protein greater
Diagnostic Approach
The leading causes of transudative pleural effusions in the United
Diagnostic Approach
The leading causes of transudative pleural effusions in the United
Pleural fluid analysis
Gross appearance (pus- Empyema, black- Aspergillus, green- Biliothorax, white- Chylothorax)
Very
Pleural fluid analysis
Gross appearance (pus- Empyema, black- Aspergillus, green- Biliothorax, white- Chylothorax)
Very

Effusion Due to Heart Failure
A diagnostic thoracentesis should be performed
Effusion Due to Heart Failure
A diagnostic thoracentesis should be performed
Hepatic Hydrothorax
Pleural effusions occur in ~5% of patients with cirrhosis and
Hepatic Hydrothorax
Pleural effusions occur in ~5% of patients with cirrhosis and
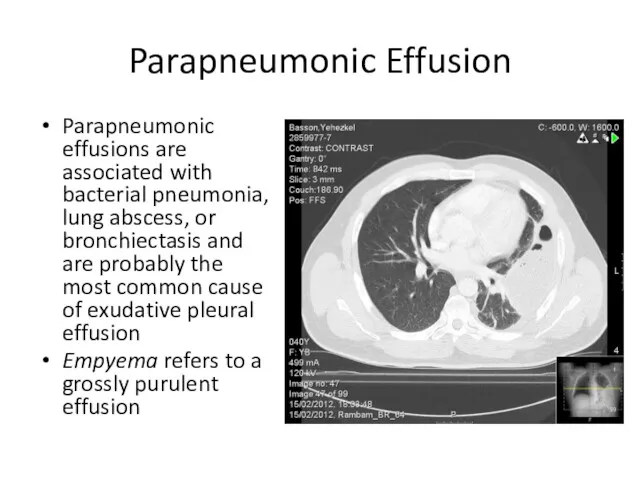
Parapneumonic Effusion
Parapneumonic effusions are associated with bacterial pneumonia, lung abscess, or
Parapneumonic Effusion
Parapneumonic effusions are associated with bacterial pneumonia, lung abscess, or
Parapneumonic Effusion
Patients with aerobic bacterial pneumonia and pleural effusion present with
Parapneumonic Effusion
Patients with aerobic bacterial pneumonia and pleural effusion present with
Uncomplicated Vs. Complicated parapneumonic effusion
An uncomplicated parapneumonic effusion has "exudative"
Uncomplicated Vs. Complicated parapneumonic effusion
An uncomplicated parapneumonic effusion has "exudative"
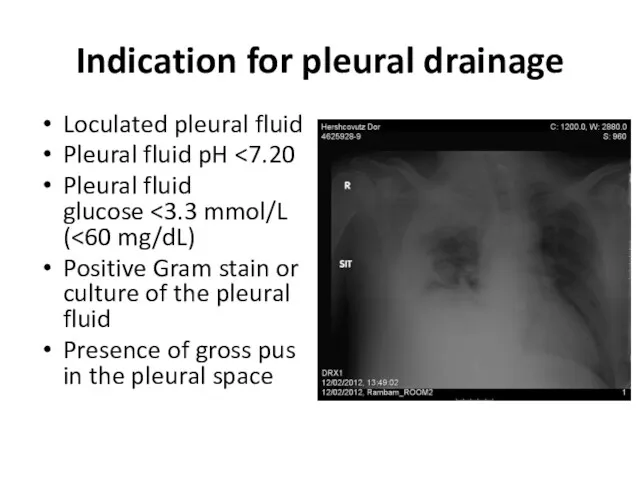
Indication for pleural drainage
Loculated pleural fluid
Pleural fluid pH <7.20
Pleural fluid glucose <3.3
Indication for pleural drainage
Loculated pleural fluid
Pleural fluid pH <7.20
Pleural fluid glucose <3.3
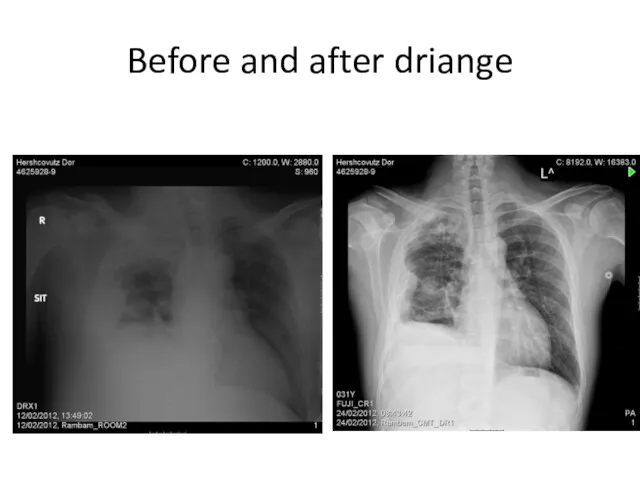
Before and after driange
Before and after driange
Treatment of parapneumonic effusion
An empiric, broad spectrum antibiotic that includes
Treatment of parapneumonic effusion
An empiric, broad spectrum antibiotic that includes

Effusion Secondary to Malignancy
Malignant pleural effusions secondary to metastatic disease are
Effusion Secondary to Malignancy
Malignant pleural effusions secondary to metastatic disease are

Effusion Secondary to Malignancy
The diagnosis usually is made via cytology of
Effusion Secondary to Malignancy
The diagnosis usually is made via cytology of
Treatment of Malignant pleural effusion
If the patient's lifestyle is compromised
Treatment of Malignant pleural effusion
If the patient's lifestyle is compromised
Pneumothorax introduction
Pneumothorax is the accumulation of air within the pleural space
Pneumothorax
Pneumothorax introduction
Pneumothorax is the accumulation of air within the pleural space
Pneumothorax
Pneumothorax introduction
Patients with pneumothorax most commonly present with chest pain (sharp
Pneumothorax introduction
Patients with pneumothorax most commonly present with chest pain (sharp
diagnosis
A pneumothorax usually is seen on the standard posteroanterior chest radiograph
diagnosis
A pneumothorax usually is seen on the standard posteroanterior chest radiograph
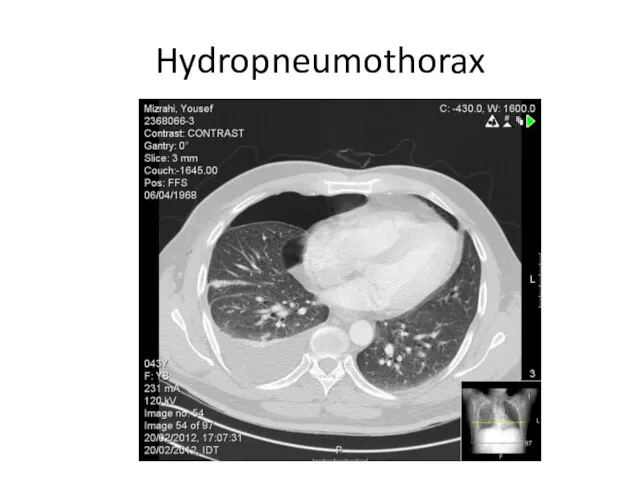
Hydropneumothorax
Hydropneumothorax
Classifications of Pneumothorax
Spontaneous
Primary
Secondary
Traumatic
Iatrogenic
Esophageal perforation
Classifications of Pneumothorax
Spontaneous
Primary
Secondary
Traumatic
Iatrogenic
Esophageal perforation
primary spontaneous pneumothorax
A primary spontaneous pneumothorax occurs in the absence
primary spontaneous pneumothorax
A primary spontaneous pneumothorax occurs in the absence
Treatment of primary spontaneous pneumothorax
Small pneumothoraces (<20%, ≤2 to 3
Treatment of primary spontaneous pneumothorax
Small pneumothoraces (<20%, ≤2 to 3
Treatment of primary spontaneous pneumothorax
Moderate (20%-40%) and large (>40%) pneumothoraces
Treatment of primary spontaneous pneumothorax
Moderate (20%-40%) and large (>40%) pneumothoraces
Treatment of primary spontaneous pneumothorax
Complications of chest tube insertion for
Treatment of primary spontaneous pneumothorax
Complications of chest tube insertion for
Indication for Surgical intervention in spontaneous pneumothorax
Air leak that persist
Indication for Surgical intervention in spontaneous pneumothorax
Air leak that persist
Surgical intervention for spontaneous pneumothorax
Apical blebs are resected. The parietal
Surgical intervention for spontaneous pneumothorax
Apical blebs are resected. The parietal
Secondary spontaneous pneumothorax
Most secondary pneumothoraxes are due to chronic obstructive
Secondary spontaneous pneumothorax
Most secondary pneumothoraxes are due to chronic obstructive
Preventing recurrence
smoking cessation
VATS pleurodesis- The rate of recurrent pneumothorax is less
Preventing recurrence
smoking cessation
VATS pleurodesis- The rate of recurrent pneumothorax is less

Traumatic pneumothoraxes
Traumatic pneumothoraxes can result from both penetrating and blunt
Traumatic pneumothoraxes
Traumatic pneumothoraxes can result from both penetrating and blunt

Traumatic pneumothoraxes
Traumatic pneumothoraxes
Iatrogenic pneumothorax
Iatrogenic pneumothorax is a type of traumatic pneumothorax that is
Iatrogenic pneumothorax
Iatrogenic pneumothorax is a type of traumatic pneumothorax that is
tension pneumothorax
hemodynamic collapse (decreased venous return to the heart and reduced
tension pneumothorax
hemodynamic collapse (decreased venous return to the heart and reduced
Diagnosis of tension pneumothorax
The diagnosis is made by physical examination:
An enlarged
Diagnosis of tension pneumothorax
The diagnosis is made by physical examination:
An enlarged
 Электрофизиологические основы ЭКГ. Электрическая ось сердца. ЭКГ-характеристика гипертрофий
Электрофизиологические основы ЭКГ. Электрическая ось сердца. ЭКГ-характеристика гипертрофий Предлежание плаценты
Предлежание плаценты Эвтаназия, как важнейшая проблема современной биоэтики. Хоспис, как альтернатива активной эвтаназии
Эвтаназия, как важнейшая проблема современной биоэтики. Хоспис, как альтернатива активной эвтаназии Организация работы органов, осуществляющих медицинскую помощь гражданам. Тема 8
Организация работы органов, осуществляющих медицинскую помощь гражданам. Тема 8 Атеросклероз. Клиникалық қөріністері. Емдеу жолдары. Қорытынды
Атеросклероз. Клиникалық қөріністері. Емдеу жолдары. Қорытынды Организация работы детской городской поликлиники и больницы
Организация работы детской городской поликлиники и больницы Воспаление висцеральной и париетальной брюшины малого таза - пельвиоперитонит
Воспаление висцеральной и париетальной брюшины малого таза - пельвиоперитонит Современное состояние и перспективы развития антимикробной химиотерапии
Современное состояние и перспективы развития антимикробной химиотерапии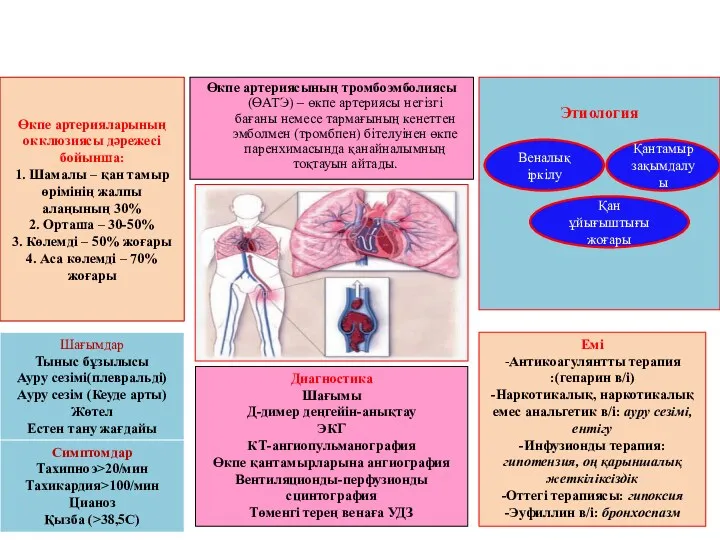 Өкпе артерияларының окклюзиясы дəрежесі бойынша: 1. Шамалы – қан тамыр өрімінің жалпы алаңының 30% 2. Орташа – 30-50% 3
Өкпе артерияларының окклюзиясы дəрежесі бойынша: 1. Шамалы – қан тамыр өрімінің жалпы алаңының 30% 2. Орташа – 30-50% 3 Синдром болей в левой половине грудной клетки. ИБС в практике терапевта поликлиники
Синдром болей в левой половине грудной клетки. ИБС в практике терапевта поликлиники Острая церебральная недостаточность
Острая церебральная недостаточность Клеточные факторы врождённого иммунитета. Фагоцитоз и его стадии
Клеточные факторы врождённого иммунитета. Фагоцитоз и его стадии Общие закономерности роста и развития детей и подростков
Общие закономерности роста и развития детей и подростков Қыз балалар гинекологиясының негіздері
Қыз балалар гинекологиясының негіздері Расстройства внимания
Расстройства внимания Острый респираторный дистресс-синдром
Острый респираторный дистресс-синдром Острый ларингит
Острый ларингит Физическое развитие и функциональное состояние организма. Медицинский контроль
Физическое развитие и функциональное состояние организма. Медицинский контроль Церебральные инсульты у взрослых
Церебральные инсульты у взрослых Специфические заболевания ЛОР-органов
Специфические заболевания ЛОР-органов Диагностика в терапии. Заболевания сердечно-сосудистой системы
Диагностика в терапии. Заболевания сердечно-сосудистой системы Ишемическая болезнь сердца. Стабильная стенокардия напряжения. Ведение на современном этапе
Ишемическая болезнь сердца. Стабильная стенокардия напряжения. Ведение на современном этапе Энтероколит. Колиттер. Гельминтоздар
Энтероколит. Колиттер. Гельминтоздар Пищевая аллергия и пищевая непереносимость
Пищевая аллергия и пищевая непереносимость Стоматологические материалы на основе полимеров (базисные и для искусственных зубов)
Стоматологические материалы на основе полимеров (базисные и для искусственных зубов) Tпринципы терапии дыхательных расстройств
Tпринципы терапии дыхательных расстройств Этика и деонтология для работников регистратур медицинских организаций
Этика и деонтология для работников регистратур медицинских организаций Лучевые синдромы поражения легких
Лучевые синдромы поражения легких