- Pulpitis etiology, pathogeny and classifications

Содержание
- 2. Introduction Endodontics is the specialty of dentistry that manages the prevention, diagnosis, and treatment of the
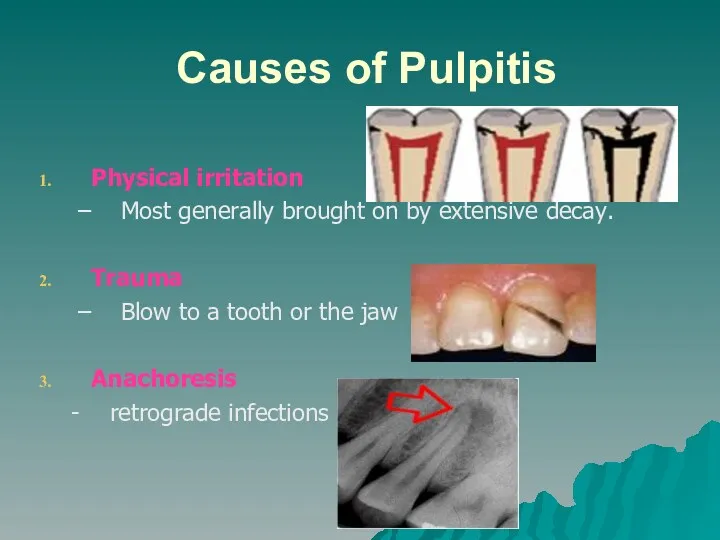
- 3. Causes of Pulpitis Physical irritation Most generally brought on by extensive decay. Trauma Blow to a
- 4. Signs and Symptoms Pain when biting down Pain when chewing Sensitivity with hot or cold beverages
- 5. Endodontic Diagnosis Subjective examination Chief complaint Character and duration of pain Painful stimuli Sensitivity to biting
- 6. Important questions? What do you think the problem is? Does it hurt to hot or cold?
- 7. Objective examination Extent of decay Periodontal conditions surrounding the tooth in question Presence of an extensive
- 8. Challenges in diagnosis of pulpitis Referred pain & the lack of proprioceptors in the pulp localizing
- 9. Diagnostic Tests Percussion Palpation Thermal Electrical Radiographs
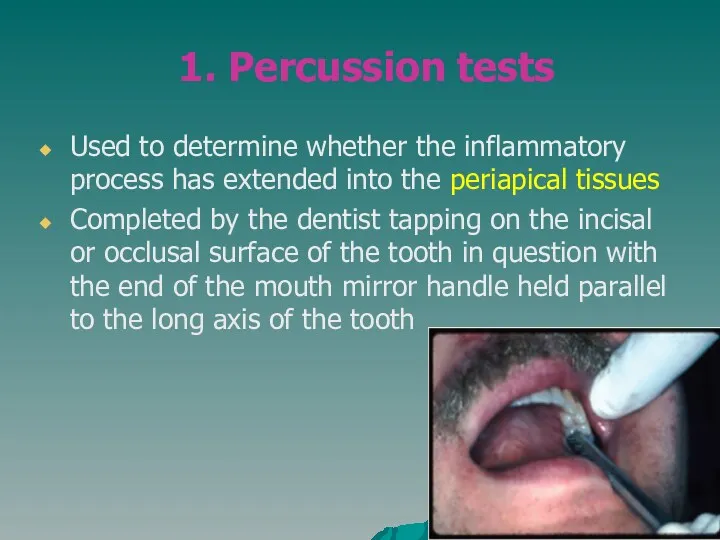
- 10. 1. Percussion tests Used to determine whether the inflammatory process has extended into the periapical tissues
- 11. Used to determine whether the inflammatory process has extended into the periapical tissues The dentist applies
- 12. 3. Thermal sensitivity Necrotic pulp will not respond to cold or hot Cold test Ice, dry
- 13. Evaluation of thermal test results 4 distinct responses: No response non-vital pulp or false negative Mild
- 15. Causes of false positives/negative Calcified canals Immature apex – usually seen in young patients Trauma Premedication
- 16. 4. Electric pulp testing Delivers a small electrical stimulus to the pulp Factors that may influence
- 17. Placement of a pulp tester.
- 19. 5. Radiographs Pre-operative radiograph Invaluable diagnostic tool Periapical radiolucency Widening of PDL Deep caries Resorption Pulp
- 20. Requirements of Endodontic Films Show 4-5 mm beyond the apex of the tooth and the surrounding
- 21. Quality radiograph in endodontics.
- 22. Diagnostic Conclusions Normal pulp Pulpitis
- 23. Normal pulp There are no subjective symptoms or objective signs. The pulp responds normally to sensory
- 24. Pulpitis The pulp tissues have become inflamed Can be either: Acute – inflammation of the periapical
- 25. Acute Pulpitis mainly occurs in children teeth and adolescent pain is more pronounced than in chronic
- 26. Symptoms and Signs of acute pulpitis The pain not localized in the affected tooth is constant
- 28. Forms of acute pulpitis 1. Form of purulent acute where the pulp is totally inflammed 2.
- 29. Chronic Pulpitis Reversible Irreversible
- 30. Reversible pulpitis The pulp is irritated, and the patient is experiencing pain to thermal stimuli Sharp
- 31. Irreversible pulpitis The tooth will display symptoms of lingering pain pain occurs spontaneously or lingers minutes
- 32. Periradicular abscess An inflammatory reaction to pulpal infection that can be chronic or have rapid onset
- 34. An inflammatory reaction frequently caused by bacteria entrapped in the periodontal sulcus for a long time.
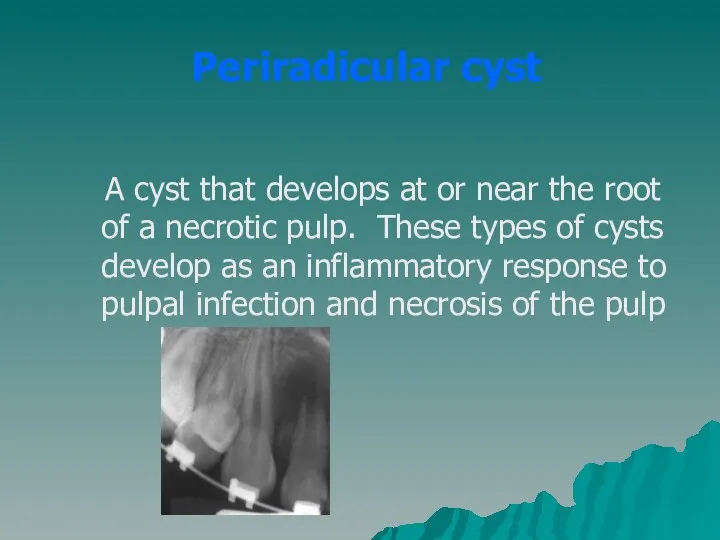
- 36. Periradicular cyst A cyst that develops at or near the root of a necrotic pulp. These
- 37. Pulp fibrosis The decrease of living cells within the pulp causing fibrous tissue to take over
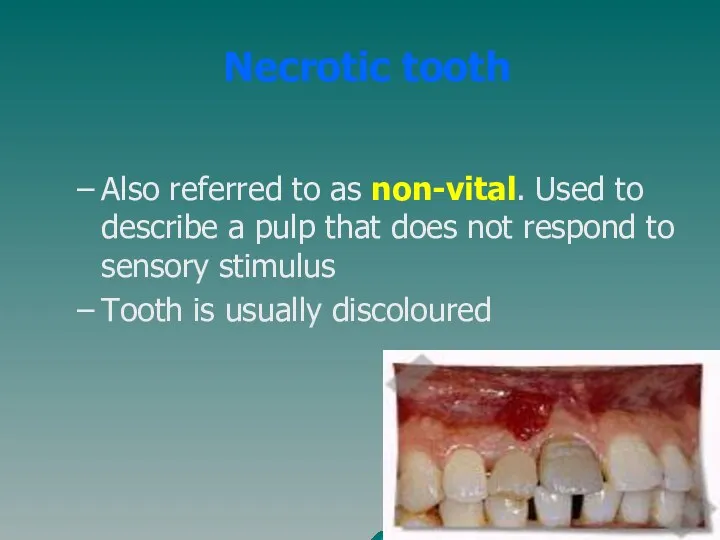
- 38. Necrotic tooth Also referred to as non-vital. Used to describe a pulp that does not respond
- 39. Plan of Treatment Depends widely on the diagnosis
- 40. Simple plan of treatment Visit 1: Medical history History of the tooth Access cavity Place rubberdam
- 41. Visit 2: Working length determination Debridement using the hybrid technique Irrigation Placed intra-canal medication (calcium hydroxide)
- 42. Visit 3: Obturation with GP using lateral condensation Placed temporary/permanent restoration (IRM/Kalzinol)
- 43. Referral To appropriate discipline
- 44. Remember Access cavity shapes: Anterior – inverted triangle Premolars – round Molars – rhomboid Always use
- 45. Contraindications for RCT Caries extending beyond bone level Rubberdam cannot be placed Crown of tooth cannot
- 46. Inter & cross-departmental diagnosis Mobile teeth Teeth associated with severe periodontal problems Confusion between TMJ dysfunctional
- 48. Скачать презентацию
Introduction
Endodontics is the specialty of dentistry that manages the prevention, diagnosis,
Introduction
Endodontics is the specialty of dentistry that manages the prevention, diagnosis,
Causes of Pulpitis
Physical irritation
Most generally brought on by extensive decay.
Trauma
Causes of Pulpitis
Physical irritation
Most generally brought on by extensive decay.
Trauma
Signs and Symptoms
Pain when biting down
Pain when chewing
Sensitivity with hot
Signs and Symptoms
Pain when biting down
Pain when chewing
Sensitivity with hot
Endodontic Diagnosis
Subjective examination
Chief complaint
Character and duration of pain
Painful stimuli
Endodontic Diagnosis
Subjective examination
Chief complaint
Character and duration of pain
Painful stimuli
Important questions?
What do you think the problem is?
Does it hurt
Important questions?
What do you think the problem is?
Does it hurt
Objective examination
Extent of decay
Periodontal conditions surrounding the tooth in question
Objective examination
Extent of decay
Periodontal conditions surrounding the tooth in question
Challenges in diagnosis of pulpitis
Referred pain & the lack of proprioceptors
Challenges in diagnosis of pulpitis
Referred pain & the lack of proprioceptors
Diagnostic Tests
Percussion
Palpation
Thermal
Electrical
Radiographs
Diagnostic Tests
Percussion
Palpation
Thermal
Electrical
Radiographs
1. Percussion tests
Used to determine whether the inflammatory process has extended
1. Percussion tests
Used to determine whether the inflammatory process has extended
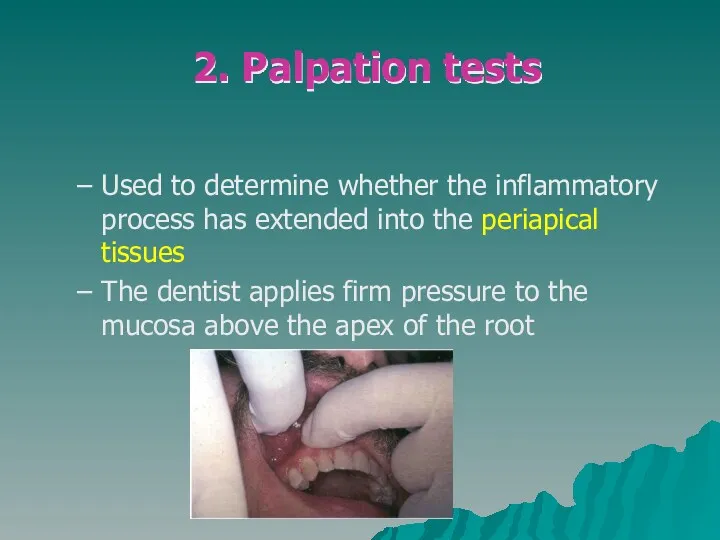
Used to determine whether the inflammatory process has extended into the
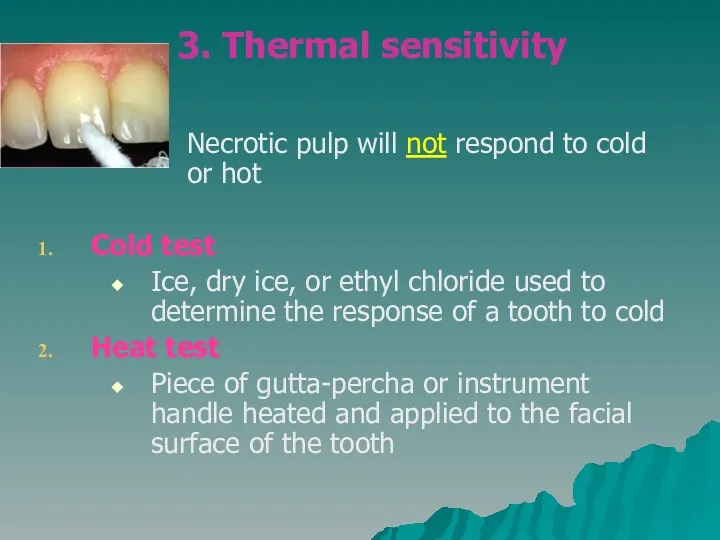
3. Thermal sensitivity
Necrotic pulp will not respond to cold
3. Thermal sensitivity
Necrotic pulp will not respond to cold
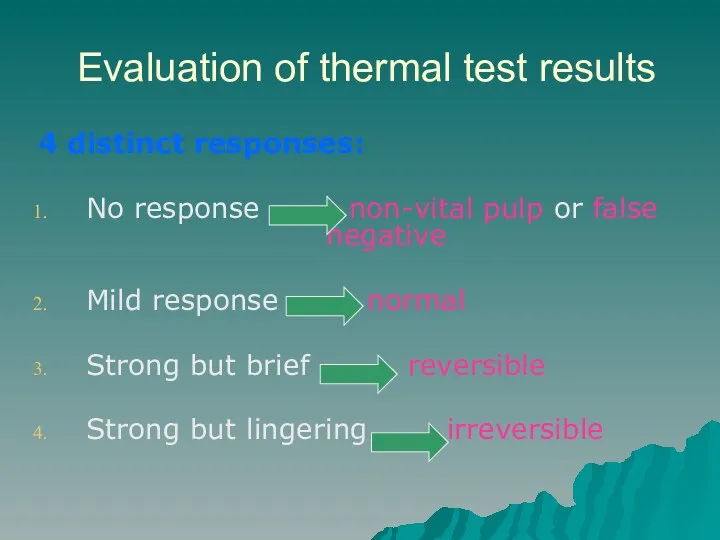
Evaluation of thermal test results
4 distinct responses:
No response non-vital pulp or
Evaluation of thermal test results
4 distinct responses:
No response non-vital pulp or

Causes of false positives/negative
Calcified canals
Immature apex – usually seen in young
Causes of false positives/negative
Calcified canals
Immature apex – usually seen in young
4. Electric pulp testing
Delivers a small electrical stimulus to the pulp
4. Electric pulp testing
Delivers a small electrical stimulus to the pulp
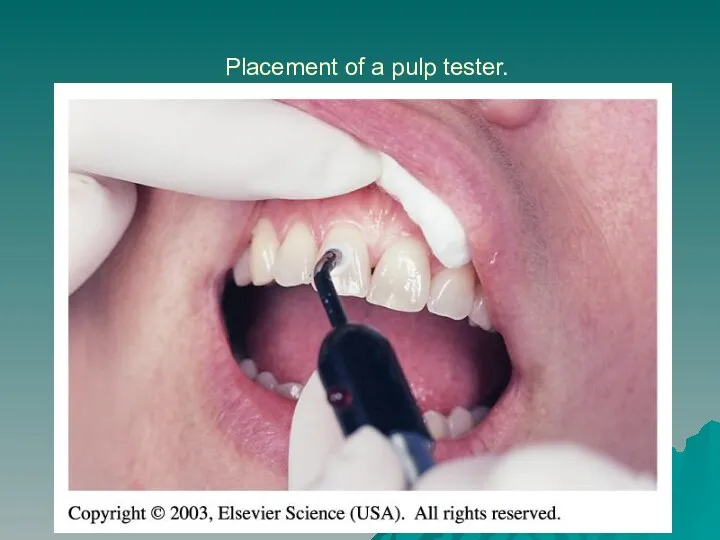
Placement of a pulp tester.
Placement of a pulp tester.

5. Radiographs
Pre-operative radiograph
Invaluable diagnostic tool
Periapical radiolucency
Widening of PDL
Deep caries
Resorption
Pulp
5. Radiographs
Pre-operative radiograph
Invaluable diagnostic tool
Periapical radiolucency
Widening of PDL
Deep caries
Resorption
Pulp
Requirements of Endodontic Films
Show 4-5 mm beyond the apex of the
Requirements of Endodontic Films
Show 4-5 mm beyond the apex of the
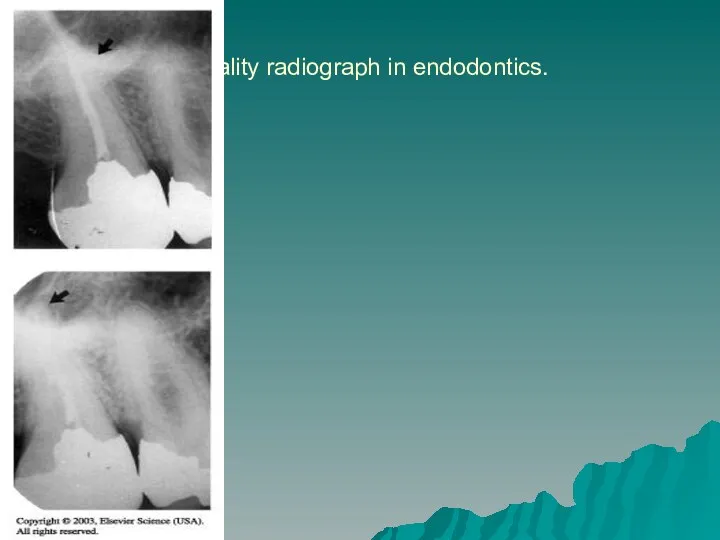
Quality radiograph in endodontics.
Quality radiograph in endodontics.
Diagnostic Conclusions
Normal pulp
Pulpitis
Diagnostic Conclusions
Normal pulp
Pulpitis
Normal pulp
There are no subjective symptoms or objective signs. The
Normal pulp
There are no subjective symptoms or objective signs. The
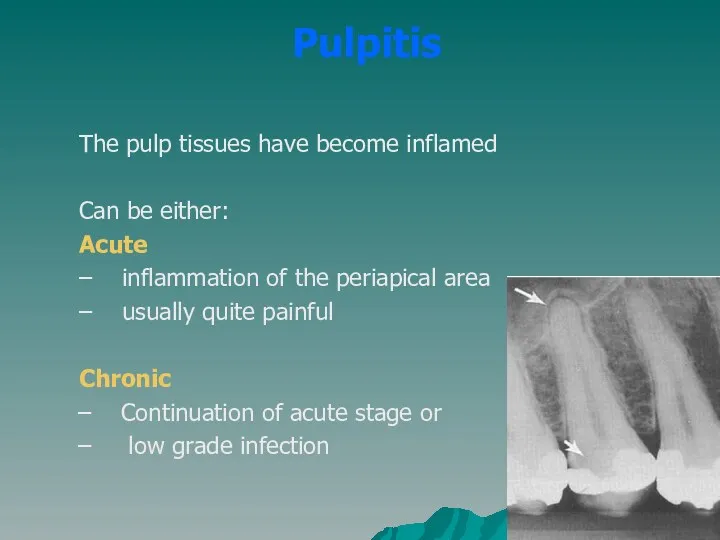
Pulpitis
The pulp tissues have become inflamed
Can be either:
Acute
– inflammation
Pulpitis
The pulp tissues have become inflamed
Can be either:
Acute
– inflammation
Acute Pulpitis
mainly occurs in children teeth and adolescent
pain is more pronounced
Acute Pulpitis
mainly occurs in children teeth and adolescent
pain is more pronounced
Symptoms and Signs of acute pulpitis
The pain not localized in the
Symptoms and Signs of acute pulpitis
The pain not localized in the

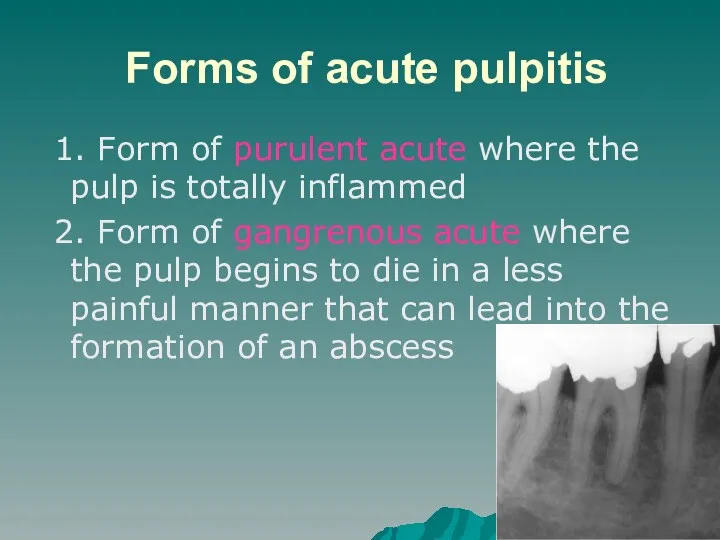
Forms of acute pulpitis
1. Form of purulent acute where the
Forms of acute pulpitis
1. Form of purulent acute where the
Chronic Pulpitis
Reversible
Irreversible
Chronic Pulpitis
Reversible
Irreversible
Reversible pulpitis
The pulp is irritated, and the patient is experiencing pain
Reversible pulpitis
The pulp is irritated, and the patient is experiencing pain
Irreversible pulpitis
The tooth will display symptoms of lingering pain
pain occurs spontaneously
Irreversible pulpitis
The tooth will display symptoms of lingering pain
pain occurs spontaneously
Periradicular abscess
An inflammatory reaction to pulpal infection that can be
Periradicular abscess
An inflammatory reaction to pulpal infection that can be

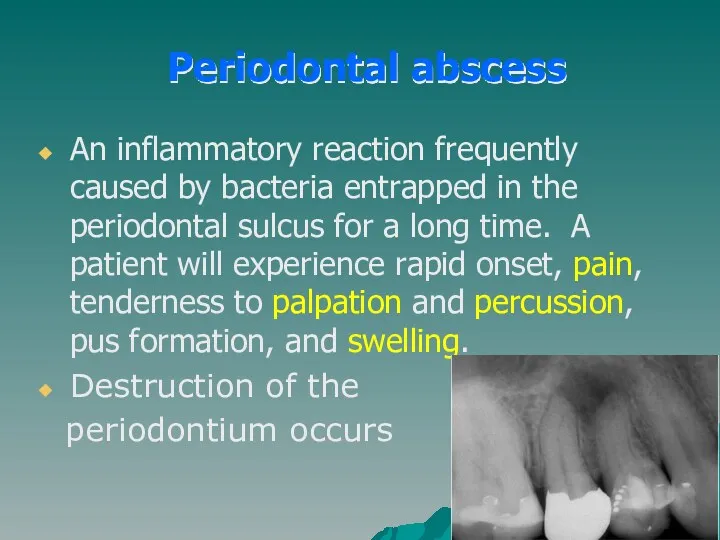
An inflammatory reaction frequently caused by bacteria entrapped in the periodontal
An inflammatory reaction frequently caused by bacteria entrapped in the periodontal

Periradicular cyst
A cyst that develops at or near the root
Periradicular cyst
A cyst that develops at or near the root
Pulp fibrosis
The decrease of living cells within the pulp causing
Pulp fibrosis
The decrease of living cells within the pulp causing
Necrotic tooth
Also referred to as non-vital. Used to describe a pulp
Necrotic tooth
Also referred to as non-vital. Used to describe a pulp
Plan of Treatment
Depends widely on the diagnosis
Plan of Treatment
Depends widely on the diagnosis
Simple plan of treatment
Visit 1:
Medical history
History of the tooth
Access cavity
Place rubberdam
Extirpation
Simple plan of treatment
Visit 1:
Medical history
History of the tooth
Access cavity
Place rubberdam
Extirpation
Visit 2:
Working length determination
Debridement using the hybrid technique
Irrigation
Placed intra-canal medication (calcium
Visit 2:
Working length determination
Debridement using the hybrid technique
Irrigation
Placed intra-canal medication (calcium
Visit 3:
Obturation with GP using lateral condensation
Placed temporary/permanent restoration (IRM/Kalzinol)
Visit 3:
Obturation with GP using lateral condensation
Placed temporary/permanent restoration (IRM/Kalzinol)
Referral
To appropriate discipline
Referral
To appropriate discipline
Remember
Access cavity shapes:
Anterior – inverted triangle
Premolars – round
Molars – rhomboid
Always
Remember
Access cavity shapes:
Anterior – inverted triangle
Premolars – round
Molars – rhomboid
Always
Contraindications for RCT
Caries extending beyond bone level
Rubberdam cannot be placed
Crown of
Contraindications for RCT
Caries extending beyond bone level
Rubberdam cannot be placed
Crown of
Inter & cross-departmental diagnosis
Mobile teeth
Teeth associated with severe periodontal problems
Confusion
Inter & cross-departmental diagnosis
Mobile teeth
Teeth associated with severe periodontal problems
Confusion
 Депрессия в пожилом возрасте
Депрессия в пожилом возрасте Рак ободочной кишки (C-r coli)
Рак ободочной кишки (C-r coli) Проблема здоровья людей: глобальный аспект
Проблема здоровья людей: глобальный аспект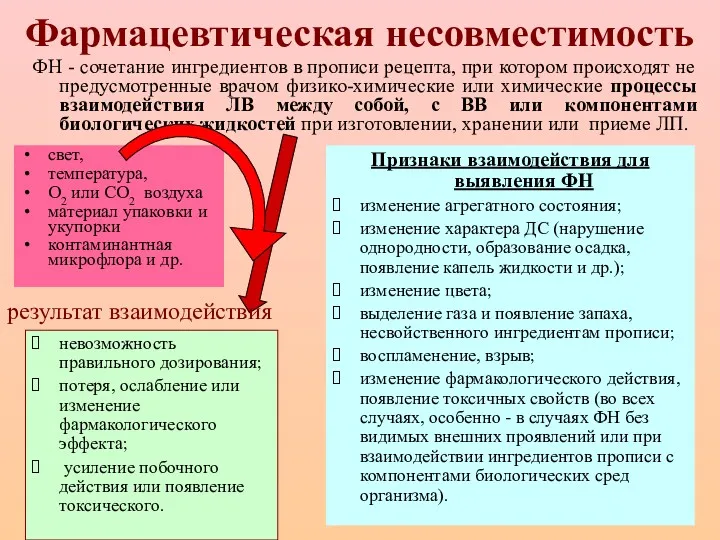 Фармацевтическая несовместимость
Фармацевтическая несовместимость Злокачественные новообразования желудка
Злокачественные новообразования желудка Средства индивидуальной защиты (противочумные костюмы I, II, III, IV типа)
Средства индивидуальной защиты (противочумные костюмы I, II, III, IV типа) Острая ревматическая лихорадка
Острая ревматическая лихорадка Дәрігер мен науқас арасында туындайтын шиеленіс
Дәрігер мен науқас арасында туындайтын шиеленіс Алькогольдің адам организміне зияны
Алькогольдің адам организміне зияны Определение группы крови по системе АВ0 моноклональными антителами (цоликлонами)
Определение группы крови по системе АВ0 моноклональными антителами (цоликлонами) Инфекционные заболевания и беременность
Инфекционные заболевания и беременность Регуляция кровообращения
Регуляция кровообращения Неспецифическая хирургическая инфекция
Неспецифическая хирургическая инфекция Деонтология в хирургии
Деонтология в хирургии Генетика и наследственные заболевания человека
Генетика и наследственные заболевания человека Виды частичных съемных протезов. Способы их фиксации
Виды частичных съемных протезов. Способы их фиксации Ультразвуковая диагностика заболеваний вен нижних конечностей
Ультразвуковая диагностика заболеваний вен нижних конечностей Витамины. (Часть 2)
Витамины. (Часть 2) Психотерапевтический метод музыкотерапия
Психотерапевтический метод музыкотерапия Лечение туберкулеза у детей и подростков
Лечение туберкулеза у детей и подростков DSD-template
DSD-template Отбасын жоспарлау сұрақтары. Контрацепция. Әйелдің репродуктивті денсаулығын қорғау
Отбасын жоспарлау сұрақтары. Контрацепция. Әйелдің репродуктивті денсаулығын қорғау Гемолитическая болезнь новорожденных
Гемолитическая болезнь новорожденных Профилактика, диагностика, и оптимизация лечения маргинальной резорбции костной ткани
Профилактика, диагностика, и оптимизация лечения маргинальной резорбции костной ткани Закономерности распределения лекарственных веществ в организме мелких домашних животных
Закономерности распределения лекарственных веществ в организме мелких домашних животных Врожденная дисфункция коры надпочечников
Врожденная дисфункция коры надпочечников Тіс ішінара болмағанда немесе түгел болмағанда қолданылатын ортопедиялық ем. Операциялық және қалпына келтіретін дентистрия
Тіс ішінара болмағанда немесе түгел болмағанда қолданылатын ортопедиялық ем. Операциялық және қалпына келтіретін дентистрия Жасына сәйкес екпе алмаған балаға жеке егу күнтізбесін құрастыру
Жасына сәйкес екпе алмаған балаға жеке егу күнтізбесін құрастыру