- Techniques to reduce postoperative opioid requirements

Содержание
- 2. OVERVIEW Problems with opioids Hypothesis: if I improve analgesia with non-opioids, I can give less opioid,
- 3. INTRAOPERATIVE TECHNIQUES Prevent opioid hyperalgesia Wound infiltration or regional anesthesia Limit spinal cord wind-up NMDA antagonists,
- 4. PROBLEMS WITH OPIOIDS Pharmacogenetic Organ-specific side effects Physiologic effects Hyperalgesia, tolerance, addiction Inadequate pain relief Adverse
- 5. PHARMACOGENETIC ISSUES WITH OPIOIDS Cytochrome P450 enzyme CYP2D6 Normal (extensive metabolizers) convert: Codeine (inactive) -> morphine
- 6. ORGAN-SPECIFIC SIDE EFFECTS WITH OPIOIDS - 1 GI Stomach: decreased emptying, nausea, vomiting Gallbladder: biliary spasm
- 7. ORGAN-SPECIFIC SIDE EFFECTS WITH OPIOIDS - 2 Respiratory Hypoventilation, decreased ventilatory response to hypoxia & hypercarbia,
- 8. ORGAN-SPECIFIC SIDE EFFECTS WITH OPIOIDS - 3 GU – urinary retention CNS – dysphoria, hallucinations, coma
- 9. REVERSING OPIOID SIDE EFFECTS - 1 Symptomatic therapy Nausea, vomiting: 5-HT3 antagonists Ileus: lidocaine, Constipation: laxatives
- 10. REVERSING OPIOID SIDE EFFECTS - 2 Systemic antagonists – reverse analgesia Peripheral antagonists (in development) Do
- 11. UNDESIRABLE PHYSIOLOGIC EFFECTS OF OPIOIDS Hyperalgesia NMDA receptor Tolerance NMDA receptor Addiction
- 12. PATIENT PERCEPTION of PAIN after OUTPATIENT SURGERY Apfelbaum. A-1 At home after surgery 82% - moderate
- 13. EXCESSIVE PAIN after AMBULATORY SURGERY Chung F. Anesth Analg 1999; 89: 1352-9 Excessive pain 9.5% 22%
- 14. POSTOPERATIVE CHRONIC PAIN STATES - 1 Perkins, Kehlet. Chronic pain as an outcome of surgery. Anesthesiology
- 15. POSTOPERATIVE CHRONIC PAIN STATES - 2 Perkins, Kehlet. Chronic pain as an outcome of surgery. Anesthesiology
- 16. PAIN PHYSIOLOGY REVIEW Potential sites of intervention Peripheral nerve ending Peripheral nerve transmission Dorsal horn Spinal
- 17. PERIPHERAL NERVE ENDINGS Pain receptor (nociceptor) stimulation Incision, traction, cutting, pressure Nociceptor sensitization Inflammatory mediators Primary
- 18. PERIPHERAL NERVE TRANSMISSION Normal A-δ fibers (sharp) + c-fibers (dull) 70-90% of peripheral nerve; reserve:total =
- 19. DORSAL HORN Termination of nociceptor input Lamina I – A-δ fibers Lamina II (substantia gelatinosa) –
- 20. SPINAL CORD Ascending tracts Supraspinal reflexes – surgical stress response Descending tracts Opioids, α2-agonists Spinal cord
- 21. OPIOID HYPERALGESIA Vinik. Anesth Analg 1998;86:1307 Rapid Development of Tolerance to Analgesia during Remifentanil Infusion in
- 22. PREVENT OPIOID HYPERALGESIA Luginbuhl. Anesth Analg 2003;96:726 Modulation of Remifentanil-induced Analgesia, Hyperalgesia, and Tolerance by Small-Dose
- 23. Koppert. Anesthesiology 2003;99:152
- 24. WOUND INFILTRATION – BLOCK NERVE ENDINGS REGIONAL ANESTHESIA – BLOCK NERVE TRANSMISSION
- 25. WOUND INFILTRATION – BLOCK NERVE ENDINGS Bianconi. Anesth Analg 2004; 98:166 Pharmacokinetics & Efficacy of Ropivacaine
- 26. VAS during Passive Mobilization after Spine Surgery Bianconi. Anesth Analg 2004;98:166
- 27. Diclofenac (mg, im) & Tramadol (mg, iv) Rescue after Spine Surgery Bianconi. Anesth Analg 2004;98:166
- 28. Maximum Pain Scores after Elective Shoulder Surgery Wurm. ANESTH ANALG 2003;97:1620 Pre- vs Postop Interscalene Block
- 29. REGIONAL ANALGESIA initiated during surgery DECREASES OPIOID DEMAND after inpatient surgery Wang. A-135 Capdevila. Anesthesiology 1999;
- 30. LIMIT SPINAL CORD WIND-UP NMDA antagonists Magnesium Ketamine NSAIDS Local anesthetics iv
- 31. Ketamine: Pre-incision vs. Pre-emergence Fu. Anesth Analg 1997; 84:1086 Ketamine administration Pre-incision group 0.5 mg/kg bolus
- 32. Ketamine: Pre-incision vs. Pre-emergence Effect on Morphine (mg) Administered Fu. Anesth Analg 1997; 84:1086
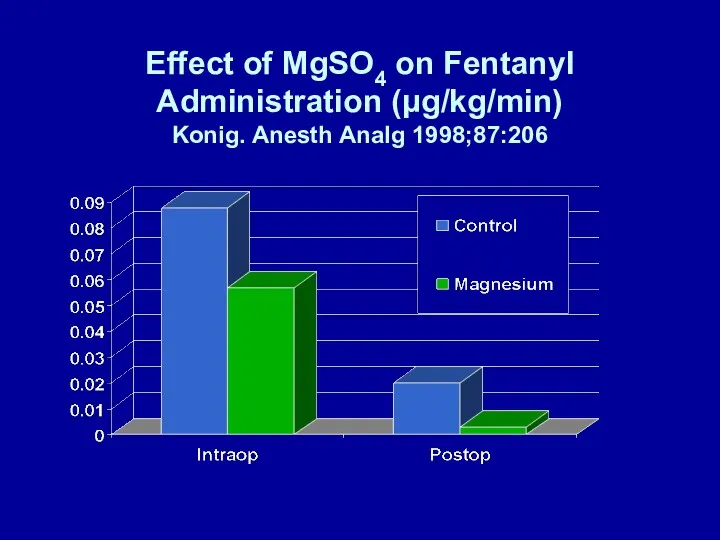
- 33. Intraoperative MgSO4 Reduces Fentanyl Requirements During and After Knee Arthroscopy Konig. Anesth Analg 1998; 87:206 MgSO4
- 34. Effect of MgSO4 on Fentanyl Administration (μg/kg/min) Konig. Anesth Analg 1998;87:206
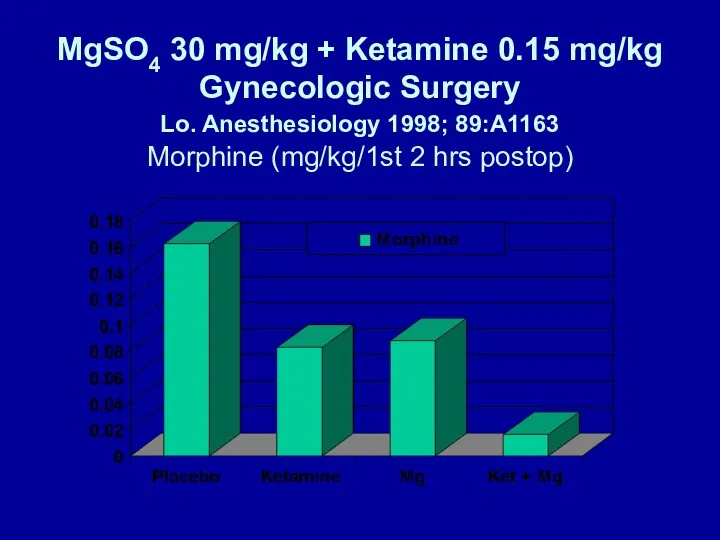
- 35. MgSO4 30 mg/kg + Ketamine 0.15 mg/kg Gynecologic Surgery Lo. Anesthesiology 1998; 89:A1163 Morphine (mg/kg/1st 2
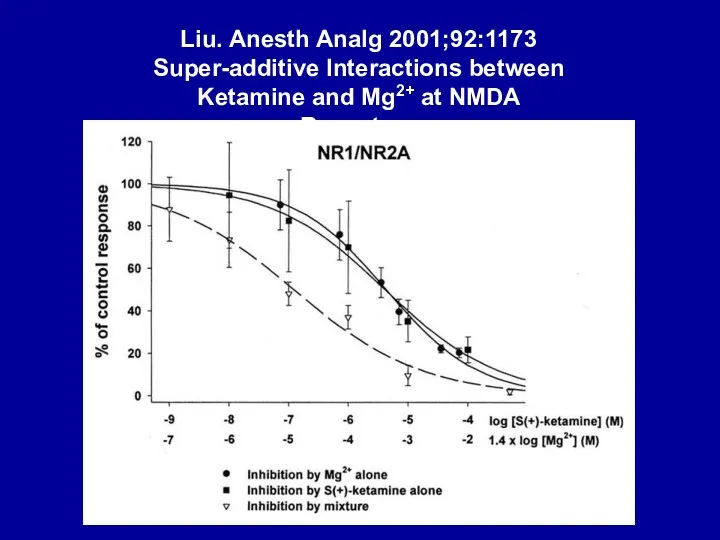
- 36. Liu. Anesth Analg 2001;92:1173 Super-additive Interactions between Ketamine and Mg2+ at NMDA Receptors
- 37. NMDA ANTAGONISTS - MAGNESIUM O’Flaherty, et al. A-1265 Pain after tonsillectomy, 40 patients 3-12 yrs Monitored
- 38. NEUROMUSCULAR BLOCKADE & Mg2+ Fuchs-Buder. Br J Anaesth 1995; 74:405 Mg2+ 40 mg/kg Reduces vecuronium ED50
- 39. NMDA ANTAGONISTS - METHADONE Byas-Smith, et al. Methadone produces greater reduction than fentanyl in post-operative morphine
- 40. PREOPERATIVE ADMINISTRATION OF ORAL NSAIDS DECREASES POSTOPERATIVE ANALGESIC DEMANDS Sinatra. Anesth Analg 2004; 98:135 Preoperative Rofecoxib
- 41. Preoperative Rofecoxib Oral Suspension as an Analgesic after Lower Abdominal Surgery Sinatra. Anesth Analg 2004; 98:135
- 42. Buvendendran. JAMA 2003;290:2411 Anesthesia for TKR Epidural bupivacaine/fentanyl + propofol “Traditional analgesia” (VAS Basal epidural +
- 43. Buvendendran. JAMA 2003;290:2411 Rofecoxib group (vs placebo) Less opioid asked for – PCEA and oral Fewer
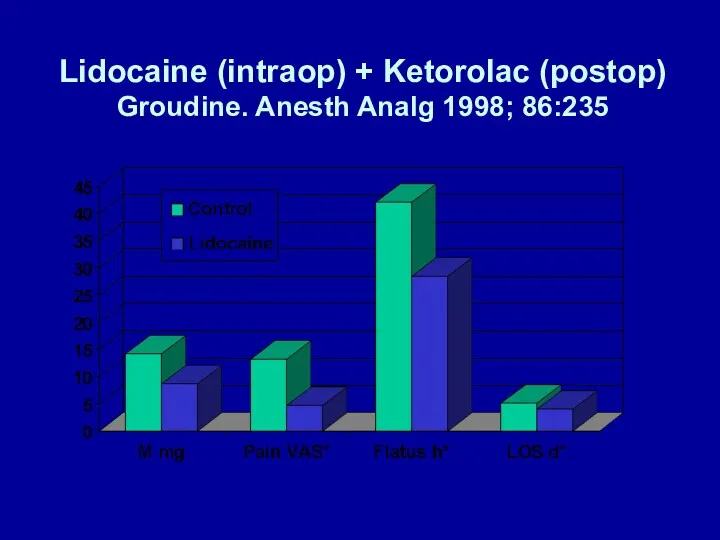
- 44. IV LIDOCAINE - 1 Groudine. Anesth Analg 1998; 86:235-9 Radical retropubic prostatectomy, 64-yr-olds Isoflurane-N2O-opioid anesthesia Lidocaine:
- 45. IV LIDOCAINE - 2 Groudine. Anesth Analg 1998; 86:235-9 Postoperative advantages Lower VAS pain scores Less
- 46. Lidocaine (intraop) + Ketorolac (postop) Groudine. Anesth Analg 1998; 86:235
- 47. IV LIDOCAINE - 3 Koppert. Anesthesiology 2000;93:A855 Abdominal surgery Lidocaine: none vs 1.5 mg/kg/hr surgery/PACU Total
- 48. Epidural Analgesia after Partial Colectomy Liu. Anesthesiology 1995; 83:757 What if [iv-lidocaine ± ketorolac + PCA-morphine]
- 49. β-ADRENERGIC RECEPTOR ANTAGONISTS REDUCE POSTOPERATIVE OPIOID REQUIREMENTS Zaugg. Anesthesiology 1999; 91:1674 White. Anesth Analg 2003; 97:1633
- 50. β-BLOCKERS REDUCE MORPHINE ADMINISTRATION Zaugg. Anesthesiology 1999;91:1674 75-yr-olds, major abdominal surgery Fentanyl-isoflurane anesthesia Atenolol administration (iv)
- 51. Atenolol Reduces Fentanyl (μg/kg/h) Intraop & Morphine (mg) in PACU Zaugg. Anesthesiology 1999; 91:1674
- 52. Esmolol Infusion Intraop Reduces # of Patients Requiring Analgesia White. Anesth Analg 2003;97:1633 Gyn laparoscopy Induction:
- 53. Esmolol Reduces Anesthetic Requirements, Need for Postop Analgesia, & LOS White. Anesth Analg 2003;97:1633
- 54. DOES MUSIC AFFECT ANESTHESIA OR POSTOPERATIVE ANALGESIA? Fentanyl (HR, BP), isoflurane (BIS 50) Yes Hemispheric synchronization,
- 55. DOES MUSIC AFFECT ANESTHESIA OR POSTOPERATIVE ANALGESIA? No (patient-selected CD or Hemi-Sync) Lumbar laminectomy (Hemi-Sync) Lewis.
- 56. SUMMARY Considerable research activity addressing Basic - new pain mechanisms Translational - new drugs based on
- 57. WHAT DO I DO DIFFFERENTLY? If general anesthesia and not regional or combined regional-general, I use:
- 59. WOUND INFILTRATION VS. SYSTEMIC LOCAL ANESTHETICS EMLA CREAM -> DECREASED POSTOPERATIVE PAIN Fassoulaki, et al. EMLA
- 60. α-ADRENERGIC RECEPTOR AGONISTS REDUCE POSTOPERATIVE OPIOID REQUIREMENTS Locus ceruleus (sedation) Dorsal horn (analgesia) Arain. Anesth Analg
- 62. Скачать презентацию
OVERVIEW
Problems with opioids
Hypothesis: if I improve analgesia with non-opioids, I can
OVERVIEW
Problems with opioids
Hypothesis: if I improve analgesia with non-opioids, I can
INTRAOPERATIVE TECHNIQUES
Prevent opioid hyperalgesia
Wound infiltration or regional anesthesia
Limit spinal cord wind-up
NMDA
INTRAOPERATIVE TECHNIQUES
Prevent opioid hyperalgesia
Wound infiltration or regional anesthesia
Limit spinal cord wind-up
NMDA
PROBLEMS WITH OPIOIDS
Pharmacogenetic
Organ-specific side effects
Physiologic effects
Hyperalgesia, tolerance, addiction
Inadequate pain relief
Adverse physiologic
PROBLEMS WITH OPIOIDS
Pharmacogenetic
Organ-specific side effects
Physiologic effects
Hyperalgesia, tolerance, addiction
Inadequate pain relief
Adverse physiologic
PHARMACOGENETIC ISSUES WITH OPIOIDS
Cytochrome P450 enzyme CYP2D6
Normal (extensive metabolizers) convert:
Codeine (inactive)
PHARMACOGENETIC ISSUES WITH OPIOIDS
Cytochrome P450 enzyme CYP2D6
Normal (extensive metabolizers) convert:
Codeine (inactive)
ORGAN-SPECIFIC SIDE EFFECTS WITH OPIOIDS - 1
GI
Stomach: decreased emptying, nausea, vomiting
Gallbladder:
ORGAN-SPECIFIC SIDE EFFECTS WITH OPIOIDS - 1
GI
Stomach: decreased emptying, nausea, vomiting
Gallbladder:
ORGAN-SPECIFIC SIDE EFFECTS WITH OPIOIDS - 2
Respiratory
Hypoventilation, decreased ventilatory response to
ORGAN-SPECIFIC SIDE EFFECTS WITH OPIOIDS - 2
Respiratory
Hypoventilation, decreased ventilatory response to
ORGAN-SPECIFIC SIDE EFFECTS WITH OPIOIDS - 3
GU – urinary retention
CNS –
ORGAN-SPECIFIC SIDE EFFECTS WITH OPIOIDS - 3
GU – urinary retention
CNS –
REVERSING OPIOID SIDE EFFECTS - 1
Symptomatic therapy
Nausea, vomiting: 5-HT3 antagonists
Ileus: lidocaine,
REVERSING OPIOID SIDE EFFECTS - 1
Symptomatic therapy
Nausea, vomiting: 5-HT3 antagonists
Ileus: lidocaine,
REVERSING OPIOID SIDE EFFECTS - 2
Systemic antagonists – reverse analgesia
Peripheral antagonists
REVERSING OPIOID SIDE EFFECTS - 2
Systemic antagonists – reverse analgesia
Peripheral antagonists
UNDESIRABLE PHYSIOLOGIC EFFECTS OF OPIOIDS
Hyperalgesia
NMDA receptor
Tolerance
NMDA receptor
Addiction
UNDESIRABLE PHYSIOLOGIC EFFECTS OF OPIOIDS
Hyperalgesia
NMDA receptor
Tolerance
NMDA receptor
Addiction
PATIENT PERCEPTION of PAIN after OUTPATIENT SURGERY
Apfelbaum. A-1
At home after surgery
82%
PATIENT PERCEPTION of PAIN after OUTPATIENT SURGERY
Apfelbaum. A-1
At home after surgery
82%
EXCESSIVE PAIN after AMBULATORY SURGERY
Chung F. Anesth Analg 1999; 89:
EXCESSIVE PAIN after AMBULATORY SURGERY
Chung F. Anesth Analg 1999; 89:
POSTOPERATIVE CHRONIC PAIN STATES - 1
Perkins, Kehlet. Chronic pain as an
POSTOPERATIVE CHRONIC PAIN STATES - 1
Perkins, Kehlet. Chronic pain as an
POSTOPERATIVE CHRONIC PAIN STATES - 2
Perkins, Kehlet. Chronic pain as an
POSTOPERATIVE CHRONIC PAIN STATES - 2
Perkins, Kehlet. Chronic pain as an
PAIN PHYSIOLOGY REVIEW
Potential sites of intervention
Peripheral nerve ending
Peripheral nerve transmission
Dorsal
PAIN PHYSIOLOGY REVIEW
Potential sites of intervention
Peripheral nerve ending
Peripheral nerve transmission
Dorsal
PERIPHERAL NERVE ENDINGS
Pain receptor (nociceptor) stimulation
Incision, traction, cutting, pressure
Nociceptor sensitization
Inflammatory mediators
Primary
PERIPHERAL NERVE ENDINGS
Pain receptor (nociceptor) stimulation
Incision, traction, cutting, pressure
Nociceptor sensitization
Inflammatory mediators
Primary
PERIPHERAL NERVE TRANSMISSION
Normal
A-δ fibers (sharp) + c-fibers (dull)
70-90% of peripheral nerve;
PERIPHERAL NERVE TRANSMISSION
Normal
A-δ fibers (sharp) + c-fibers (dull)
70-90% of peripheral nerve;
DORSAL HORN
Termination of nociceptor input
Lamina I – A-δ fibers
Lamina II (substantia
DORSAL HORN
Termination of nociceptor input
Lamina I – A-δ fibers
Lamina II (substantia
SPINAL CORD
Ascending tracts
Supraspinal reflexes – surgical stress response
Descending tracts
Opioids, α2-agonists
Spinal cord
SPINAL CORD
Ascending tracts
Supraspinal reflexes – surgical stress response
Descending tracts
Opioids, α2-agonists
Spinal cord
OPIOID HYPERALGESIA
Vinik. Anesth Analg 1998;86:1307
Rapid Development of Tolerance to Analgesia during
OPIOID HYPERALGESIA
Vinik. Anesth Analg 1998;86:1307
Rapid Development of Tolerance to Analgesia during
PREVENT OPIOID HYPERALGESIA
Luginbuhl. Anesth Analg 2003;96:726
Modulation of Remifentanil-induced Analgesia, Hyperalgesia, and
PREVENT OPIOID HYPERALGESIA
Luginbuhl. Anesth Analg 2003;96:726
Modulation of Remifentanil-induced Analgesia, Hyperalgesia, and
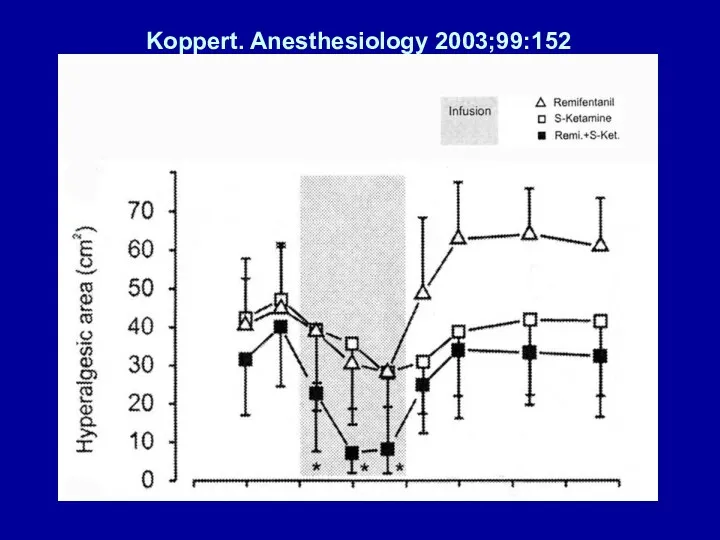
Koppert. Anesthesiology 2003;99:152
Koppert. Anesthesiology 2003;99:152
WOUND INFILTRATION – BLOCK NERVE ENDINGS
REGIONAL ANESTHESIA –
BLOCK NERVE
WOUND INFILTRATION – BLOCK NERVE ENDINGS REGIONAL ANESTHESIA – BLOCK NERVE
WOUND INFILTRATION – BLOCK NERVE ENDINGS
Bianconi. Anesth Analg 2004; 98:166
Pharmacokinetics &
WOUND INFILTRATION – BLOCK NERVE ENDINGS
Bianconi. Anesth Analg 2004; 98:166
Pharmacokinetics &
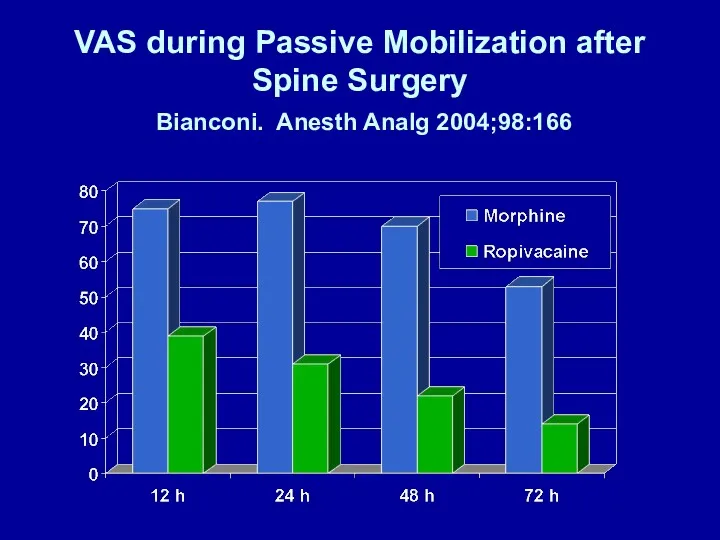
VAS during Passive Mobilization after Spine Surgery
Bianconi. Anesth Analg 2004;98:166
VAS during Passive Mobilization after Spine Surgery
Bianconi. Anesth Analg 2004;98:166
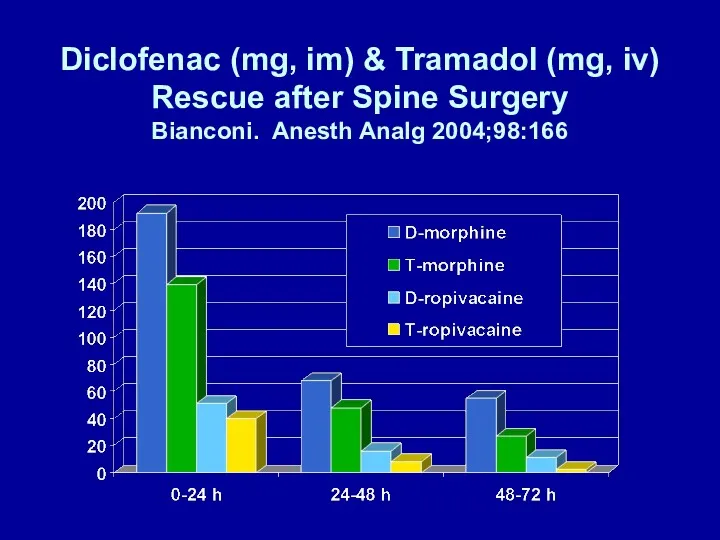
Diclofenac (mg, im) & Tramadol (mg, iv) Rescue after Spine Surgery
Bianconi.
Diclofenac (mg, im) & Tramadol (mg, iv) Rescue after Spine Surgery Bianconi.
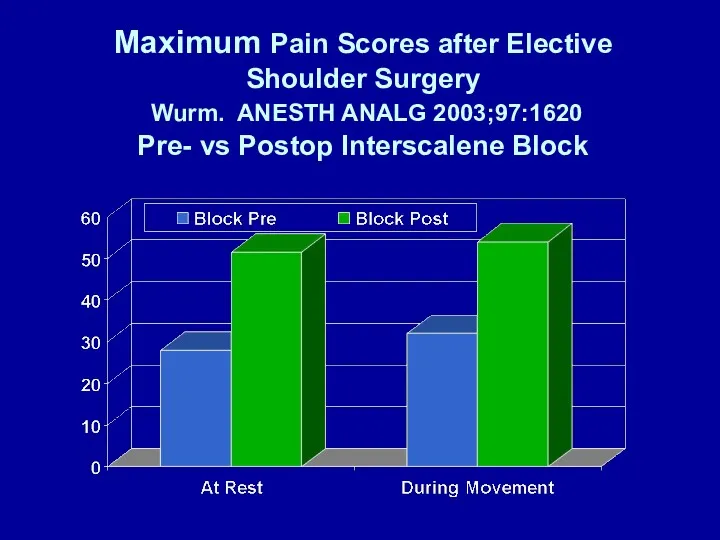
Maximum Pain Scores after Elective Shoulder Surgery
Wurm. ANESTH ANALG 2003;97:1620
Maximum Pain Scores after Elective Shoulder Surgery Wurm. ANESTH ANALG 2003;97:1620
REGIONAL ANALGESIA initiated during surgery DECREASES OPIOID DEMAND after inpatient surgery
Wang.
REGIONAL ANALGESIA initiated during surgery DECREASES OPIOID DEMAND after inpatient surgery
Wang.
LIMIT SPINAL CORD WIND-UP
NMDA antagonists
Magnesium
Ketamine
NSAIDS
Local anesthetics iv
LIMIT SPINAL CORD WIND-UP
NMDA antagonists
Magnesium
Ketamine
NSAIDS
Local anesthetics iv
Ketamine: Pre-incision vs. Pre-emergence
Fu. Anesth Analg 1997; 84:1086
Ketamine administration
Pre-incision group
0.5
Ketamine: Pre-incision vs. Pre-emergence
Fu. Anesth Analg 1997; 84:1086
Ketamine administration
Pre-incision group
0.5
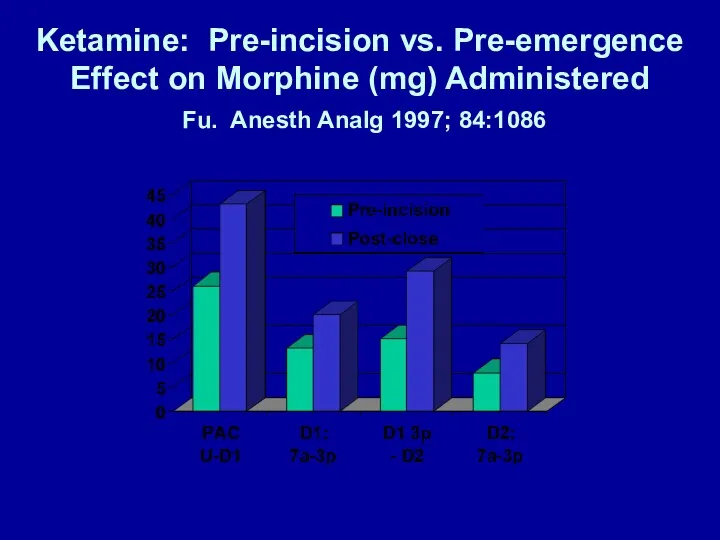
Ketamine: Pre-incision vs. Pre-emergence
Effect on Morphine (mg) Administered
Fu. Anesth Analg
Ketamine: Pre-incision vs. Pre-emergence Effect on Morphine (mg) Administered Fu. Anesth Analg
Intraoperative MgSO4 Reduces Fentanyl Requirements During and After Knee Arthroscopy
Konig. Anesth
Intraoperative MgSO4 Reduces Fentanyl Requirements During and After Knee Arthroscopy
Konig. Anesth
Effect of MgSO4 on Fentanyl Administration (μg/kg/min)
Konig. Anesth Analg 1998;87:206
Effect of MgSO4 on Fentanyl Administration (μg/kg/min)
Konig. Anesth Analg 1998;87:206
MgSO4 30 mg/kg + Ketamine 0.15 mg/kg
Gynecologic Surgery
Lo. Anesthesiology 1998;
MgSO4 30 mg/kg + Ketamine 0.15 mg/kg Gynecologic Surgery Lo. Anesthesiology 1998;
Liu. Anesth Analg 2001;92:1173
Super-additive Interactions between
Ketamine and Mg2+ at NMDA
Liu. Anesth Analg 2001;92:1173
Super-additive Interactions between
Ketamine and Mg2+ at NMDA
NMDA ANTAGONISTS - MAGNESIUM
O’Flaherty, et al. A-1265
Pain after tonsillectomy, 40 patients
NMDA ANTAGONISTS - MAGNESIUM
O’Flaherty, et al. A-1265
Pain after tonsillectomy, 40 patients
NEUROMUSCULAR BLOCKADE & Mg2+
Fuchs-Buder. Br J Anaesth 1995; 74:405
Mg2+ 40 mg/kg
Reduces
NEUROMUSCULAR BLOCKADE & Mg2+
Fuchs-Buder. Br J Anaesth 1995; 74:405
Mg2+ 40 mg/kg
Reduces
NMDA ANTAGONISTS - METHADONE
Byas-Smith, et al. Methadone produces greater reduction than
NMDA ANTAGONISTS - METHADONE
Byas-Smith, et al. Methadone produces greater reduction than
PREOPERATIVE ADMINISTRATION OF ORAL NSAIDS DECREASES POSTOPERATIVE ANALGESIC DEMANDS
Sinatra. Anesth Analg
PREOPERATIVE ADMINISTRATION OF ORAL NSAIDS DECREASES POSTOPERATIVE ANALGESIC DEMANDS
Sinatra. Anesth Analg
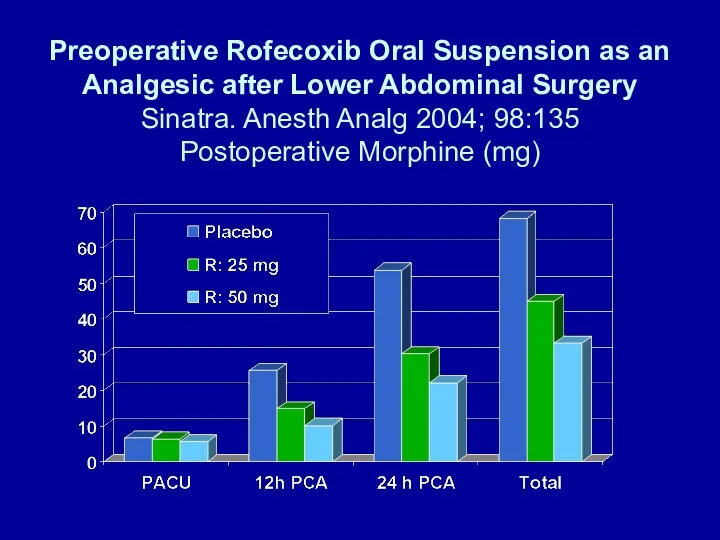
Preoperative Rofecoxib Oral Suspension as an Analgesic after Lower Abdominal Surgery
Sinatra.
Preoperative Rofecoxib Oral Suspension as an Analgesic after Lower Abdominal Surgery Sinatra.
Buvendendran. JAMA 2003;290:2411
Anesthesia for TKR
Epidural bupivacaine/fentanyl + propofol
“Traditional analgesia” (VAS <
Buvendendran. JAMA 2003;290:2411
Anesthesia for TKR
Epidural bupivacaine/fentanyl + propofol
“Traditional analgesia” (VAS <
Buvendendran. JAMA 2003;290:2411
Rofecoxib group (vs placebo)
Less opioid asked for – PCEA
Buvendendran. JAMA 2003;290:2411
Rofecoxib group (vs placebo)
Less opioid asked for – PCEA
IV LIDOCAINE - 1
Groudine. Anesth Analg 1998; 86:235-9
Radical retropubic prostatectomy, 64-yr-olds
Isoflurane-N2O-opioid
IV LIDOCAINE - 1
Groudine. Anesth Analg 1998; 86:235-9
Radical retropubic prostatectomy, 64-yr-olds
Isoflurane-N2O-opioid
IV LIDOCAINE - 2
Groudine. Anesth Analg 1998; 86:235-9
Postoperative advantages
Lower VAS pain
IV LIDOCAINE - 2
Groudine. Anesth Analg 1998; 86:235-9
Postoperative advantages
Lower VAS pain
Lidocaine (intraop) + Ketorolac (postop)
Groudine. Anesth Analg 1998; 86:235
Lidocaine (intraop) + Ketorolac (postop)
Groudine. Anesth Analg 1998; 86:235
IV LIDOCAINE - 3
Koppert. Anesthesiology 2000;93:A855
Abdominal surgery
Lidocaine: none vs 1.5 mg/kg/hr
IV LIDOCAINE - 3
Koppert. Anesthesiology 2000;93:A855
Abdominal surgery
Lidocaine: none vs 1.5 mg/kg/hr
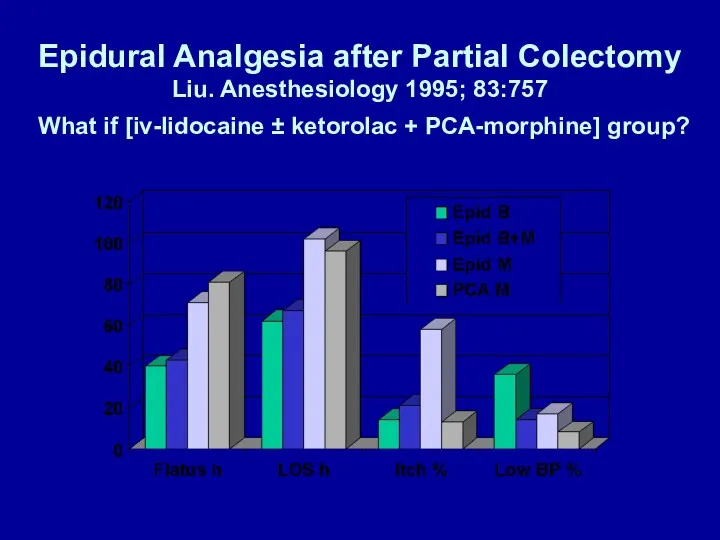
Epidural Analgesia after Partial Colectomy Liu. Anesthesiology 1995; 83:757
What if
Epidural Analgesia after Partial Colectomy Liu. Anesthesiology 1995; 83:757 What if
β-ADRENERGIC RECEPTOR ANTAGONISTS REDUCE POSTOPERATIVE OPIOID REQUIREMENTS
Zaugg. Anesthesiology 1999; 91:1674
White. Anesth
β-ADRENERGIC RECEPTOR ANTAGONISTS REDUCE POSTOPERATIVE OPIOID REQUIREMENTS
Zaugg. Anesthesiology 1999; 91:1674
White. Anesth
β-BLOCKERS REDUCE MORPHINE ADMINISTRATION
Zaugg. Anesthesiology 1999;91:1674
75-yr-olds, major abdominal surgery
Fentanyl-isoflurane anesthesia
Atenolol
β-BLOCKERS REDUCE MORPHINE ADMINISTRATION
Zaugg. Anesthesiology 1999;91:1674
75-yr-olds, major abdominal surgery
Fentanyl-isoflurane anesthesia
Atenolol
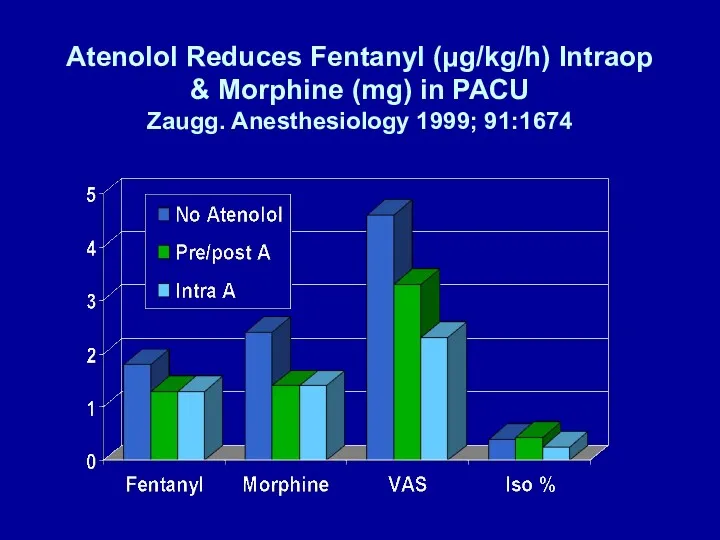
Atenolol Reduces Fentanyl (μg/kg/h) Intraop & Morphine (mg) in PACU
Zaugg. Anesthesiology
Atenolol Reduces Fentanyl (μg/kg/h) Intraop & Morphine (mg) in PACU Zaugg. Anesthesiology
Esmolol Infusion Intraop Reduces # of Patients Requiring Analgesia
White. Anesth
Esmolol Infusion Intraop Reduces # of Patients Requiring Analgesia White. Anesth
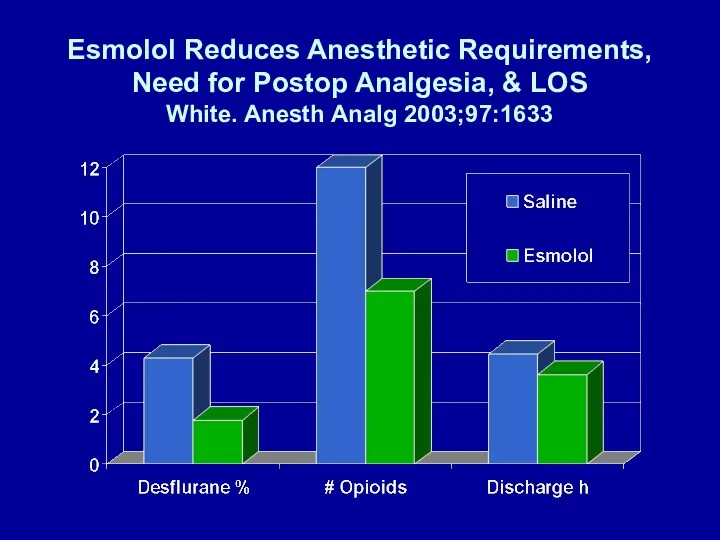
Esmolol Reduces Anesthetic Requirements, Need for Postop Analgesia, & LOS
White. Anesth
Esmolol Reduces Anesthetic Requirements, Need for Postop Analgesia, & LOS White. Anesth
DOES MUSIC AFFECT ANESTHESIA OR POSTOPERATIVE ANALGESIA?
Fentanyl (HR, BP), isoflurane (BIS
DOES MUSIC AFFECT ANESTHESIA OR POSTOPERATIVE ANALGESIA?
Fentanyl (HR, BP), isoflurane (BIS
DOES MUSIC AFFECT ANESTHESIA OR POSTOPERATIVE ANALGESIA?
No (patient-selected CD or Hemi-Sync)
Lumbar
DOES MUSIC AFFECT ANESTHESIA OR POSTOPERATIVE ANALGESIA?
No (patient-selected CD or Hemi-Sync)
Lumbar
SUMMARY
Considerable research activity addressing
Basic - new pain mechanisms
Translational - new drugs
SUMMARY
Considerable research activity addressing
Basic - new pain mechanisms
Translational - new drugs
WHAT DO I DO DIFFFERENTLY?
If general anesthesia and not regional
WHAT DO I DO DIFFFERENTLY?
If general anesthesia and not regional

WOUND INFILTRATION VS. SYSTEMIC LOCAL ANESTHETICS
EMLA CREAM -> DECREASED POSTOPERATIVE PAIN
Fassoulaki,
WOUND INFILTRATION VS. SYSTEMIC LOCAL ANESTHETICS
EMLA CREAM -> DECREASED POSTOPERATIVE PAIN
Fassoulaki,
α-ADRENERGIC RECEPTOR AGONISTS REDUCE POSTOPERATIVE OPIOID REQUIREMENTS
Locus ceruleus (sedation)
Dorsal horn (analgesia)
Arain.
α-ADRENERGIC RECEPTOR AGONISTS REDUCE POSTOPERATIVE OPIOID REQUIREMENTS
Locus ceruleus (sedation)
Dorsal horn (analgesia)
Arain.
 Антибиотиктер. Алкалоидтар. Гормондар
Антибиотиктер. Алкалоидтар. Гормондар Обеспечение безопасности пациентов. Обеспечение психологической безопасности в чрезвычайных ситуациях на уровне врача
Обеспечение безопасности пациентов. Обеспечение психологической безопасности в чрезвычайных ситуациях на уровне врача Пренатальді генетикалық зерттеулер
Пренатальді генетикалық зерттеулер Морфология органов мочевыделительной системы
Морфология органов мочевыделительной системы Общие закономерности токсикокинетики
Общие закономерности токсикокинетики Стоматология Денталия
Стоматология Денталия Основные принципы организации хирургической помощи населению в ЧС
Основные принципы организации хирургической помощи населению в ЧС Шок: патогенез, классификация, клиника, лечение
Шок: патогенез, классификация, клиника, лечение Острый рассеянный энцефаломиелит
Острый рассеянный энцефаломиелит Строение печени. Портальная гипертензия. Цирроз печени
Строение печени. Портальная гипертензия. Цирроз печени Критические периоды в ходе онтогенеза человека. Пагубное влияние на развитие плода лекарственных препаратов, алкоголя, никотина
Критические периоды в ходе онтогенеза человека. Пагубное влияние на развитие плода лекарственных препаратов, алкоголя, никотина Методы индивидуальной и коммунальной профилактики стом заболеваний у детей и взрослых
Методы индивидуальной и коммунальной профилактики стом заболеваний у детей и взрослых Основы питания при снижении массы тела
Основы питания при снижении массы тела Хронический холецистит
Хронический холецистит Двигательная система
Двигательная система Легочное сердце
Легочное сердце Базовое реанимационное пособие при поражении электричеством и молнией
Базовое реанимационное пособие при поражении электричеством и молнией Пневмонии у детей
Пневмонии у детей Показания и противопоказания переливания крови. Способы, виды, методы переливания. Осложнения и профилактика
Показания и противопоказания переливания крови. Способы, виды, методы переливания. Осложнения и профилактика Аппаратная косметология лица и тела
Аппаратная косметология лица и тела Снижение веса. Таблица продуктов со скрытым сахаром
Снижение веса. Таблица продуктов со скрытым сахаром Коматозные состояния
Коматозные состояния Чешуйчатый лишай (псориаз)
Чешуйчатый лишай (псориаз) Открытые повреждения. Раны, ожоги, отморожения
Открытые повреждения. Раны, ожоги, отморожения Синдромы и методы функциональной диагностики при патологии ЖВП и печени
Синдромы и методы функциональной диагностики при патологии ЖВП и печени Медикаментозные средства, используемые при реанимационных мероприятиях. Постреанимационная болезнь
Медикаментозные средства, используемые при реанимационных мероприятиях. Постреанимационная болезнь Переношенная беременность
Переношенная беременность Перспективы использования доказательной медицины врачами общей практики
Перспективы использования доказательной медицины врачами общей практики