- The treatment of Lobular Pneumonia

Содержание
- 2. Pneumonia is an inflammation of the lung, usually caused by bacteria, viruses or protozoa. If the
- 5. Pneumonia: infecting organisms in approximate descending order of frequency Community acquired Streptococcus pneumoniae Mycoplasma pneumoniae Influenza
- 7. The usual clinical presentation in pneumonia caused by Streptococcus pneumoniae is acute, with the abrupt onset
- 8. Pneumococci are typically asociated with pneumonia
- 9. Lobar pneumonia: stage of onset Morphology. Congestion stage — extensive serous exudation, vascular engorgement, rapid bacterial
- 10. Lobar pneumonia: stage of consolidation Morphology. Red hepatization stage — airspaces are filled with PMN cells,
- 12. Lobar pneumonia: stage of resolution Morphology. Resolution stage — resorption of the exudate. Inspection. The patient
- 14. Complications Lung abscess Pleurisy Toxic shock Myocarditis
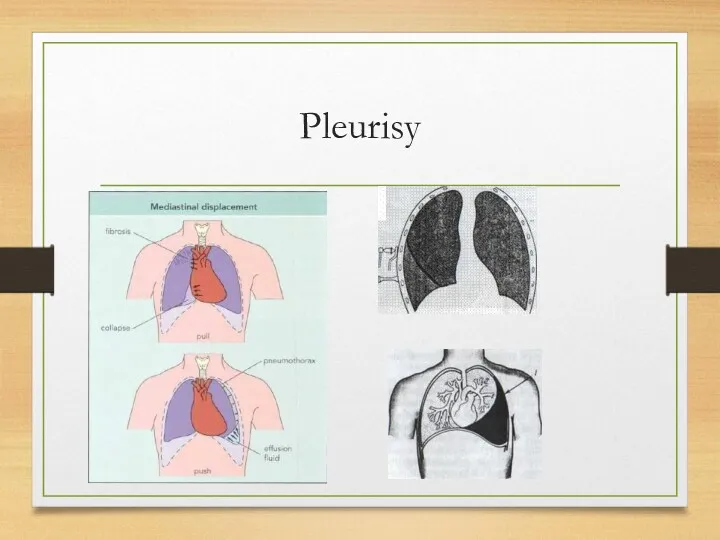
- 15. Pleurisy
- 16. Pleurisy with effusion: a-anterior view; b—posterior view: 1—Damoiseau's curve; 2—Garland's triangle; 3—Rauchfuss-Grocco triangle.
- 17. Mycoplasma pneumoniae is the most common cause of the «atypical» pneumonias. Infection usually occurs in older
- 18. Staphylococcal pneumonia typically occurs as a complication of influenza, especially in the elderly and, although uncommon,
- 19. Legionnaires' disease is pneumonia caused by Le-gionella pneumophila. Infection is most common in debilitated or immunocompromised
- 20. Aspiration pneumonia results from the aspiration of gastric contents into the lung and is associated with
- 21. Treatment of all pneumonias should be started immediately and the antibiotic chosen should be the «best
- 22. Infection in the immunocompromised host There has been a steady increase in the number of patients
- 23. Pneumocystis carinii is the most important cause of fatal pneumonia in immunosuppressed patients. It is believed
- 24. In Pneumocystis carinii pneumonia the changes on X-ray may be very minor, but the patient is
- 25. Principles of treatment Antibiotics Expectorants Desintoxication Oxygen Antigistamine agents Symptomatic therapy
- 27. Скачать презентацию
Pneumonia is an inflammation of the lung, usually caused by bacteria,
Pneumonia is an inflammation of the lung, usually caused by bacteria,

Pneumonia: infecting organisms in approximate descending order of frequency
Community acquired
Streptococcus pneumoniae
Mycoplasma
Pneumonia: infecting organisms in approximate descending order of frequency
Community acquired
Streptococcus pneumoniae
Mycoplasma

The usual clinical presentation in pneumonia caused by Streptococcus pneumoniae is
The usual clinical presentation in pneumonia caused by Streptococcus pneumoniae is
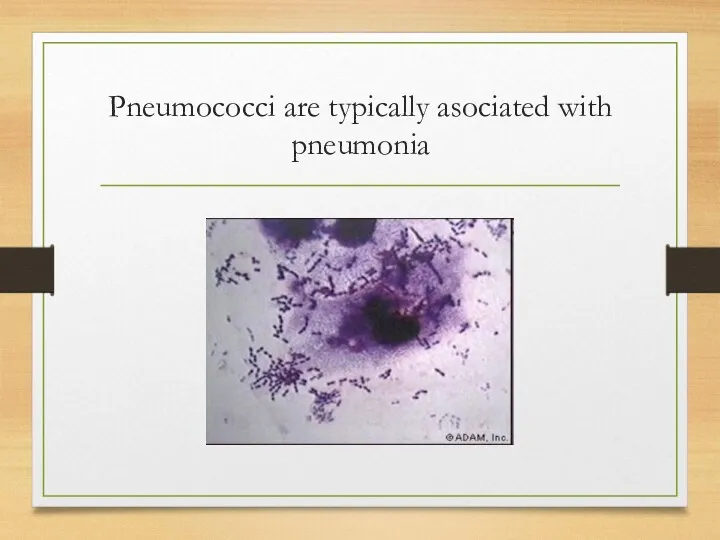
Pneumococci are typically asociated with pneumonia
Pneumococci are typically asociated with pneumonia
Lobar pneumonia: stage of onset
Morphology. Congestion stage — extensive serous exudation,
Lobar pneumonia: stage of onset
Morphology. Congestion stage — extensive serous exudation,
Lobar pneumonia: stage of consolidation
Morphology. Red hepatization stage — airspaces are
Lobar pneumonia: stage of consolidation
Morphology. Red hepatization stage — airspaces are

Lobar pneumonia: stage of resolution
Morphology. Resolution stage — resorption of the
Lobar pneumonia: stage of resolution
Morphology. Resolution stage — resorption of the


Complications
Lung abscess
Pleurisy
Toxic shock
Myocarditis
Complications
Lung abscess
Pleurisy
Toxic shock
Myocarditis
Pleurisy
Pleurisy
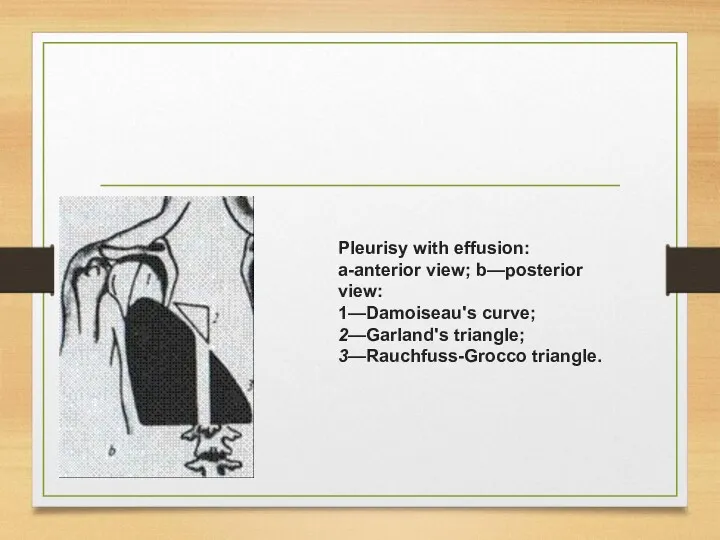
Pleurisy with effusion: a-anterior view; b—posterior view:
1—Damoiseau's curve; 2—Garland's triangle;
3—Rauchfuss-Grocco triangle.
Pleurisy with effusion: a-anterior view; b—posterior view:
1—Damoiseau's curve; 2—Garland's triangle;
3—Rauchfuss-Grocco triangle.

Mycoplasma pneumoniae is the most common cause of the «atypical» pneumonias.
Mycoplasma pneumoniae is the most common cause of the «atypical» pneumonias.
Staphylococcal pneumonia typically occurs as a complication of influenza, especially in
Staphylococcal pneumonia typically occurs as a complication of influenza, especially in
Legionnaires' disease is pneumonia caused by Le-gionella pneumophila. Infection is most
Legionnaires' disease is pneumonia caused by Le-gionella pneumophila. Infection is most
Aspiration pneumonia results from the aspiration of gastric contents into the
Aspiration pneumonia results from the aspiration of gastric contents into the
Treatment of all pneumonias should be started immediately and the antibiotic
Treatment of all pneumonias should be started immediately and the antibiotic
Infection in the immunocompromised host
There has been a steady increase in
Infection in the immunocompromised host
There has been a steady increase in
Pneumocystis carinii is the most important cause of fatal pneumonia in
Pneumocystis carinii is the most important cause of fatal pneumonia in
In Pneumocystis carinii pneumonia the changes on X-ray may be very
In Pneumocystis carinii pneumonia the changes on X-ray may be very

Principles of treatment
Antibiotics
Expectorants
Desintoxication
Oxygen
Antigistamine agents
Symptomatic therapy
Principles of treatment
Antibiotics
Expectorants
Desintoxication
Oxygen
Antigistamine agents
Symptomatic therapy
 Шигеллы
Шигеллы Функциональная морфология мочевыделительной системы человека. (Лекция 3)
Функциональная морфология мочевыделительной системы человека. (Лекция 3) Общая реакция организма на травму
Общая реакция организма на травму Герметизация фиссур
Герметизация фиссур Жарақаттан болатын шок. Жарақаттан болатын асфиксия. Жарақаттан болатын токсикоз
Жарақаттан болатын шок. Жарақаттан болатын асфиксия. Жарақаттан болатын токсикоз Methods of examination in gynecology
Methods of examination in gynecology Temperature curves. Fever
Temperature curves. Fever Патофизиология паращитовидных желез
Патофизиология паращитовидных желез Анатомия сердца. Первая медицинская помощь при ранах и кровотечения
Анатомия сердца. Первая медицинская помощь при ранах и кровотечения Новокаиновая блокада
Новокаиновая блокада Физиология сенсорных систем
Физиология сенсорных систем Травми опорно-рухової системи
Травми опорно-рухової системи Особенности оказания помощи при экстремальных воздействиях. Медицина катастроф. Тема 3
Особенности оказания помощи при экстремальных воздействиях. Медицина катастроф. Тема 3 Лабораторная диагностика при критических состояниях
Лабораторная диагностика при критических состояниях Определение туберкулеза. Эпидемиология, этиология, патогенез, Иммунитет при туберкулезе. (Лекция 1)
Определение туберкулеза. Эпидемиология, этиология, патогенез, Иммунитет при туберкулезе. (Лекция 1) Актуальные вопросы диспансеризации
Актуальные вопросы диспансеризации Врожденные пороки развития гортани и трахеи
Врожденные пороки развития гортани и трахеи Медицинские приборно-компьютерные системы клинического мониторинга. (Лекция 6)
Медицинские приборно-компьютерные системы клинического мониторинга. (Лекция 6) Синдром красного глаза без снижения зрительных функций
Синдром красного глаза без снижения зрительных функций Вирус полиомиелита
Вирус полиомиелита Обследование больных с патологией сердечно-сосудистой системы. Расспрос, осмотр, пальпация сердечной области. (Лекция 6)
Обследование больных с патологией сердечно-сосудистой системы. Расспрос, осмотр, пальпация сердечной области. (Лекция 6) Сбалансированное питание. Жиры. Главные функции жиров
Сбалансированное питание. Жиры. Главные функции жиров Субпопуляции Т-лимфоцитов
Субпопуляции Т-лимфоцитов Надання допомоги пораненим під час бойових дій
Надання допомоги пораненим під час бойових дій Сестринские манипуляции. Разведение антибиотиков
Сестринские манипуляции. Разведение антибиотиков Трихология. Функции волосяного покрова
Трихология. Функции волосяного покрова Экзистенциальные вопросы умирающих
Экзистенциальные вопросы умирающих Диагностика и коррекция нарушения зрения у детей раннего возраста
Диагностика и коррекция нарушения зрения у детей раннего возраста