- The problem of multiple sclerosis

Содержание
- 3. Multiple sclerosis (MS) also known as disseminated sclerosis (DS).
- 4. This nosology was first described in 1868 by French neurologist Jean-Martin Charcot.
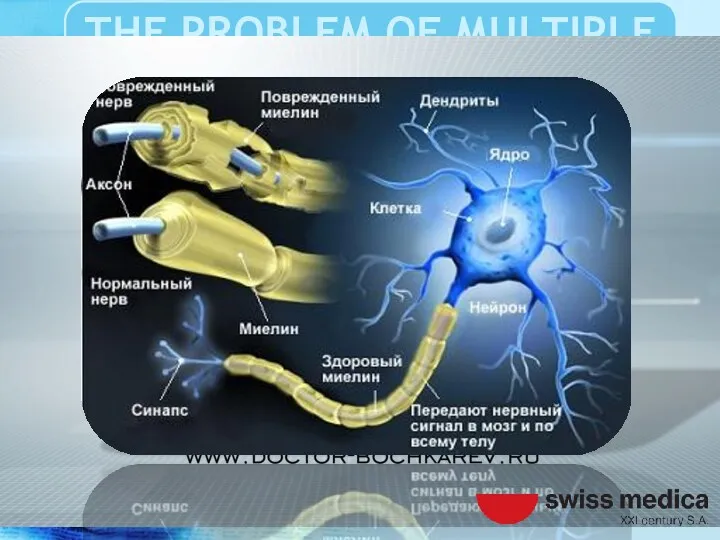
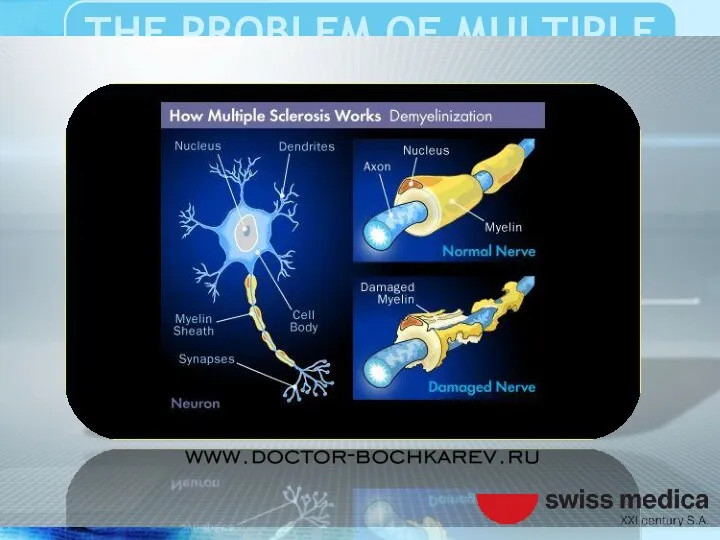
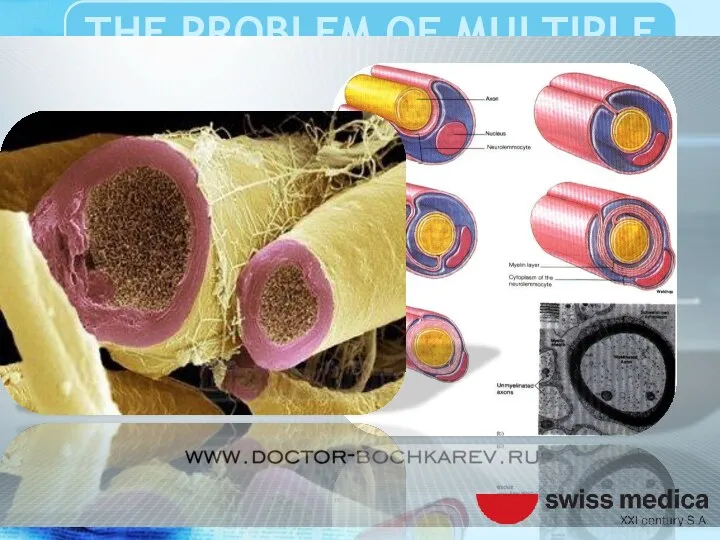
- 5. MS is a demyelinating disease of the central nervous system.
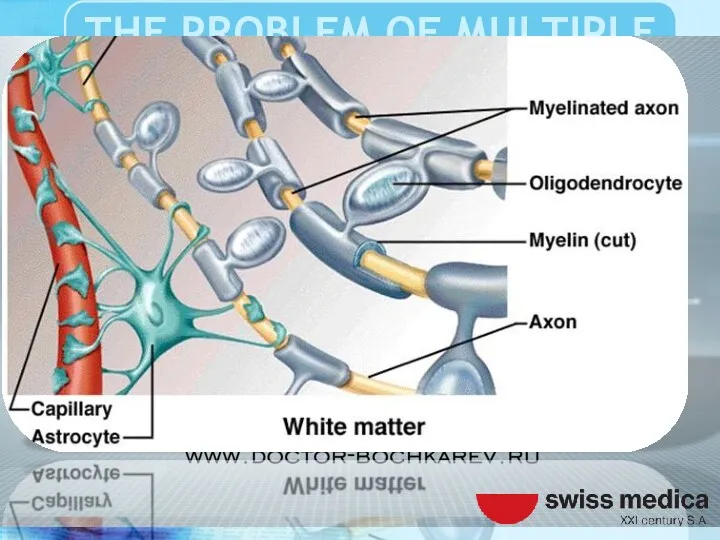
- 6. That affects the myelin sheath oligodendrocytes, glial cells covering the axons of the neurons of the
- 8. Violation of axonal conduction results in loss of the ability to communicate the different structures of
- 9. As a result, there are various neurological and psychiatric symptoms and syndromes, the totality of which
- 10. Manifestations of MS can be very diverse from the mental and intellectual disorders to gross motor,
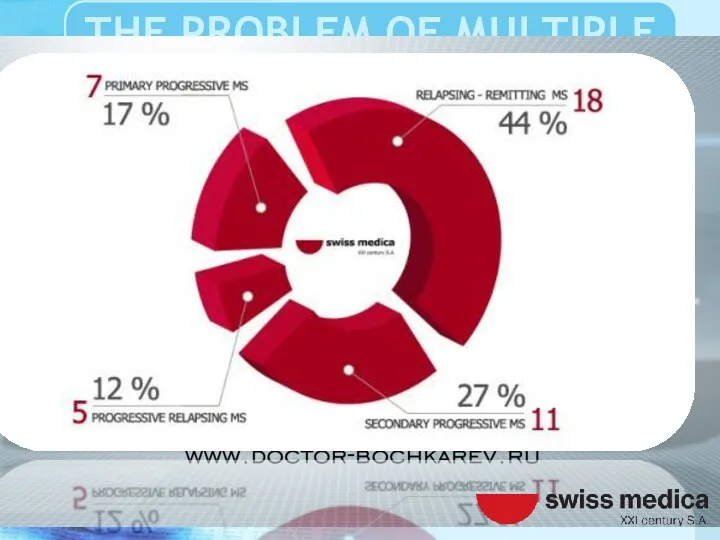
- 14. Disseminated sclerosis (DS) has several major clinical forms of the disease, in which the dynamics of
- 15. The debut of the disease or the emergence, new pathological symptoms, and after that her smooth
- 16. Between attacks, symptoms may disappear completely. However, permanent neurologic deficit is very characteristic of the disease.
- 17. The progression of old symptoms, the growth and the emergence of new, more typical of the
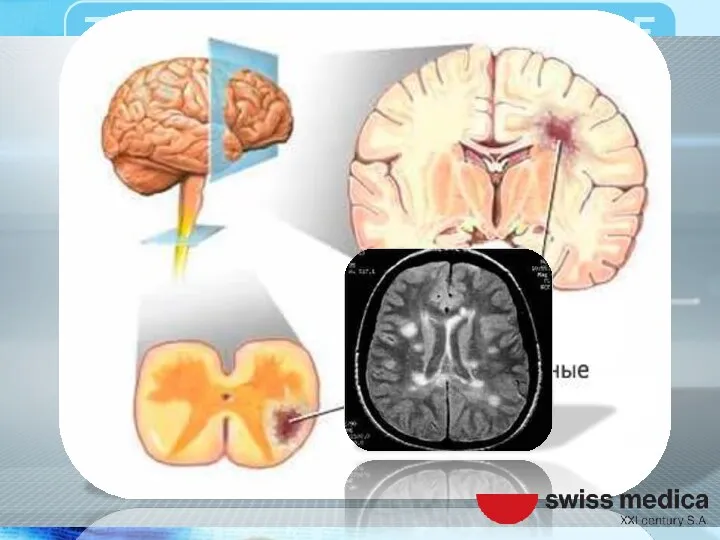
- 18. Multiple Sclerosis dispersed in space and time, as the demyelinating lesions scattered in the space of
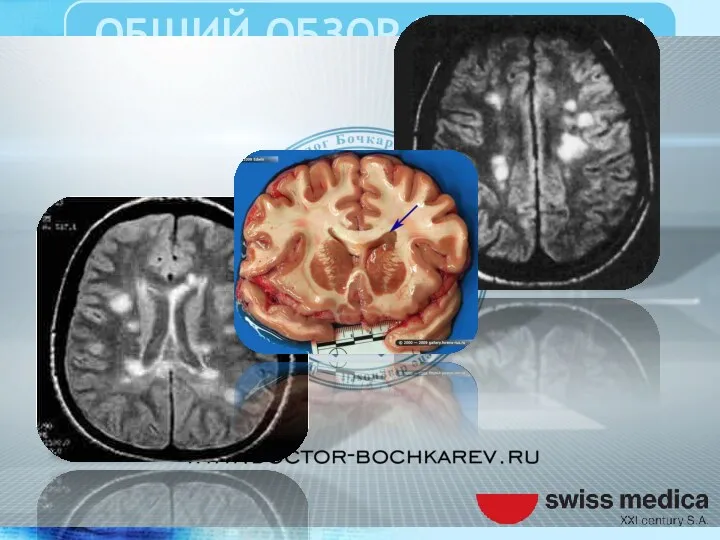
- 19. The name "multiple sclerosis" is named because of the identified at postmortem autopsy specific multiple non-specifically
- 20. Sclerotic plaques of different sizes that have arisen as a consequence of autoimmune damage to the
- 23. The etiology of MS and the pathological mechanism of demyelination is not completely clear.
- 24. Presumably based on genetic predisposition, dysfunction of the immune system autoimmune aggression against myelin producing cells
- 27. The pathogenic substrate is a chronic T cell-induced autoimmune inflammation, in which the body’s own immune
- 28. Manifested perivascular infiltration of mononuclear cells, demyelination and axonal damage. Result of diffusion transmission and reactive
- 29. Lots gliosis and demyelination, distributed mainly in the white matter of the central nervous system, radiant
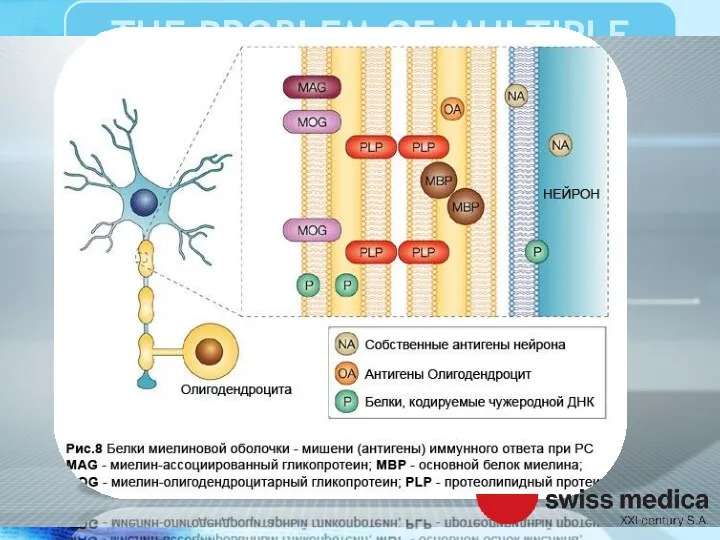
- 32. The disease destroys the myelin protein preferably belongs to the structure of the membrane of oligodendrocytes
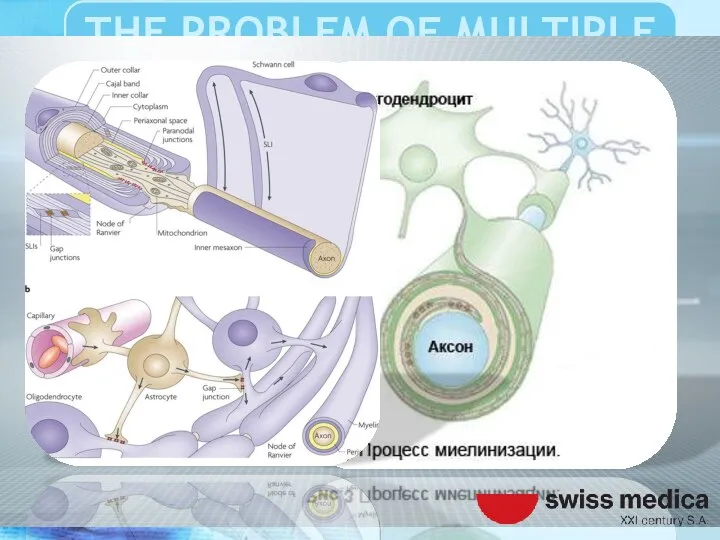
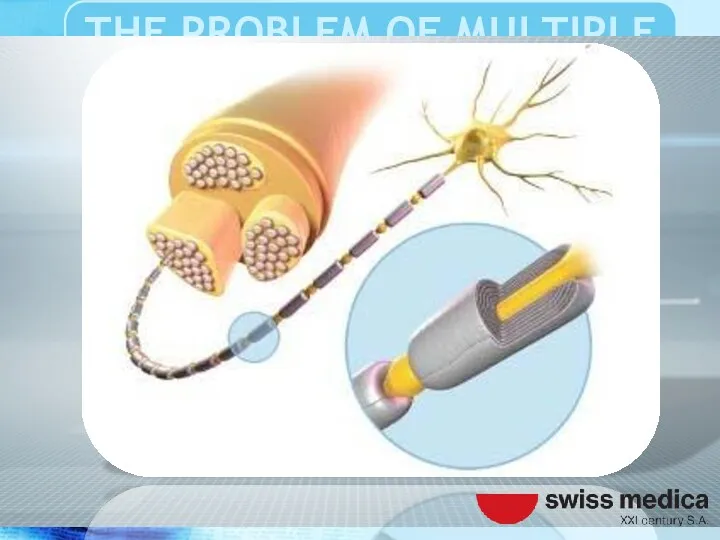
- 34. Oligodendrocytes are specialized glial cells involved in the transmission of nerve impulses and gain by which
- 35. The myelin sheath is necessary to complete the transmission (saltatory conducting) the bioelectric signals from the
- 37. The destruction of the myelin sheath leads to partial or complete blockade of the nerve impulse
- 40. Important role in the failure of immunity given to heredity, environmental factors and infections.
- 41. These factors according to various studies have a leading role in the development of autoimmune aggression
- 42. Also, some researchers play a key role in the development of autoimmune process, Ebstein-Barr virus.
- 44. The virus enters the body in early childhood and persists for a long time manifests infectious
- 46. Also noted the key patterns of response of the organism to various environmental influences.
- 47. In particular, patients with multiple sclerosis showed a decrease tolerance to the effects of solar radiation
- 48. Vitamin D deficiency, smoking tobacco may be additional triggers the development of multiple sclerosis
- 50. Multiple sclerosis is the most common autoimmune disease affecting the central nervous system.
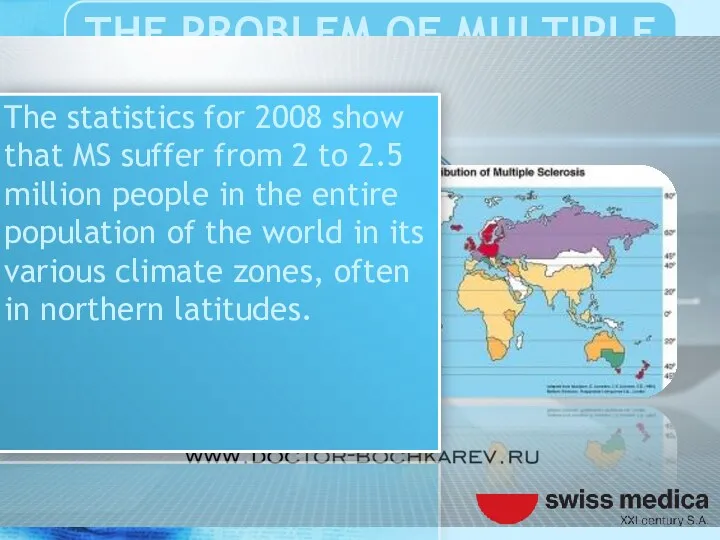
- 51. The statistics for 2008 show that MS suffer from 2 to 2.5 million people in the
- 52. There was a statistically upward trend in the incidence of MS. In 2013, 20,000 people died
- 53. At the same time in 1990 such cases were registered in 12000.
- 54. The disease usually debuts at the age of 20 to 50 years. Most earlier age groups.
- 55. Women suffer from MS almost twice as often as men. The life expectancy of an average
- 57. For the diagnosis of multiple sclerosis requires a detailed medical history, a thorough neurological examination with
- 58. Field selection of clinical symptoms and combining them into syndromes exhibit a preliminary diagnosis of the
- 59. To confirm the clinical apperception apply additional methods of diagnostics tools such as brain imaging, magnetic
- 60. MRI study demyelinating program (FLAIR - mode, T1-T2-weighted images, etc.
- 62. Then, a lumbar puncture and cerebrospinal fluid obtained is investigated for the presence of Monoclonal antibodies
- 63. For a more precise characterization demyelinating process of resorting to additional consultations related professionals such as
- 65. Neurophysiological research methods can be quite informative, even at the early onset of the disease, a
- 66. Progression of the disease leads to permanent disability, motor, sensory, mental and cognitive disorders.
- 68. Treatment of multiple sclerosis are not currently found.
- 69. Until the end is not clear pathophysiological mechanism of occurrence of the system demyelination. For this
- 70. However, modern medical science allows for effective palliative and symptomatic therapy.
- 71. Designed and tested international standards of treatment that aimed at improving the quality of life of
- 72. Strategic effect of therapy aims at reducing the recurrence of, reducing the number of attacks, increased
- 73. For these purposes at the current time successfully passed clinical trials and actively introducing modern medicines.
- 74. Treatment algorithms, individual approach to reparative regeneration and physiotherapy rehabilitation of patients with multiple sclerosis.
- 75. Tested and implemented new cutting-edge biotech treatments. Studies conducted in the field of regenerative medicine using
- 76. Of the currently available therapies advantageously used selective inhibition of autoimmune attack against the nervous system.
- 77. Used interferons, glucocorticoid hormones, various immunosuppressants including plasmapheresis. However, their use does not promote the regeneration
- 78. The therapy is aimed primarily improve lost function after CNS demyelinating attack, and to prevent new
- 79. Despite that medicines used to treat MS are ineffective, and usually have significant side effects which
- 80. Poorly tolerated, and vice versa worsen the quality of life of patients.
- 81. So many people suffer from MS often resort to alternative treatments, despite the lack of credible
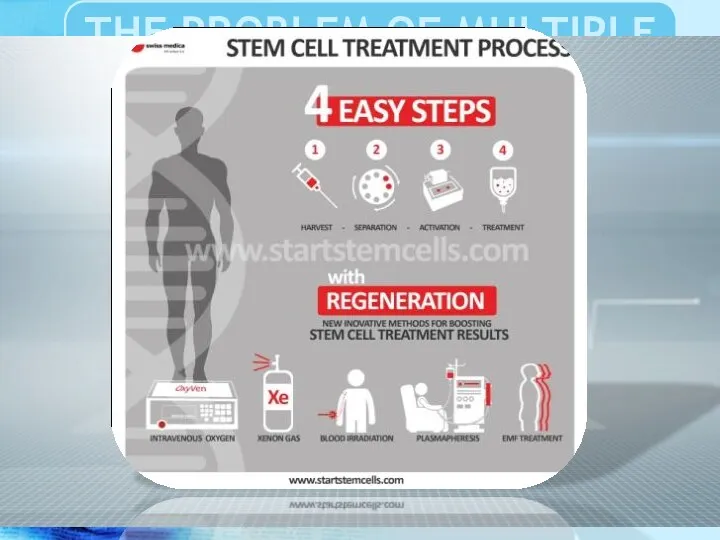
- 82. One of the most promising methods of treatment of multiple sclerosis is the use of stem
- 83. Studies on the use in the treatment of MS autologous stem cells show a positive therapeutic
- 84. Long-term results are difficult to predict good results stem from an alternative method of treatment is
- 86. Treatment in Swiss Medica Clinic showed that stromal stem cells administered intravenously cross the blood brain
- 87. This stem cell treatment leads to the replacement of damaged cells and the restoration of the
- 88. Until recently, it was believed that damaged brain tissue is permanent condition. Nowadays, the re-growth of
- 89. Swiss Medica Clinic has developed the Adult Autologous Stem Cell Therapy program to treat a variety
- 90. During stem cell treatment a patient receives 200 – 300 million stem cells. This quantity of
- 91. Thus the reserve of the stem cells, almost lost for the latest 15 – 20 years,
- 94. The goal of this MS Cumulative report is to assess the success of Stem cells treatment
- 98. M.Sc. PhD MD Bochkarev IA
- 100. Ascherio A, Munger KL (April 2007). "Environmental risk factors for multiple sclerosis. Part I: the role
- 102. Скачать презентацию
Multiple sclerosis (MS) also known as disseminated sclerosis (DS).
Multiple sclerosis (MS) also known as disseminated sclerosis (DS).
This nosology was first described in 1868 by French neurologist Jean-Martin
This nosology was first described in 1868 by French neurologist Jean-Martin
MS is a demyelinating disease of the central nervous system.
MS is a demyelinating disease of the central nervous system.
That affects the myelin sheath oligodendrocytes, glial cells covering the axons
That affects the myelin sheath oligodendrocytes, glial cells covering the axons

Violation of axonal conduction results in loss of the ability to
Violation of axonal conduction results in loss of the ability to
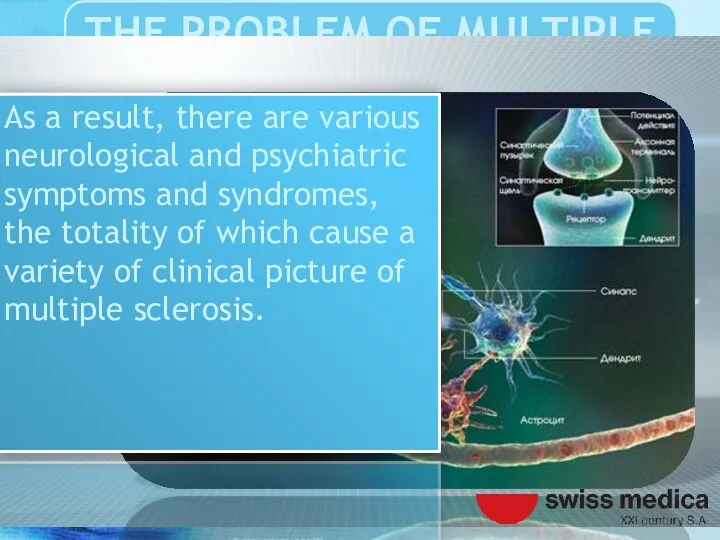
As a result, there are various neurological and psychiatric symptoms and
As a result, there are various neurological and psychiatric symptoms and
Manifestations of MS can be very diverse from the mental and
Manifestations of MS can be very diverse from the mental and
Disseminated sclerosis (DS) has several major clinical forms of the disease,
Disseminated sclerosis (DS) has several major clinical forms of the disease,
The debut of the disease or the emergence, new pathological symptoms,
The debut of the disease or the emergence, new pathological symptoms,
Between attacks, symptoms may disappear completely. However, permanent neurologic deficit is
Between attacks, symptoms may disappear completely. However, permanent neurologic deficit is
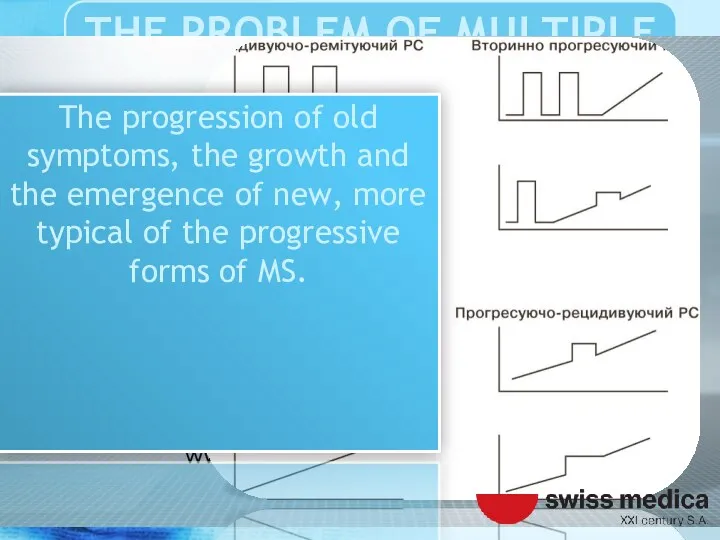
The progression of old symptoms, the growth and the emergence of
The progression of old symptoms, the growth and the emergence of
Multiple Sclerosis dispersed in space and time, as the demyelinating lesions
Multiple Sclerosis dispersed in space and time, as the demyelinating lesions
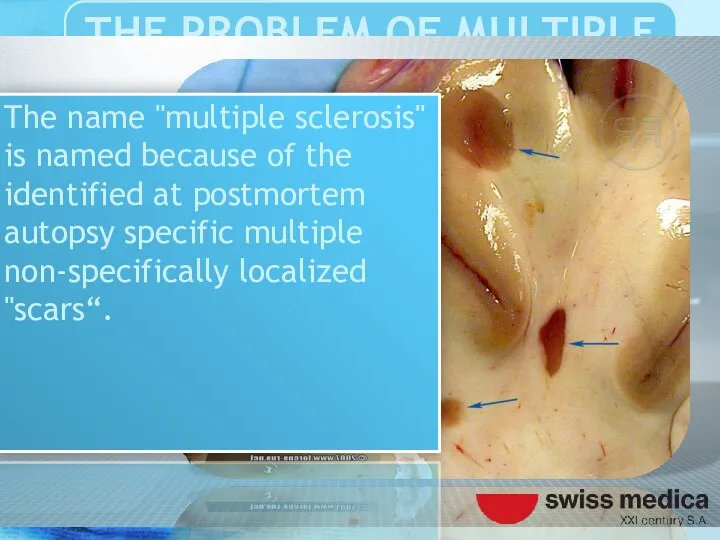
The name "multiple sclerosis" is named because of the identified at
The name "multiple sclerosis" is named because of the identified at
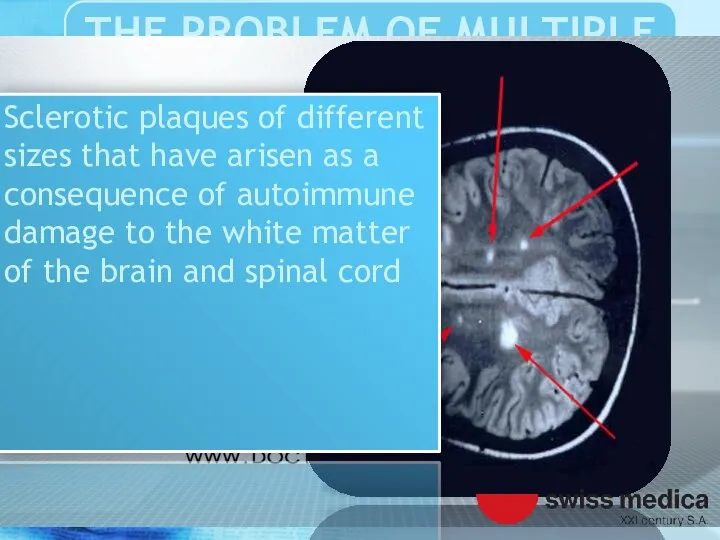
Sclerotic plaques of different sizes that have arisen as a consequence
Sclerotic plaques of different sizes that have arisen as a consequence
The etiology of MS and the pathological mechanism of demyelination is
The etiology of MS and the pathological mechanism of demyelination is
Presumably based on genetic predisposition, dysfunction of the immune system autoimmune
Presumably based on genetic predisposition, dysfunction of the immune system autoimmune
The pathogenic substrate is a chronic T cell-induced autoimmune inflammation, in
The pathogenic substrate is a chronic T cell-induced autoimmune inflammation, in
Manifested perivascular infiltration of mononuclear cells, demyelination and axonal damage. Result
Manifested perivascular infiltration of mononuclear cells, demyelination and axonal damage. Result
Lots gliosis and demyelination, distributed mainly in the white matter of
Lots gliosis and demyelination, distributed mainly in the white matter of
The disease destroys the myelin protein preferably belongs to the structure
The disease destroys the myelin protein preferably belongs to the structure
Oligodendrocytes are specialized glial cells involved in the transmission of nerve
Oligodendrocytes are specialized glial cells involved in the transmission of nerve
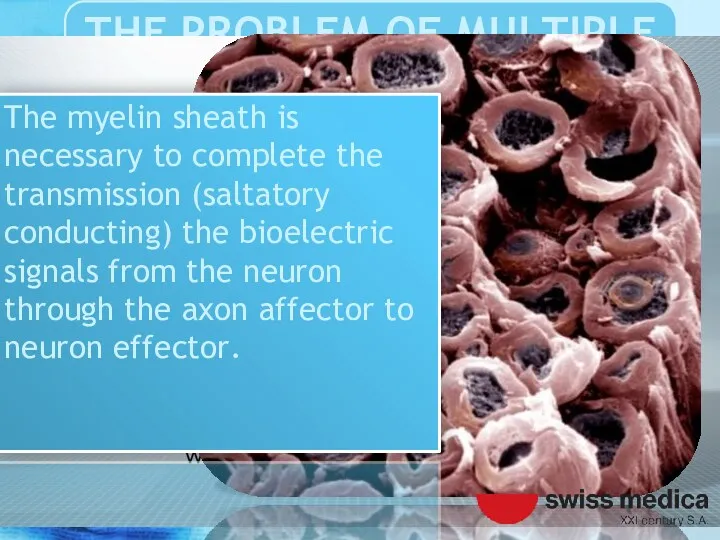
The myelin sheath is necessary to complete the transmission (saltatory conducting)
The myelin sheath is necessary to complete the transmission (saltatory conducting)
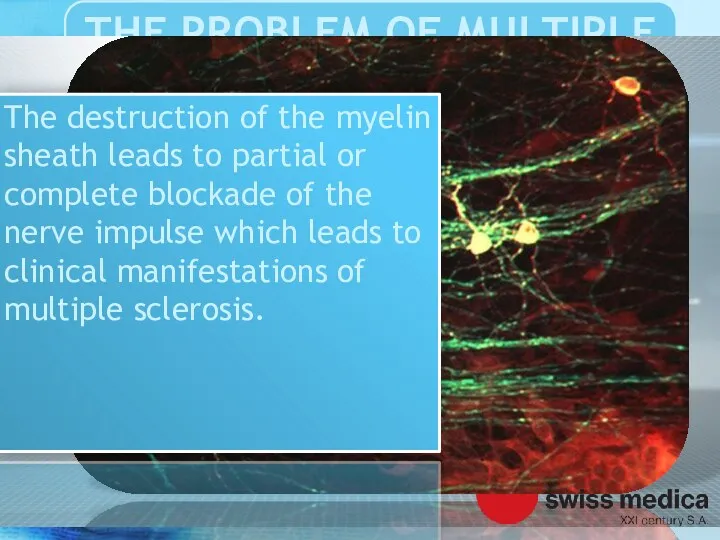
The destruction of the myelin sheath leads to partial or complete
The destruction of the myelin sheath leads to partial or complete
Important role in the failure of immunity given to heredity, environmental
Important role in the failure of immunity given to heredity, environmental
These factors according to various studies have a leading role in
These factors according to various studies have a leading role in
Also, some researchers play a key role in the development of
Also, some researchers play a key role in the development of
The virus enters the body in early childhood and persists for
The virus enters the body in early childhood and persists for

Also noted the key patterns of response of the organism
Also noted the key patterns of response of the organism
In particular, patients with multiple sclerosis showed a decrease tolerance to
In particular, patients with multiple sclerosis showed a decrease tolerance to
Vitamin D deficiency, smoking tobacco may be additional triggers the development
Vitamin D deficiency, smoking tobacco may be additional triggers the development
Multiple sclerosis is the most common autoimmune disease affecting the central
Multiple sclerosis is the most common autoimmune disease affecting the central
The statistics for 2008 show that MS suffer from 2 to
The statistics for 2008 show that MS suffer from 2 to
There was a statistically upward trend in the incidence of MS.
There was a statistically upward trend in the incidence of MS.
At the same time in 1990 such cases were registered in
At the same time in 1990 such cases were registered in
The disease usually debuts at the age of 20 to 50
The disease usually debuts at the age of 20 to 50
Women suffer from MS almost twice as often as men. The
Women suffer from MS almost twice as often as men. The
For the diagnosis of multiple sclerosis requires a detailed medical history,
For the diagnosis of multiple sclerosis requires a detailed medical history,
Field selection of clinical symptoms and combining them into syndromes exhibit
Field selection of clinical symptoms and combining them into syndromes exhibit
To confirm the clinical apperception apply additional methods of diagnostics tools
To confirm the clinical apperception apply additional methods of diagnostics tools
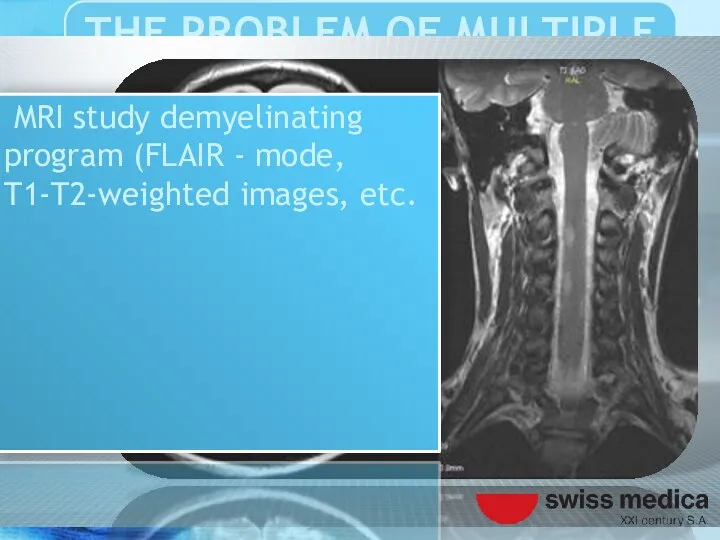
MRI study demyelinating program (FLAIR - mode, T1-T2-weighted images, etc.
MRI study demyelinating program (FLAIR - mode, T1-T2-weighted images, etc.
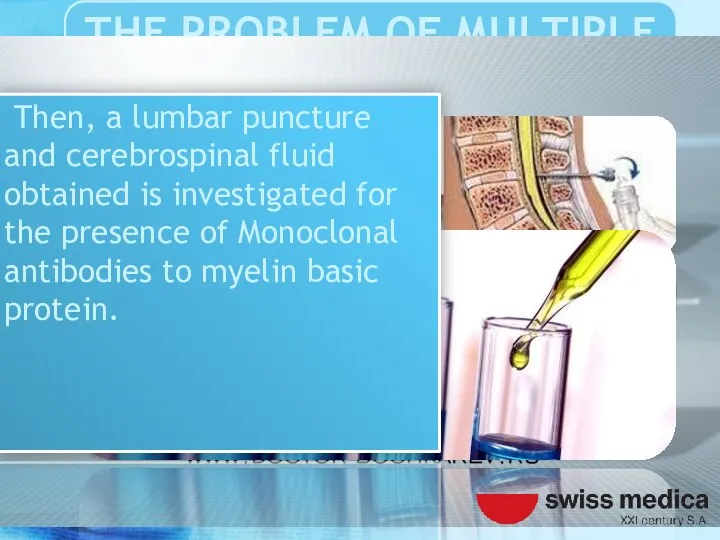
Then, a lumbar puncture and cerebrospinal fluid obtained is investigated
Then, a lumbar puncture and cerebrospinal fluid obtained is investigated
For a more precise characterization demyelinating process of resorting to
For a more precise characterization demyelinating process of resorting to
Neurophysiological research methods can be quite informative, even at the early
Neurophysiological research methods can be quite informative, even at the early
Progression of the disease leads to permanent disability, motor, sensory, mental
Progression of the disease leads to permanent disability, motor, sensory, mental
Treatment of multiple sclerosis are not currently found.
Treatment of multiple sclerosis are not currently found.
Until the end is not clear pathophysiological mechanism of occurrence of
Until the end is not clear pathophysiological mechanism of occurrence of
However, modern medical science allows for effective palliative and symptomatic therapy.
However, modern medical science allows for effective palliative and symptomatic therapy.
Designed and tested international standards of treatment that aimed at improving
Designed and tested international standards of treatment that aimed at improving
Strategic effect of therapy aims at reducing the recurrence of, reducing
Strategic effect of therapy aims at reducing the recurrence of, reducing
For these purposes at the current time successfully passed clinical trials
For these purposes at the current time successfully passed clinical trials
Treatment algorithms, individual approach to reparative regeneration and physiotherapy rehabilitation of
Treatment algorithms, individual approach to reparative regeneration and physiotherapy rehabilitation of
Tested and implemented new cutting-edge biotech treatments. Studies conducted in the
Tested and implemented new cutting-edge biotech treatments. Studies conducted in the
Of the currently available therapies advantageously used selective inhibition of autoimmune
Of the currently available therapies advantageously used selective inhibition of autoimmune
Used interferons, glucocorticoid hormones, various immunosuppressants including plasmapheresis. However, their use
Used interferons, glucocorticoid hormones, various immunosuppressants including plasmapheresis. However, their use
The therapy is aimed primarily improve lost function after CNS demyelinating
The therapy is aimed primarily improve lost function after CNS demyelinating
Despite that medicines used to treat MS are ineffective, and usually
Despite that medicines used to treat MS are ineffective, and usually
Poorly tolerated, and vice versa worsen the quality of life of
Poorly tolerated, and vice versa worsen the quality of life of
So many people suffer from MS often resort to alternative treatments,
So many people suffer from MS often resort to alternative treatments,
One of the most promising methods of treatment of multiple sclerosis
One of the most promising methods of treatment of multiple sclerosis
Studies on the use in the treatment of MS autologous stem
Studies on the use in the treatment of MS autologous stem
Long-term results are difficult to predict good results stem from an
Long-term results are difficult to predict good results stem from an
Treatment in Swiss Medica Clinic showed that stromal stem cells administered intravenously
Treatment in Swiss Medica Clinic showed that stromal stem cells administered intravenously
This stem cell treatment leads to the replacement of damaged cells
This stem cell treatment leads to the replacement of damaged cells
Until recently, it was believed that damaged brain tissue is permanent
Until recently, it was believed that damaged brain tissue is permanent
Swiss Medica Clinic has developed the Adult Autologous Stem Cell Therapy program
Swiss Medica Clinic has developed the Adult Autologous Stem Cell Therapy program
During stem cell treatment a patient receives 200 – 300 million
During stem cell treatment a patient receives 200 – 300 million
Thus the reserve of the stem cells, almost lost for the
Thus the reserve of the stem cells, almost lost for the

The goal of this MS Cumulative report is to assess the
The goal of this MS Cumulative report is to assess the


M.Sc. PhD MD Bochkarev IA
M.Sc. PhD MD Bochkarev IA
Ascherio A, Munger KL (April 2007). "Environmental risk factors for multiple
Ascherio A, Munger KL (April 2007). "Environmental risk factors for multiple
 Хронический холецистит. Желчнокаменная болезнь
Хронический холецистит. Желчнокаменная болезнь Нефротический синдром
Нефротический синдром Современные принципы антихеликобактерной терапии
Современные принципы антихеликобактерной терапии Гастростомия
Гастростомия Менингит. Классификация. Этиология. Патогенез. Клиника
Менингит. Классификация. Этиология. Патогенез. Клиника Первая помощь. Комплекс экстренных медицинских мероприятий
Первая помощь. Комплекс экстренных медицинских мероприятий Сердечно-сосудистые заболевания при ДТЗ
Сердечно-сосудистые заболевания при ДТЗ Программа добровольного медицинского страхования Доктор РЕСО. Новосибирск
Программа добровольного медицинского страхования Доктор РЕСО. Новосибирск Осложнения в ходе гинекологических операций
Осложнения в ходе гинекологических операций ВКР: Роль медицинской сестры в проведении реабилитационных мероприятий при заболеваниях органов дыхания у детей
ВКР: Роль медицинской сестры в проведении реабилитационных мероприятий при заболеваниях органов дыхания у детей Спорт и допинг
Спорт и допинг Моральные проблемы взаимоотношения врачей и ученых в процессе врачевания и научного исследования
Моральные проблемы взаимоотношения врачей и ученых в процессе врачевания и научного исследования Хронический гепатит
Хронический гепатит Психолого - педагогические закономерности развития и особенности детей с ОВЗ
Психолого - педагогические закономерности развития и особенности детей с ОВЗ Диуретики - мочегонные средства
Диуретики - мочегонные средства Лечение в Израиле
Лечение в Израиле Ауыр преэклампсия кезіндегі дәрігерге дейінгі күттірмейтін көмек көрсету алгоритімі
Ауыр преэклампсия кезіндегі дәрігерге дейінгі күттірмейтін көмек көрсету алгоритімі Выделительная система
Выделительная система Дезинфекция: виды, методы, режимы
Дезинфекция: виды, методы, режимы Особиста програма зміцнення здоров’я
Особиста програма зміцнення здоров’я Phylogenetic disorders of respiratory system
Phylogenetic disorders of respiratory system ОРВИ и грипп
ОРВИ и грипп Атрезия пищевода
Атрезия пищевода Бактериальные и паразитарные абсцессы печени. Кисты печени (паразитарные и непаразитарные)
Бактериальные и паразитарные абсцессы печени. Кисты печени (паразитарные и непаразитарные) Изменения кожи при сахарном диабете
Изменения кожи при сахарном диабете Боль в спине
Боль в спине Профессиональное выгорание среди медицинских работников: связь с ошибками и качеством медицинской помощи
Профессиональное выгорание среди медицинских работников: связь с ошибками и качеством медицинской помощи Панкреонекроз
Панкреонекроз