- Bases of endoscopic surgery

Содержание
- 2. Endoscopic surgery it is area of the surgery, allowing to execute radical operations or diagnostic procedures
- 3. Development of endoscopic surgery Hippocrat (460-375 up to AD) - has described carrying out of the
- 4. George Kelling (1901) – for the first time has made a laparoscopy in experiment on a
- 5. Light source of Arno
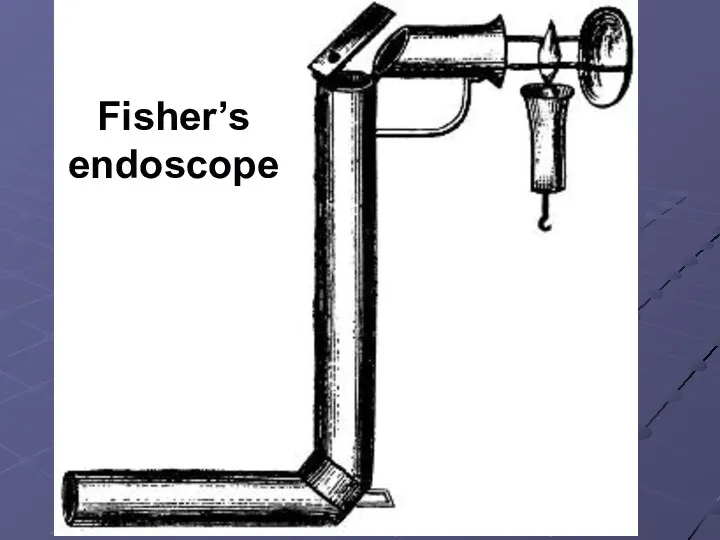
- 6. Fisher’s endoscope
- 7. Phillip Bozini
- 8. Bozini’s endoscope
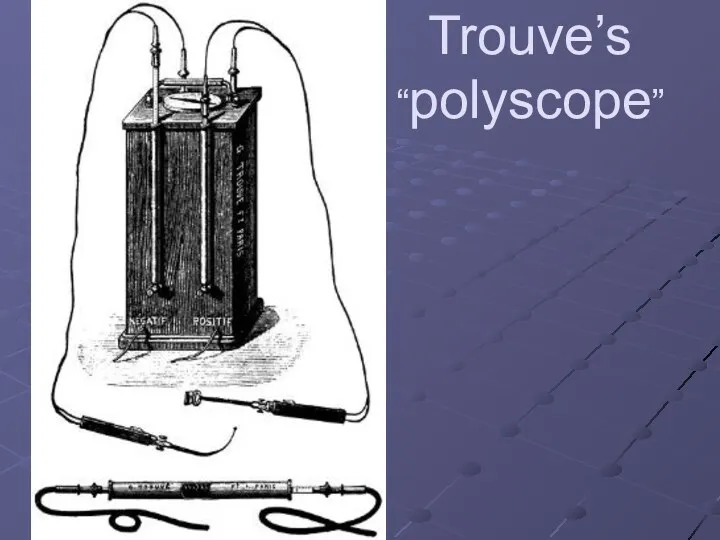
- 9. Trouve’s “polyscope”
- 10. George Kelling
- 11. Heinz Kalk
- 12. Raul Palmer
- 13. Kurt Semm
- 14. Мурре
- 15. Harold Hopkins
- 16. Advantages of endosurgery in comparison with traditional operations Slight trauma of tissues Short hospital period Decrease
- 17. Complications General lethality come to 0,5 %, and frequency of complications – 10 %; Wound infection
- 18. Relative contraindications Heavy accompanying pathology of cardiovascular and respiratory systems - Obstructive diseases of lungs -
- 19. The minimal set for carrying out endoscopic operations a) Needles for imposing pneumoperitoneum; b) trocars with
- 20. The general requirements to endoscopic tools а) Handiness: the handle of the tool should not complicate
- 21. Essentially the complex will consist of the following blocks: a) A videocamera; b) A video monitor;
- 22. Endosurgical complex
- 24. illuminator
- 25. Aquapurator
- 26. videocamera
- 27. Telescope
- 28. Usual telescope and telescope of Hopkins‘s system
- 29. Insufflator
- 30. Veress needles
- 31. Trendelenburg’s position
- 32. Fauler’s position
- 33. Points of a puncture for imposing a pneumoperitoneum
- 34. Puncture through the back fornix of vagina
- 35. Needle position
- 36. Trocars VERSAPORT
- 37. Trocar VISIPORT
- 38. Introduction of trocar by Hasson
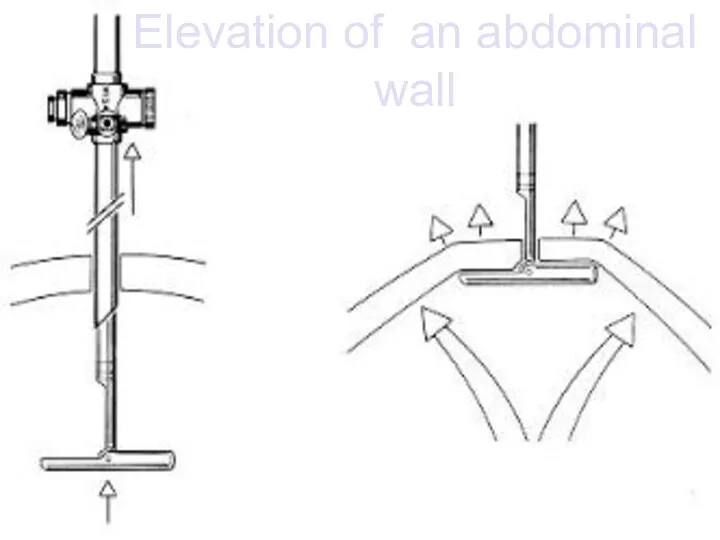
- 39. Elevation of an abdominal wall
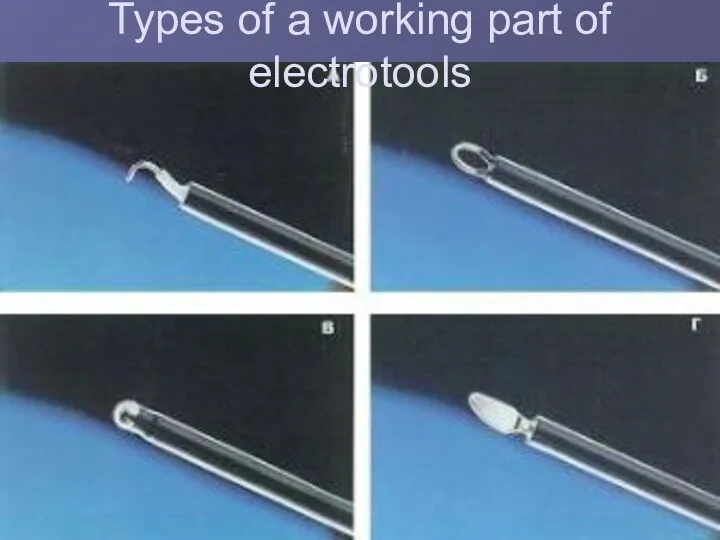
- 40. Types of a working part of electrotools
- 41. retractor
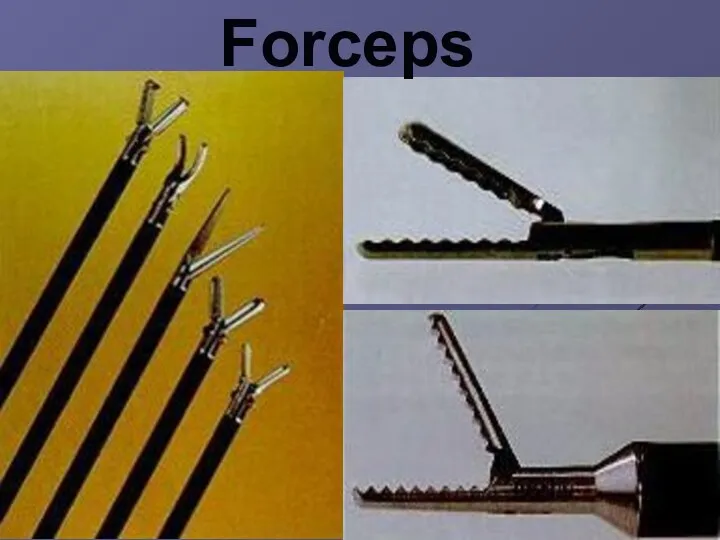
- 42. Forceps
- 43. иглодержатели
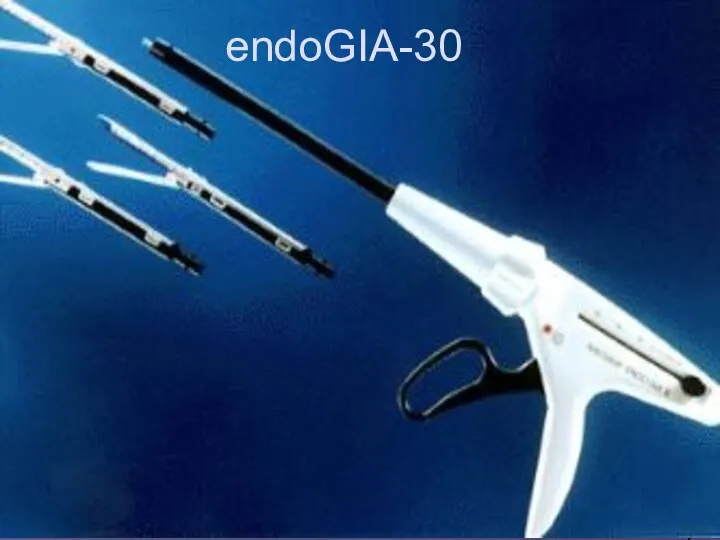
- 44. endoGIA-30
- 45. EndoStitch
- 46. Introduction of an atraumatic needles
- 47. The scheme of Reder’s knot
- 49. Скачать презентацию
Endoscopic surgery
it is area of the surgery, allowing to execute radical operations
Endoscopic surgery
it is area of the surgery, allowing to execute radical operations
Development of endoscopic surgery
Hippocrat (460-375 up to AD) - has described carrying
Development of endoscopic surgery
Hippocrat (460-375 up to AD) - has described carrying
George Kelling (1901) – for the first time has made a laparoscopy in
George Kelling (1901) – for the first time has made a laparoscopy in
Light source of Arno
Light source of Arno
Fisher’s
endoscope
Fisher’s
endoscope
Phillip Bozini
Phillip Bozini
Bozini’s endoscope
Bozini’s endoscope

Trouve’s “polyscope”
Trouve’s “polyscope”
George Kelling
George Kelling
Heinz Kalk
Heinz Kalk

Raul Palmer
Raul Palmer
Kurt Semm
Kurt Semm
Мурре
Мурре
Harold Hopkins
Harold Hopkins
Advantages of endosurgery in comparison with traditional operations
Slight trauma of tissues
Short
Advantages of endosurgery in comparison with traditional operations
Slight trauma of tissues
Short
Complications
General lethality come to 0,5 %, and frequency of complications – 10 %;
Wound
Complications
General lethality come to 0,5 %, and frequency of complications – 10 %;
Wound
Relative contraindications
Heavy accompanying pathology of cardiovascular and respiratory systems
- Obstructive diseases
Relative contraindications
Heavy accompanying pathology of cardiovascular and respiratory systems
- Obstructive diseases
The minimal set for carrying out endoscopic operations
a) Needles for imposing pneumoperitoneum;
The minimal set for carrying out endoscopic operations
a) Needles for imposing pneumoperitoneum;
The general requirements to endoscopic tools
а) Handiness: the handle of the tool
The general requirements to endoscopic tools
а) Handiness: the handle of the tool
Essentially the complex will consist of the following blocks:
a) A videocamera;
b)
Essentially the complex will consist of the following blocks:
a) A videocamera;
b)
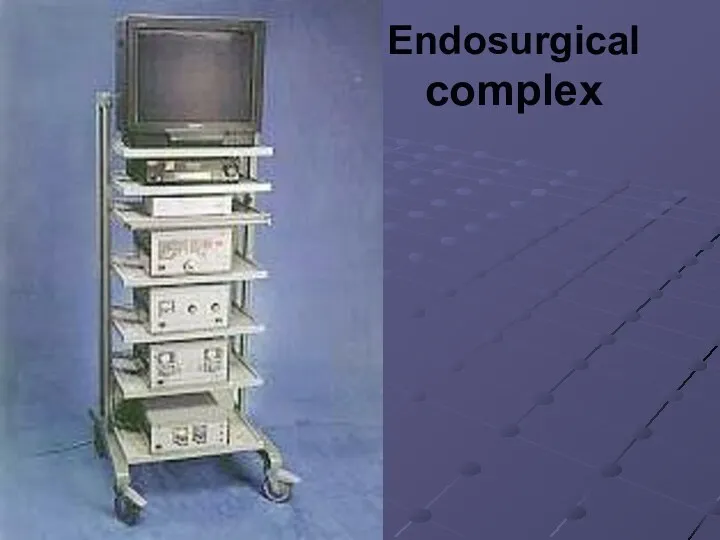
Endosurgical
complex
Endosurgical
complex
illuminator
illuminator

Aquapurator
Aquapurator

videocamera
videocamera

Telescope
Telescope
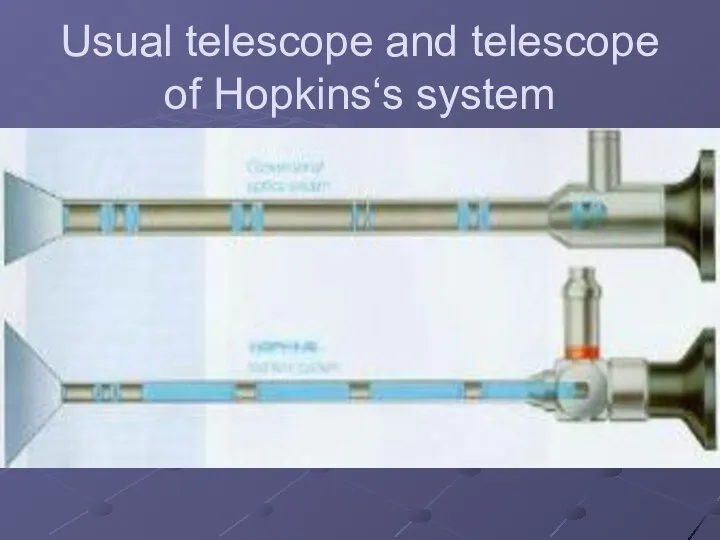
Usual telescope and telescope of Hopkins‘s system
Usual telescope and telescope of Hopkins‘s system
Insufflator
Insufflator

Veress needles
Veress needles

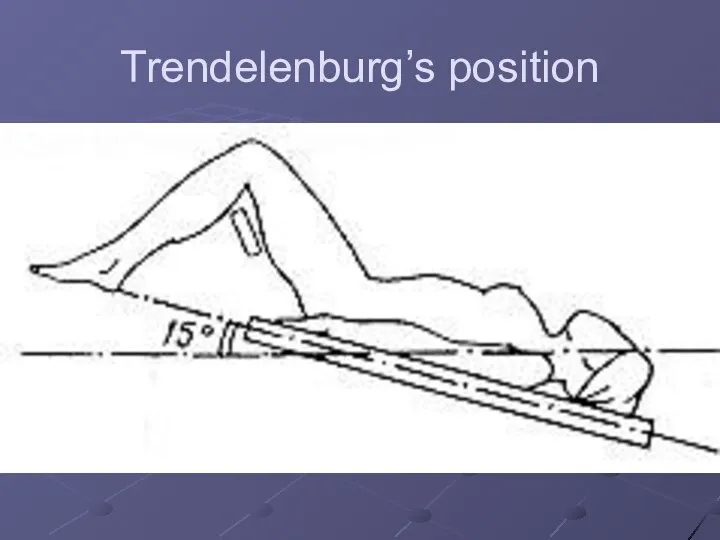
Trendelenburg’s position
Trendelenburg’s position
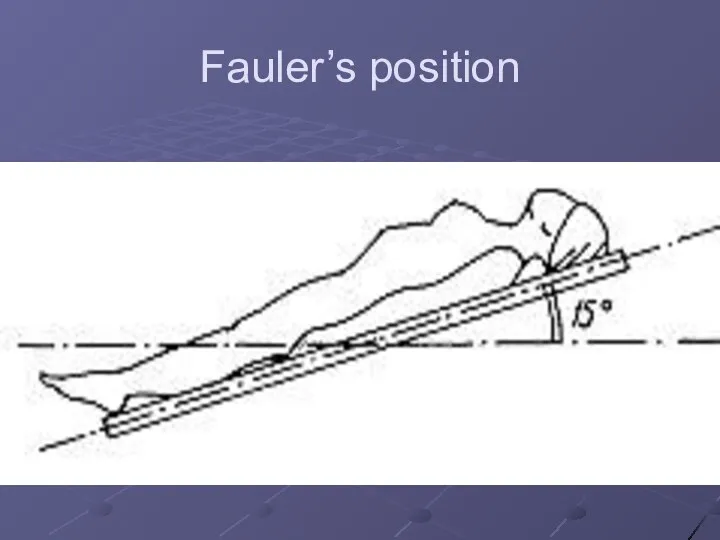
Fauler’s position
Fauler’s position
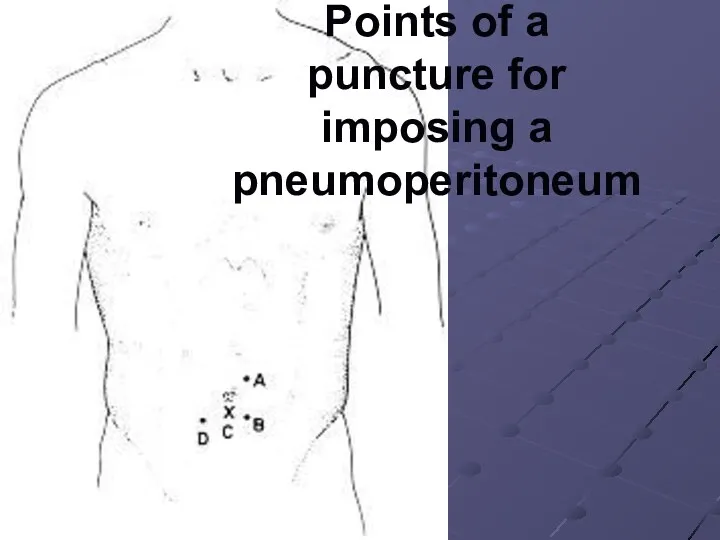
Points of a puncture for imposing a pneumoperitoneum
Points of a puncture for imposing a pneumoperitoneum
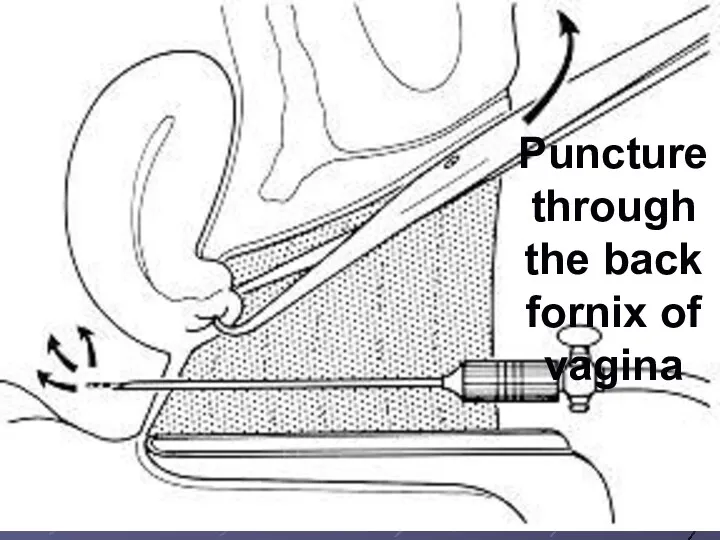
Puncture through the back fornix of vagina
Puncture through the back fornix of vagina
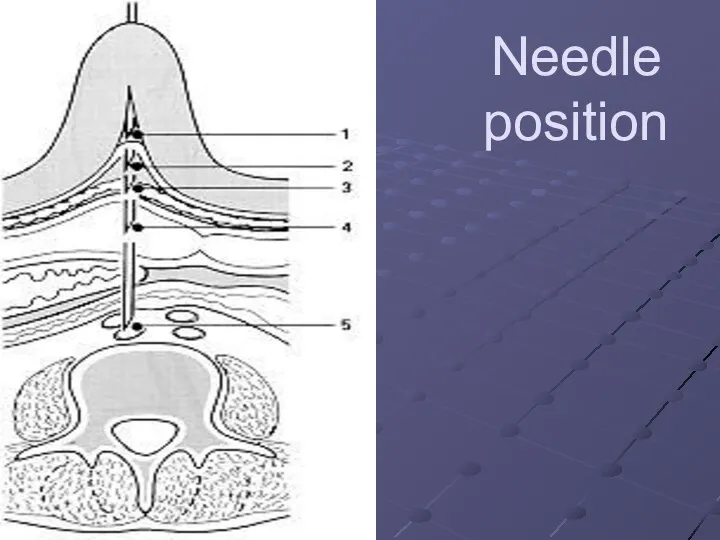
Needle position
Needle position
Trocars
VERSAPORT
Trocars
VERSAPORT

Trocar
VISIPORT
Trocar
VISIPORT

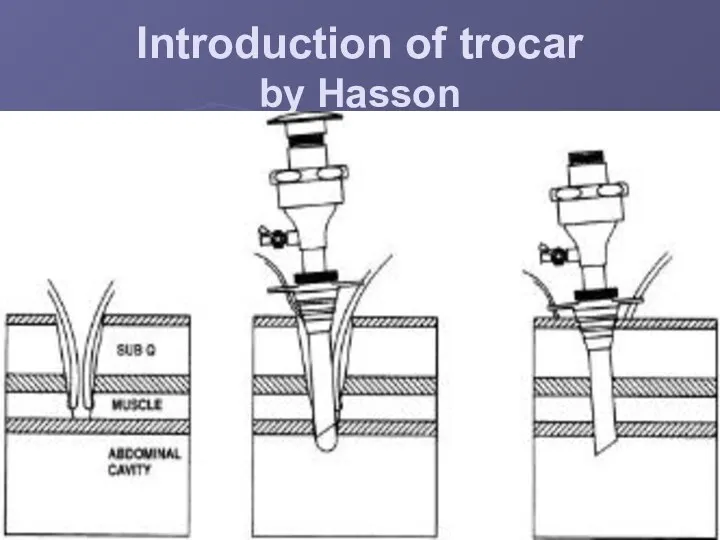
Introduction of trocar
by Hasson
Introduction of trocar
by Hasson
Elevation of an abdominal wall
Elevation of an abdominal wall
Types of a working part of electrotools
Types of a working part of electrotools
retractor
retractor

Forceps
Forceps
иглодержатели
иглодержатели

endoGIA-30
endoGIA-30
EndoStitch
EndoStitch

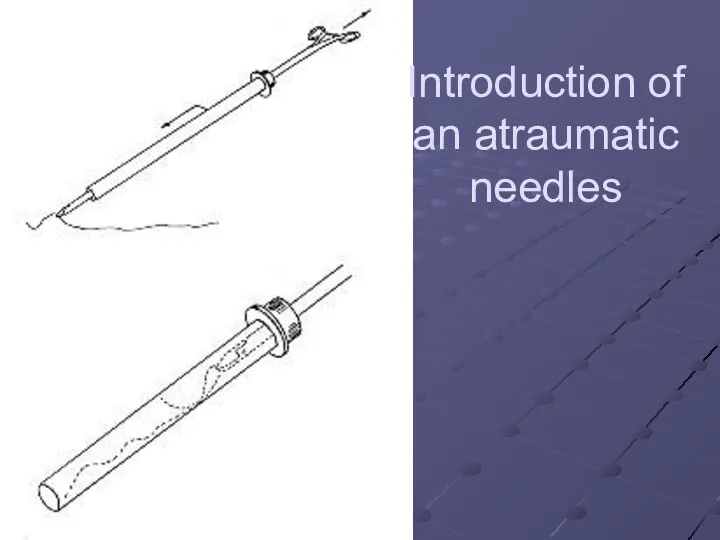
Introduction of an atraumatic needles
Introduction of an atraumatic needles
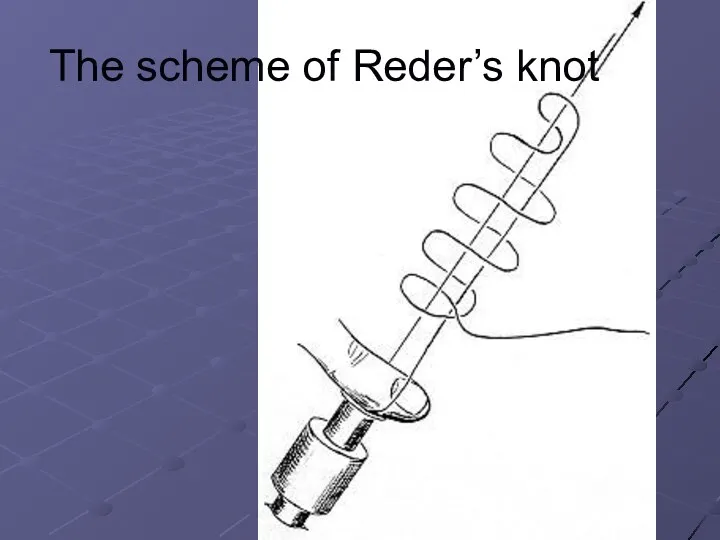
The scheme of Reder’s knot
The scheme of Reder’s knot
 Нанохимия и нанотехнологии. Методы и средства исследования нанообъектов. (Лекция 3)
Нанохимия и нанотехнологии. Методы и средства исследования нанообъектов. (Лекция 3) Первое и второе начало термодинамики
Первое и второе начало термодинамики Изучение треков заряженных частиц. Лабораторная работа № 7
Изучение треков заряженных частиц. Лабораторная работа № 7 Оценивание закономерностей окислительного изнашивания
Оценивание закономерностей окислительного изнашивания Строительная механика. Теория определения перемещений деформируемых систем. (Часть 1. Лекция 1)
Строительная механика. Теория определения перемещений деформируемых систем. (Часть 1. Лекция 1) Выбор реакторных устройств
Выбор реакторных устройств Спин, проекция на вектор n
Спин, проекция на вектор n Методы формирования уравнений электрического равновесия цепи
Методы формирования уравнений электрического равновесия цепи Электродвижущая сила. Закон Ома для полной цепи
Электродвижущая сила. Закон Ома для полной цепи Деятельностный подход в преподавании физики, как средство повышения качества знаний учащихся
Деятельностный подход в преподавании физики, как средство повышения качества знаний учащихся Тепловые двигатели и их влияние на окружающую среду
Тепловые двигатели и их влияние на окружающую среду Электрический ток. (лекция 2)
Электрический ток. (лекция 2) Physical chemistry of nanostructured systems
Physical chemistry of nanostructured systems Конструирование элементов ременных и цепных передач
Конструирование элементов ременных и цепных передач Роль фізичної та астрономічної наук у формуванні наукового світогляду сучасної людини
Роль фізичної та астрономічної наук у формуванні наукового світогляду сучасної людини Удельная теплота. Тест
Удельная теплота. Тест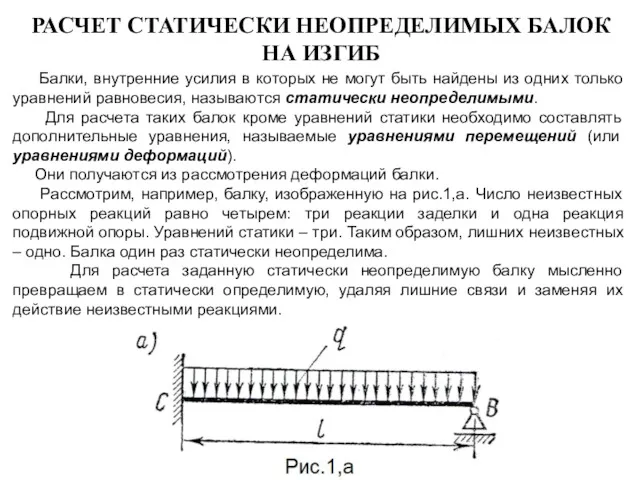 Расчет статически неопределимых балок на изгиб
Расчет статически неопределимых балок на изгиб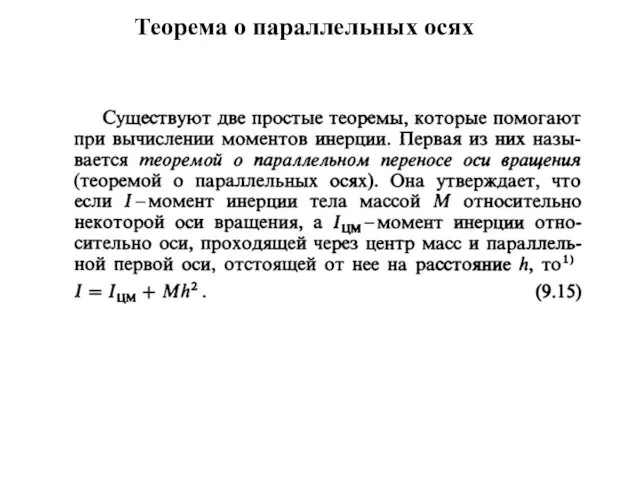 Момент инерции
Момент инерции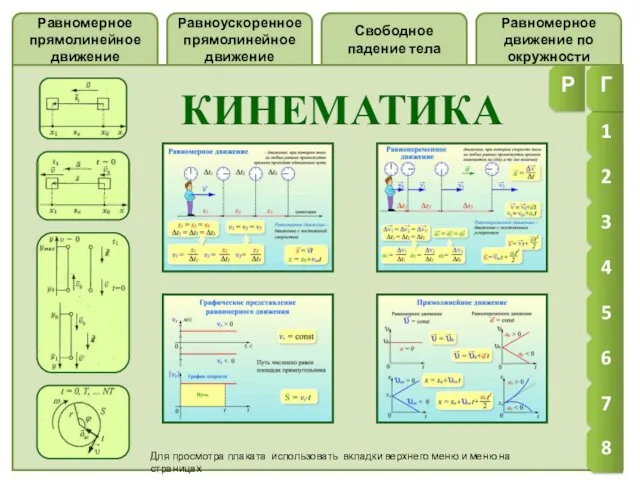 Кинематика
Кинематика Предохранительный клапан
Предохранительный клапан Введение в динамику. Законы и аксиомы динамики материальной точки. Основное уравнение динамики
Введение в динамику. Законы и аксиомы динамики материальной точки. Основное уравнение динамики Презентация к уроку по теме Механическая работа 7 класс
Презентация к уроку по теме Механическая работа 7 класс Сила тока. Амперметр
Сила тока. Амперметр Теплообмен излучением между телами, разделённой прозрачной средой. Коэффициент облучённости. Теплообмен между телами
Теплообмен излучением между телами, разделённой прозрачной средой. Коэффициент облучённости. Теплообмен между телами Основы кинематики. Раздел механики, в котором описывается движение тел, но не анализируются его причины
Основы кинематики. Раздел механики, в котором описывается движение тел, но не анализируются его причины Выходные устройства авиационных двигателей. (Тема 7)
Выходные устройства авиационных двигателей. (Тема 7) Summary of effective use 6
Summary of effective use 6 Сообщающиеся сосуды и их применение
Сообщающиеся сосуды и их применение