- Diabetes Anterior hypophysis Diabetes insipidus

Содержание
- 2. Diabetes Definition ,classification, type 1 and 2, acute and chronic complications , treatment
- 3. Diabetes definition Diabetes is a heterogeneous, complex metabolic disorder characterized by elevated blood glucose concentration secondary
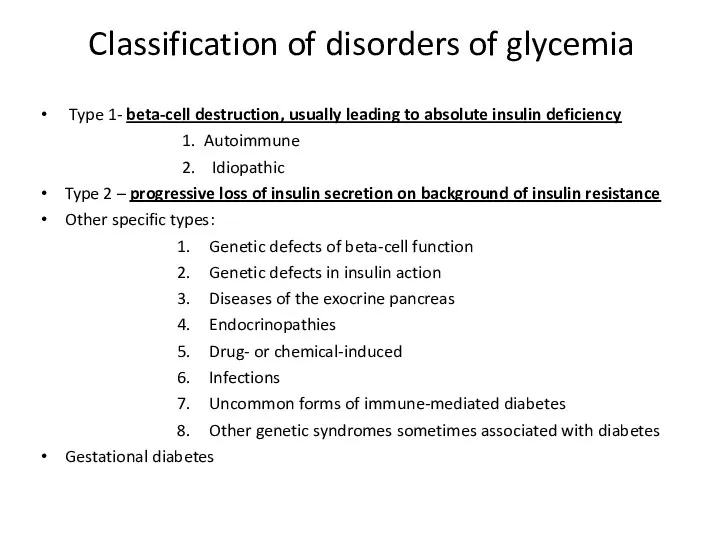
- 4. Classification of disorders of glycemia Type 1- beta-cell destruction, usually leading to absolute insulin deficiency 1.
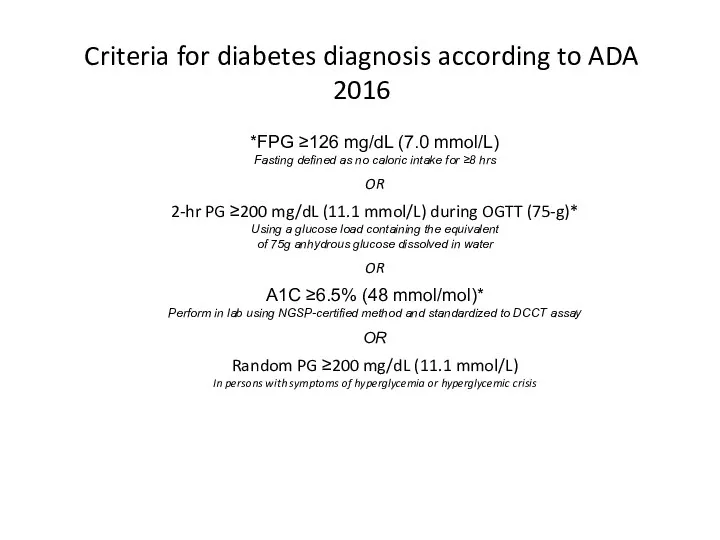
- 5. Criteria for diabetes diagnosis according to ADA 2016 *In absence of unequivocal hyperglycemia, result to be
- 6. Factors affecting HbA1C
- 7. Diabetes type 1 Usually caused by autoimmune heterogenic destruction of beta-cells. The prevailing immune process that
- 8. Diabetes type 1 Roughly 5-15% of all cases of diabetes. Two peaks:5-7 year and adolescence. Yearly
- 9. Risk of Type1 95% of persons who develop Type1 DR-3-DQ2 DR4-DR8
- 10. Autoantibodies (90% at the diagnosis of type 1) Anti GAD(Glutamic Acid Decarboxilase) 65 . Anti ICA
- 12. Diabetes type2 90 % of all diabetes in the world 9.3% of USA population in 2014(29.1
- 13. Pathogenesis of type 2
- 14. Genetic defects of insulin secretion 2-5% of all cases of diabetes mellitus Heterogeneous group of diabetes
- 15. High index of suspicion of MODY A family history of diabetes in one parent and first-degree
- 16. Beta- cell: insulin secretion
- 17. Monogenic defects in insulin secretion
- 18. MODY 3(HNF1α mutation) Most prevalent MODY:50-70 % of all mutations. Onset before age of 30. Accented
- 19. MODY 2 Mild hyperglycemia started at birth. The glucokinase enzyme catalyzes the rate limiting step of
- 20. Diagnostic approach to monogenic diabetes
- 21. Genetic defects in insulin action Rabson Mendenhall :short stature,protuberant abdomen ,teethand nail abnormalities Leprehuanism: IUGR,fasting hypoglycemia
- 22. Disorder of exocrine pancreas Chronic pancreatitis: more than 20 years of disease -80-90% risk of DM.
- 23. Endocrinopathies Cushing disease and syndrome-glucose intolerance and overt diabetes (30 %). Acromegaly –direct anti- insulin effect
- 24. examples))Drug and chemicals Ethanol – chronic pancreatitis-overt diabetes(1% of all diabetes in USA) Glucocorticoids: inhibition of
- 25. Infections Predisposition to type 1- enteroviruses. Direct beta- cells destruction-mumps ,coxsackieviruses B, adenoviruses . Congenital rubella
- 26. Uncommon immune form of diabetes High titers of antibodies to insulin receptors - severe hyperglycemia,acanthosis nigricans
- 27. Pregnancy in women with normal glucose metabolism Fasting levels of blood glucose that are lower than
- 28. Gestational diabetes mellitus(GDM) Disbalance between insulin secretion and increased insulin resistance especially in the third trimester.
- 29. Screening for GDM
- 30. Algorithm of glucose testing in pregnancy All women have to be screened for diabetes as essential
- 31. Goals of diabetes treatment Prevent macrovasular diabetes complication-cardiovascular disease (IHD, diabetic cardiomyopathy, TIA, fatal and non-
- 32. Aspects of diabetes treatment Glycemic control Lifestyle intervention include obesity treatment Medical nutritional therapy Control of
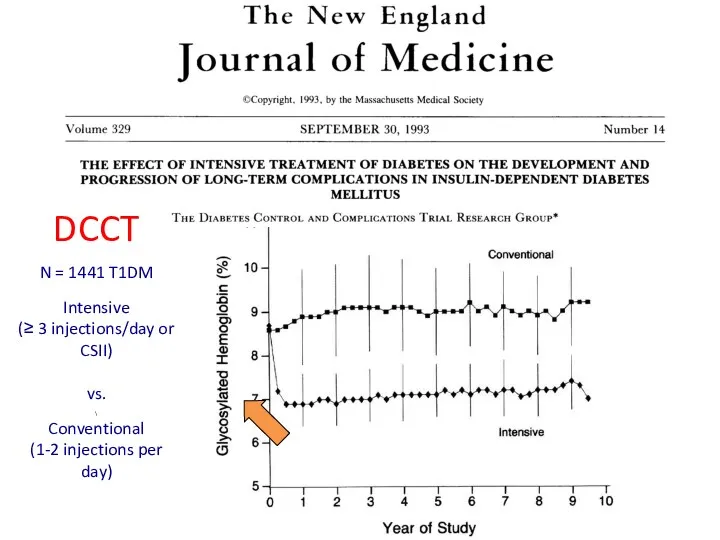
- 33. Glycemic control and diabetic complication Type 1 study: DCCT –EDIC(Diabetes Control and Complication Trial- Epidemiology of
- 34. DCCT N = 1441 T1DM Intensive (≥ 3 injections/day or CSII) vs. \ Conventional (1-2 injections
- 35. Inclusion criteria for DCCT Primary prevention group : DM type 1: 1-5 years, no retinopathy or
- 36. Baseline characteristics
- 37. Goals and modes of therapy conventional group Conventional group therapy goals: to prevent symptoms attributable to
- 38. Goals and modes of treatment intensive treatment group 3 or more insulin injection or pump therapy.
- 39. Study questions Prevention of diabetic retinopathy in primary prevention group by intensive treatment versus conventional group
- 40. Reduction in Retinopathy The Diabetes Control and Complications Trial Research Group. N Engl J Med 1993;329:977-986.
- 41. Solid line = risk of developing microalbuminuria Dashed line = risk of developing macroalbuminuria DCCT: Reduction
- 42. Reduction in Neuropathy The Diabetes Control and Complications Trial Research Group. N Engl J Med 1993;329:977-986.
- 43. DCCT/EDIC Study Research Group. N Engl J Med 2005;353:2643–2653. Reduction of cardiovascular event in DCCT –EDIC
- 44. Hypoglycemia and other adverse events General and severe hypoglycemia 3 times higher in intensively treatment group
- 45. GLYCEMIC CONTROL IN TYPE 2 UKPDS 20-year interventional trial from 1977 to 1997. 5,102 patients with
- 46. UKPDS: Aims To determine whether improved glucose control of Type 2 diabetes will prevent clinical complications
- 47. UKPDS patient characteristics 5102 newly diagnosed Type 2 diabetic patients age 25 - 65 y mean
- 48. Treatment Policies in 3867 patients Conventional Policy n = 1138 initially with diet alone aim for
- 49. UKPDS Study Group. Lancet 1998; 352:837–853. UKPDS: intensive control reduces complications in type 2 diabetes
- 50. UKPDS Any diabetes related endpoints
- 51. UKPDS- metformin Main Randomisation 4209 Overweight 1704 Non overweight 2505 Conventional Policy 411 Intensive Policy 1293
- 52. Metformin in overweight patients in comparison with conventional treatment 32% risk reduction in any diabetes-related endpoints,
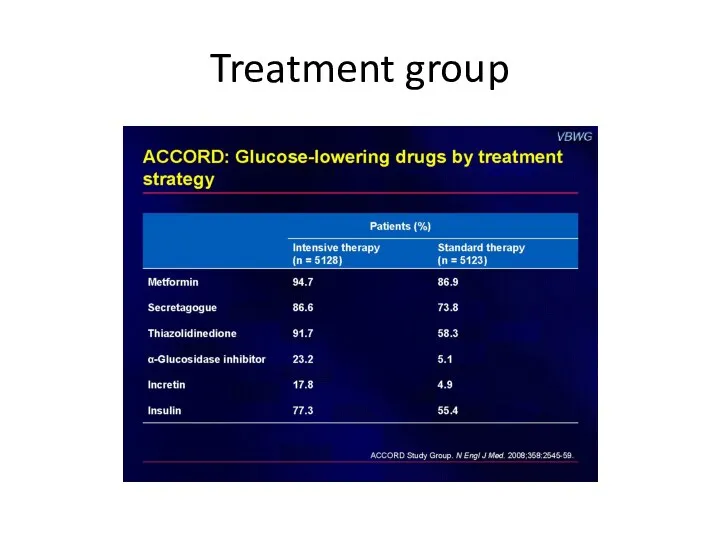
- 53. ACCORD trial 10251 patients with diabetes with HbA1c 7.6-8.9 randomly assigned to intensive therapy in order
- 54. Treatment group
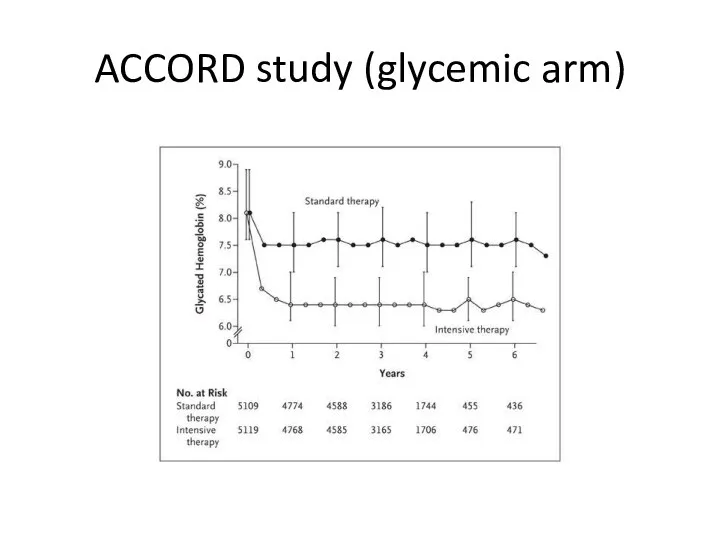
- 55. (ACCORD study (glycemic arm
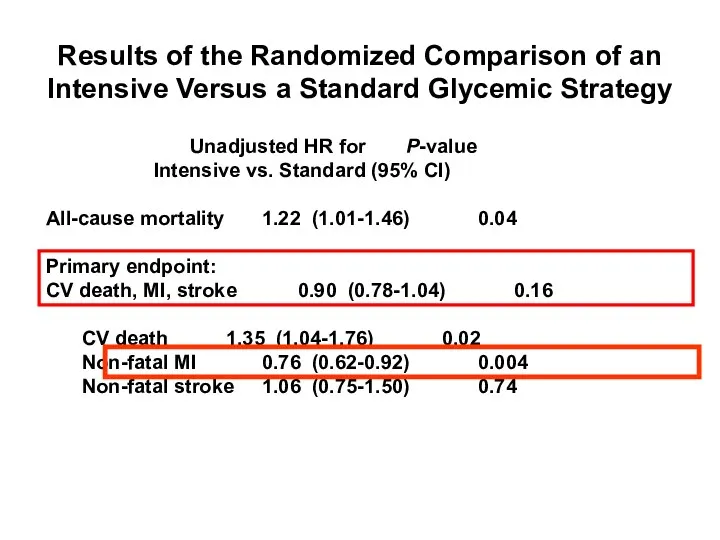
- 56. Gerstein HC et al. The ACCORD Study Group. N Engl J Med. 2008;358:2545–2559. Results of the
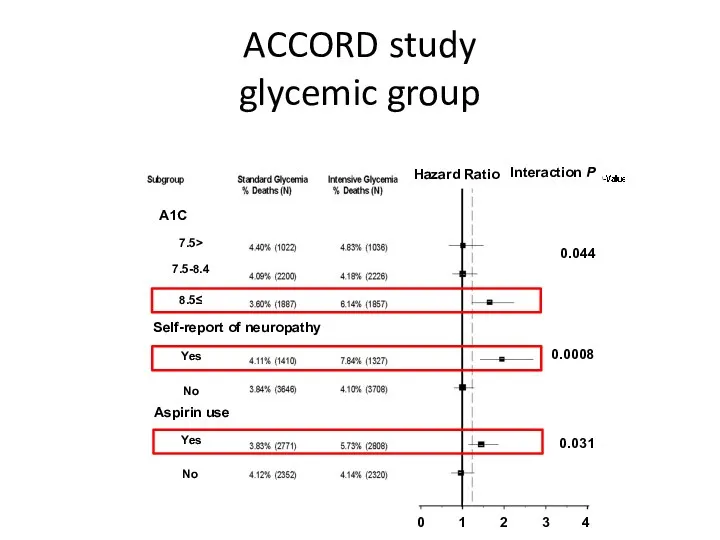
- 57. ACCORD study glycemic group
- 58. ADVANCE collaborative group
- 59. Results of intensive glucose lowering in ADVANCE trial Average lowering of HbA1c from 7.2 to 6.5%
- 60. VA Diabetes Trial (VADT) Similar study design: intensive therapy versus standard therapy. Primary endpoint: first CVD
- 61. Differences in ACCORD/ADVANCE/VADT Skyler JS, Bergenstal R, Bonow RO, et al. Diabetes Care. 2009;32:187-192.
- 62. Change in HbA1c during the trial
- 63. Initial results No excess of cardiovascular mortality. No improvement of cardiovascular morbidity. No change in incidence
- 64. 10 years follow up of VADT cohort: glycemic control
- 65. Cardiovascular outcomes after 10 years
- 66. Glycemic targets in diabetes: general consideration (ADA 2016)
- 67. Individualized treatment ADA 2016
- 68. Glycemic targets for treatment of pregnant women with type 1 and 2
- 69. Glycemic targets for treatment of pregnant women with type 1 and 2 diabetes Glycemic targets for
- 70. Type 1 insulin treatment Concept of basal - bolus Prescription of short and long acting insulins
- 71. Serum Insulin Level Time guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca Copyright © 2013 Canadian Diabetes Association
- 72. Insulin analogues
- 73. Treatment scheme
- 74. :Principles of type 2 treatment (1)non –pharmacologic therapy Physical activity. 1.1Minimum 150 minutes weekly moderate intensity
- 75. :Principles of type 2 treatment (2)non –pharmacologic therapy Diet and carbohydrates 500-750 kcal/d deficit:1200-1500 kcal /d
- 76. :Principles of type 2 treatment (3)non –pharmacologic therapy Diet and proteins 0.8 g/kg daily allowance. Enhance
- 77. Pharmacological treatment of glycemia type 2:drug classification Biguanides Secretagogues DPP4 inhibitors α- glycosidase inhibitor Thiazolidinedione GLP1
- 78. Biguanides Metfomin(Glucomin,Glucophage) Preferred initial pharmacologic agent because of long standing record of efficacy and safety and
- 79. Metformin Half-life up to 3 hour. No metabolism ,excreted by kidney as active compound. May be
- 80. Metformin toxicity and side effects Gastrointestinal (20-30%): start with lower dose with or after meals, make
- 81. Secretagogues Sulfonylureas: bind to SUR1 site of inward rectified KATP channel on beta-cells : 2 generation
- 82. 2-nd generation sulfonylureas Adverse effect : hypoglycemia ,weight gain Secondary failure : sulfonylureas require functional beta
- 83. Glinides Binding to distinct (from sulfonylurea) SUR 1 site Burst phase-1 insulin secretion In vitro- glucose
- 84. DPP-IV: ACTION Cleaves GLP-1 Results in decreased signal to the pancreas—limiting insulin response. That in turn
- 85. The Role of GLP-1 DPP-4 Inhibitors Increase ½ Life of GLP-1
- 86. DPP4 inhibitors Januvia Trajenta Onglysa Galvus Name Class Half-life Dose (mg) Use Very few side effects:
- 87. GLP1 agonists(injectable agents) Breakthrough in DM 2 treatment Glycemic ,cardiovascular (LEADER study)benefit , significant weight loss
- 88. α- glucosidase inhibitors Acarbose (Prandase ) max 100 mg *3/d May have cardiovascular benefits (STOP –
- 89. Thiazolidinediones Gamma- PPAR agonists. Increase of insulin sensitivity in adipose tissue skeletal muscle and liver. Warning
- 90. SGLT2 inhibitors
- 91. SGLT2 inhibitors medications Empafliglozin (Jardiance)10 mg ,25 mg Dapafliglozin(Forxiga) 10 mg Positive effects :glucose lowering without
- 92. Algorithm ADA of glycemic treatment 2016
- 93. Comprehensive care of diabetes(ADA 2016) Stop smoking. Treat blood pressure to targets :less than140/90 mmHg: ADVANCE
- 94. Statin treatment and diabetes Patients 40-75 without additional atherosclerotic cardiovascular disease(ACVD) risk factor- moderate intensity statin+
- 96. Скачать презентацию
Diabetes
Definition ,classification, type 1 and 2, acute and chronic complications ,
Diabetes
Definition ,classification, type 1 and 2, acute and chronic complications ,
Diabetes definition
Diabetes is a heterogeneous, complex metabolic disorder characterized by elevated
Diabetes definition
Diabetes is a heterogeneous, complex metabolic disorder characterized by elevated
Classification of disorders of glycemia
Type 1- beta-cell destruction, usually leading
Classification of disorders of glycemia
Type 1- beta-cell destruction, usually leading
Criteria for diabetes diagnosis according to ADA 2016
*In absence of unequivocal
Criteria for diabetes diagnosis according to ADA 2016
*In absence of unequivocal
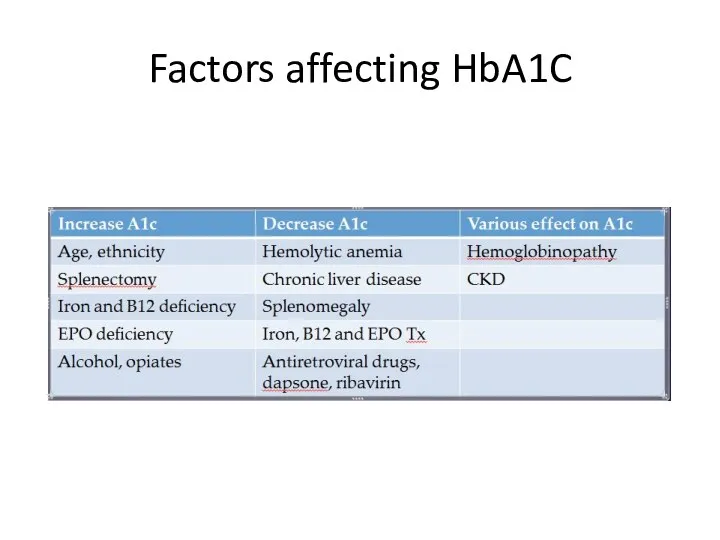
Factors affecting HbA1C
Factors affecting HbA1C
Diabetes type 1
Usually caused by autoimmune heterogenic destruction of beta-cells.
The prevailing
Diabetes type 1
Usually caused by autoimmune heterogenic destruction of beta-cells.
The prevailing
Diabetes type 1
Roughly 5-15% of all cases of diabetes.
Two peaks:5-7 year
Diabetes type 1
Roughly 5-15% of all cases of diabetes.
Two peaks:5-7 year
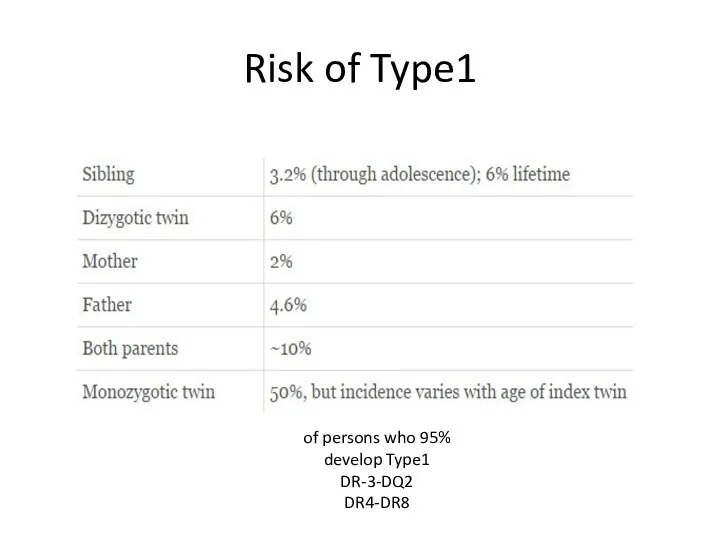
Risk of Type1
95% of persons who develop Type1
DR-3-DQ2
DR4-DR8
Risk of Type1
95% of persons who develop Type1
DR-3-DQ2
DR4-DR8
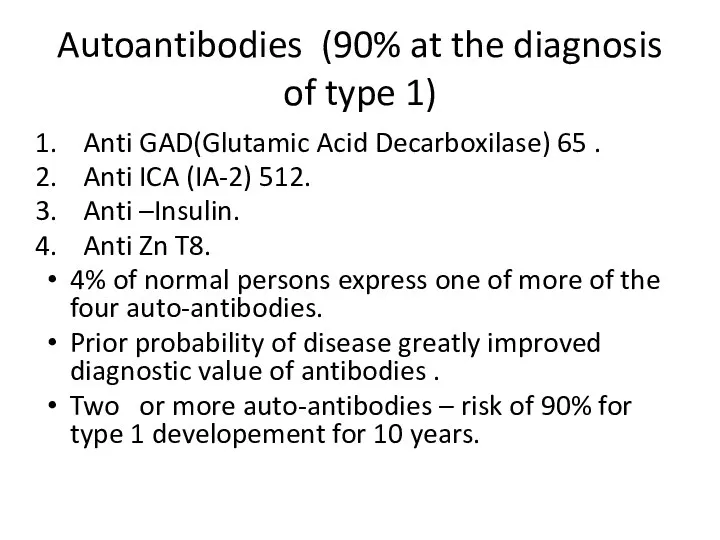
Autoantibodies (90% at the diagnosis of type 1)
Anti GAD(Glutamic Acid Decarboxilase)
Autoantibodies (90% at the diagnosis of type 1)
Anti GAD(Glutamic Acid Decarboxilase)
Diabetes type2
90 % of all diabetes in the world
9.3% of USA
Diabetes type2
90 % of all diabetes in the world
9.3% of USA
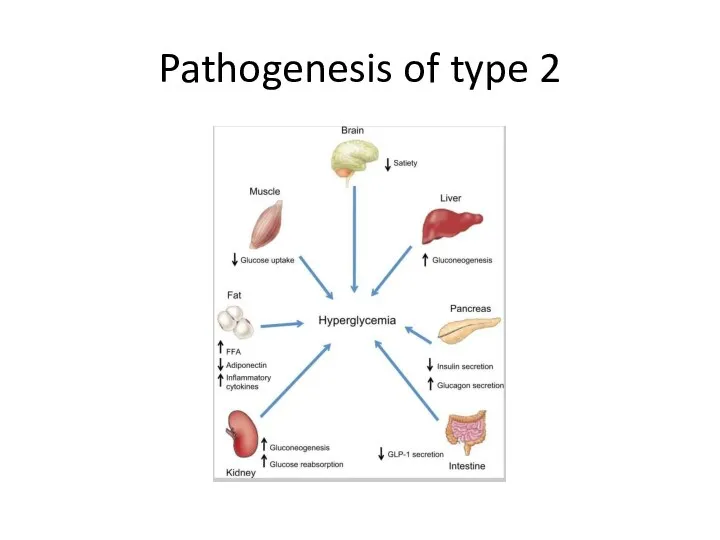
Pathogenesis of type 2
Pathogenesis of type 2
Genetic defects of insulin secretion
2-5% of all cases of diabetes
Genetic defects of insulin secretion
2-5% of all cases of diabetes
High index of suspicion of MODY
A family history of diabetes in
High index of suspicion of MODY
A family history of diabetes in
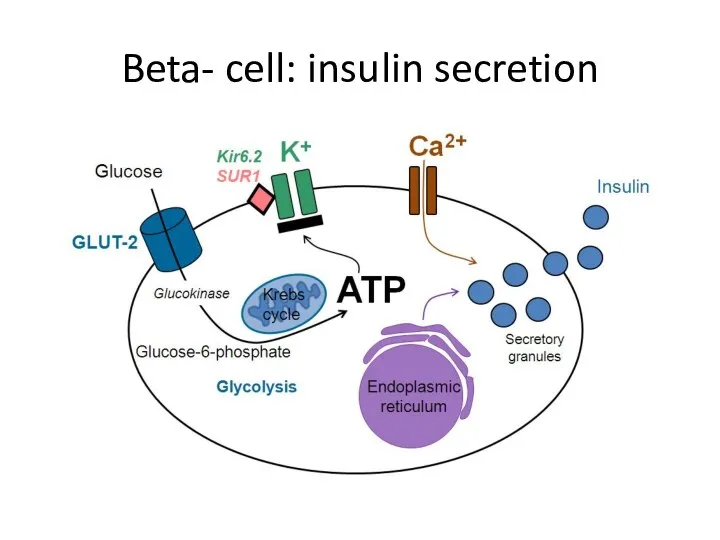
Beta- cell: insulin secretion
Beta- cell: insulin secretion
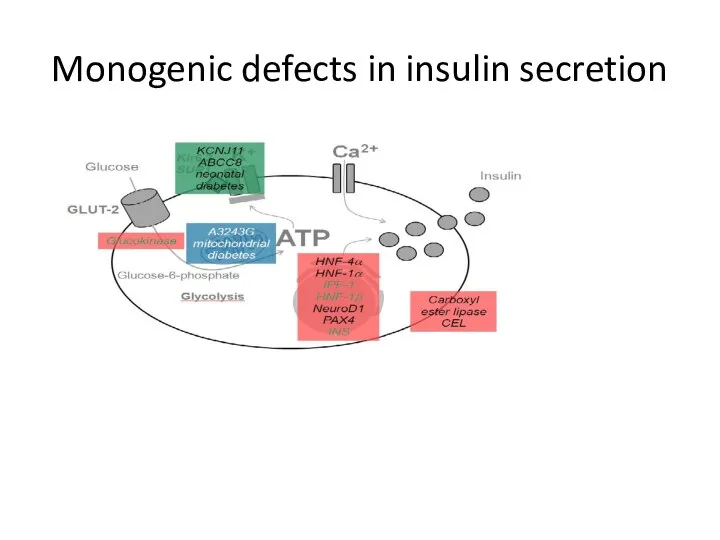
Monogenic defects in insulin secretion
Monogenic defects in insulin secretion
MODY 3(HNF1α mutation)
Most prevalent MODY:50-70 % of all mutations.
Onset before age
MODY 3(HNF1α mutation)
Most prevalent MODY:50-70 % of all mutations.
Onset before age
MODY 2
Mild hyperglycemia started at birth.
The glucokinase enzyme catalyzes the rate
MODY 2
Mild hyperglycemia started at birth.
The glucokinase enzyme catalyzes the rate
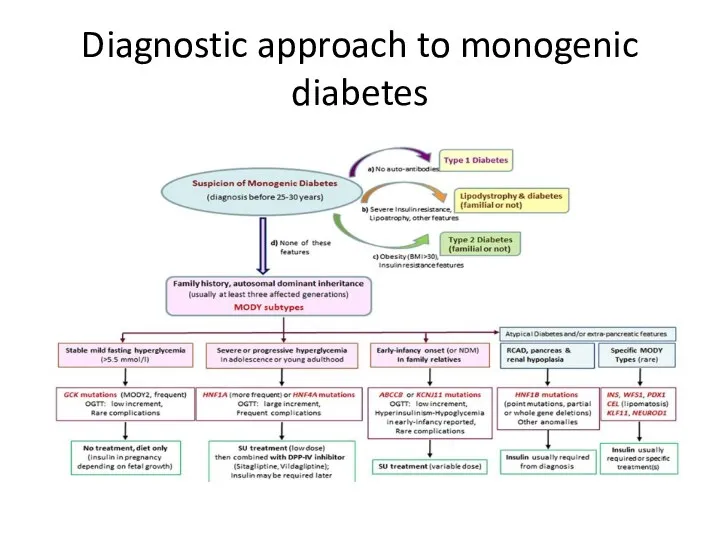
Diagnostic approach to monogenic diabetes
Diagnostic approach to monogenic diabetes
Genetic defects in insulin action
Rabson Mendenhall :short stature,protuberant abdomen ,teethand nail
Genetic defects in insulin action
Rabson Mendenhall :short stature,protuberant abdomen ,teethand nail
Disorder of exocrine pancreas
Chronic pancreatitis: more than 20 years of disease
Disorder of exocrine pancreas
Chronic pancreatitis: more than 20 years of disease
Endocrinopathies
Cushing disease and syndrome-glucose intolerance and overt diabetes (30 %).
Acromegaly –direct
Endocrinopathies
Cushing disease and syndrome-glucose intolerance and overt diabetes (30 %).
Acromegaly –direct
examples))Drug and chemicals
Ethanol – chronic pancreatitis-overt diabetes(1% of all diabetes in
examples))Drug and chemicals
Ethanol – chronic pancreatitis-overt diabetes(1% of all diabetes in
Infections
Predisposition to type 1- enteroviruses.
Direct beta- cells destruction-mumps ,coxsackieviruses B, adenoviruses
Infections
Predisposition to type 1- enteroviruses.
Direct beta- cells destruction-mumps ,coxsackieviruses B, adenoviruses
Uncommon immune form of diabetes
High titers of antibodies to insulin
Uncommon immune form of diabetes
High titers of antibodies to insulin
Pregnancy in women with normal glucose
metabolism
Fasting levels of blood glucose
Pregnancy in women with normal glucose
metabolism
Fasting levels of blood glucose
Gestational diabetes mellitus(GDM)
Disbalance between insulin secretion and increased insulin resistance especially
Gestational diabetes mellitus(GDM)
Disbalance between insulin secretion and increased insulin resistance especially
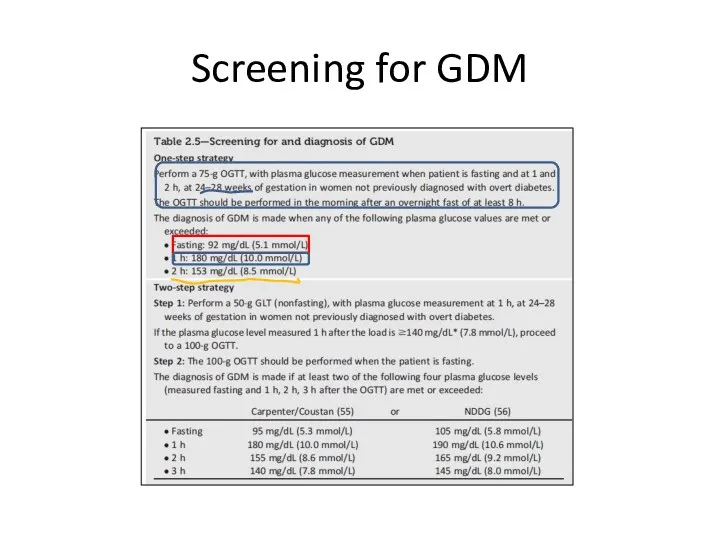
Screening for GDM
Screening for GDM
Algorithm of glucose testing in pregnancy
All women have to be screened
Algorithm of glucose testing in pregnancy
All women have to be screened
Goals of diabetes treatment
Prevent macrovasular diabetes complication-cardiovascular disease (IHD, diabetic cardiomyopathy,
Goals of diabetes treatment
Prevent macrovasular diabetes complication-cardiovascular disease (IHD, diabetic cardiomyopathy,
Aspects of diabetes treatment
Glycemic control
Lifestyle intervention include obesity treatment
Medical
Aspects of diabetes treatment
Glycemic control
Lifestyle intervention include obesity treatment
Medical
Glycemic control and diabetic complication
Type 1 study:
DCCT –EDIC(Diabetes Control and
Glycemic control and diabetic complication
Type 1 study:
DCCT –EDIC(Diabetes Control and
DCCT
N = 1441 T1DM
Intensive
(≥ 3 injections/day or CSII)
vs.
\
Conventional
(1-2
DCCT N = 1441 T1DM Intensive (≥ 3 injections/day or CSII) vs. \ Conventional (1-2
Inclusion criteria for DCCT
Primary prevention group : DM type 1:
Inclusion criteria for DCCT
Primary prevention group : DM type 1:
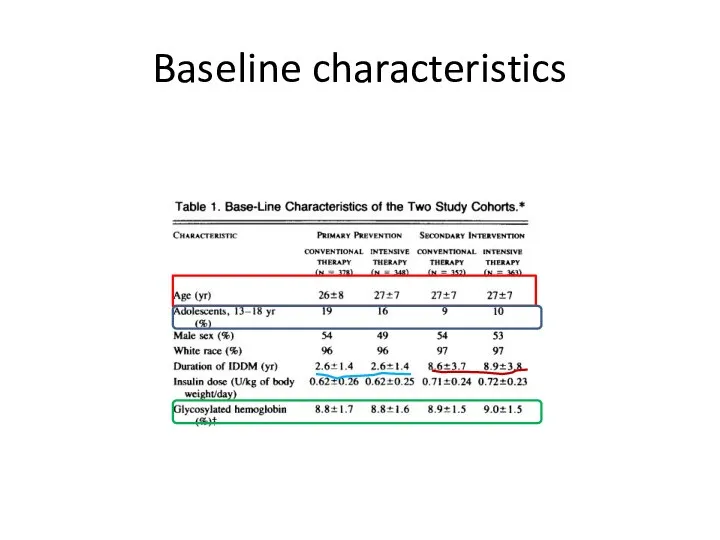
Baseline characteristics
Baseline characteristics
Goals and modes of therapy
conventional group
Conventional group therapy goals: to prevent
Goals and modes of therapy
conventional group
Conventional group therapy goals: to prevent
Goals and modes of treatment
intensive treatment group
3 or more
Goals and modes of treatment
intensive treatment group
3 or more
Study questions
Prevention of diabetic retinopathy in primary prevention group by
Study questions
Prevention of diabetic retinopathy in primary prevention group by
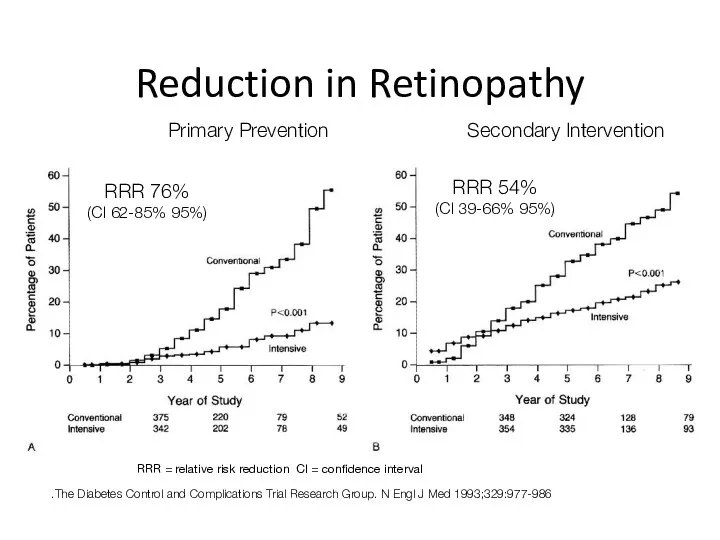
Reduction in Retinopathy
The Diabetes Control and Complications Trial Research Group. N
Reduction in Retinopathy
The Diabetes Control and Complications Trial Research Group. N
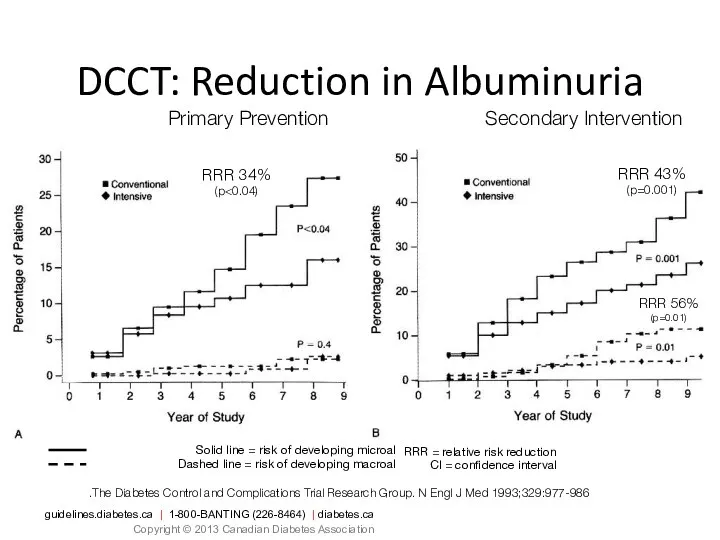
Solid line = risk of developing microalbuminuria
Dashed line = risk of
Solid line = risk of developing microalbuminuria
Dashed line = risk of
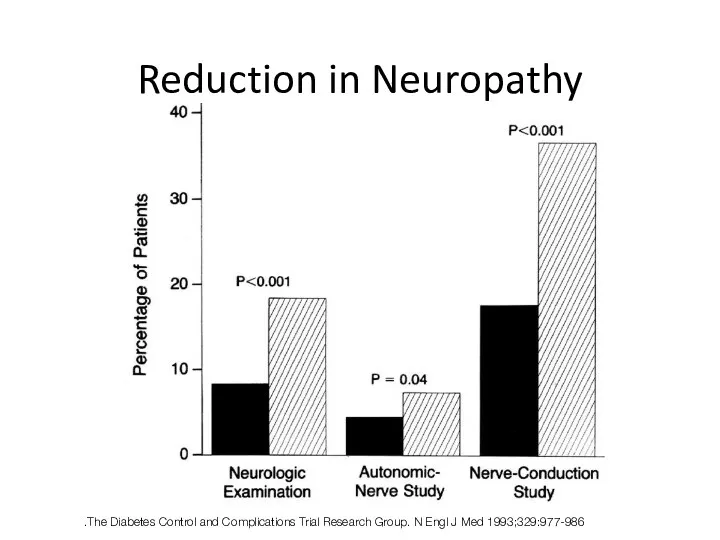
Reduction in Neuropathy
The Diabetes Control and Complications Trial Research Group. N
Reduction in Neuropathy
The Diabetes Control and Complications Trial Research Group. N
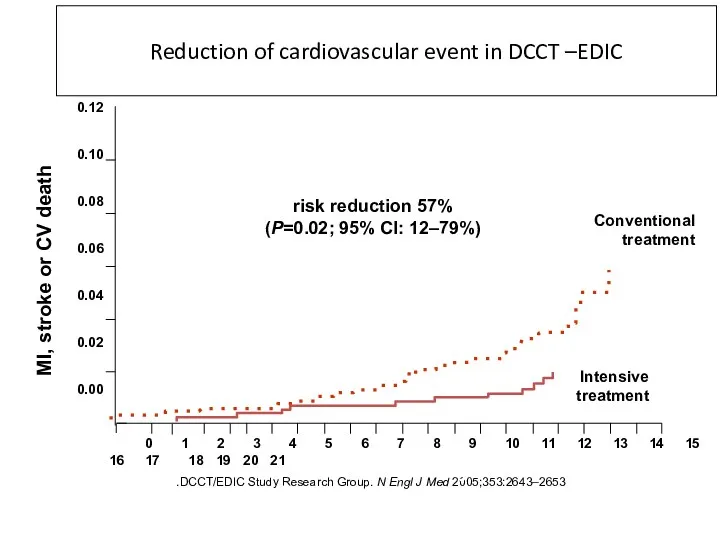
DCCT/EDIC Study Research Group. N Engl J Med 2005;353:2643–2653.
Reduction of cardiovascular
DCCT/EDIC Study Research Group. N Engl J Med 2005;353:2643–2653.
Reduction of cardiovascular
Hypoglycemia and other adverse events
General and severe hypoglycemia 3
Hypoglycemia and other adverse events
General and severe hypoglycemia 3
GLYCEMIC CONTROL IN TYPE 2
UKPDS
20-year interventional trial from 1977
GLYCEMIC CONTROL IN TYPE 2
UKPDS
20-year interventional trial from 1977
UKPDS: Aims
To determine whether improved glucose control of Type 2 diabetes
UKPDS: Aims
To determine whether improved glucose control of Type 2 diabetes
UKPDS patient characteristics
5102 newly diagnosed Type 2 diabetic patients
age 25 -
UKPDS patient characteristics
5102 newly diagnosed Type 2 diabetic patients
age 25 -
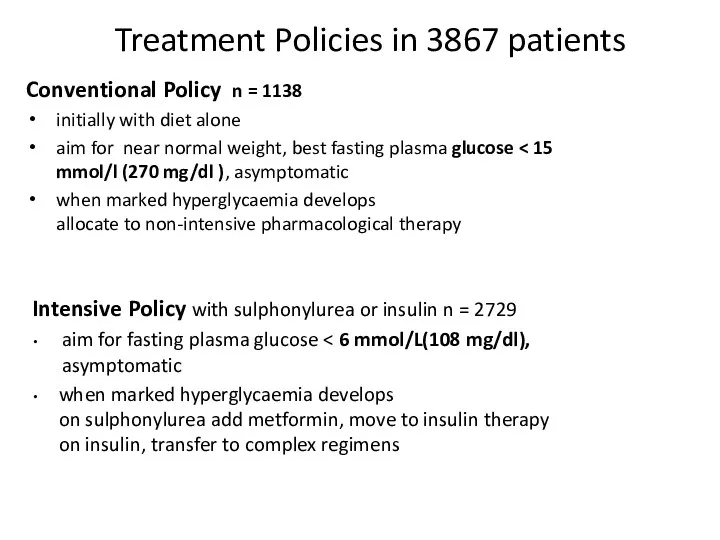
Treatment Policies in 3867 patients
Conventional Policy n = 1138
initially with diet
Treatment Policies in 3867 patients
Conventional Policy n = 1138
initially with diet
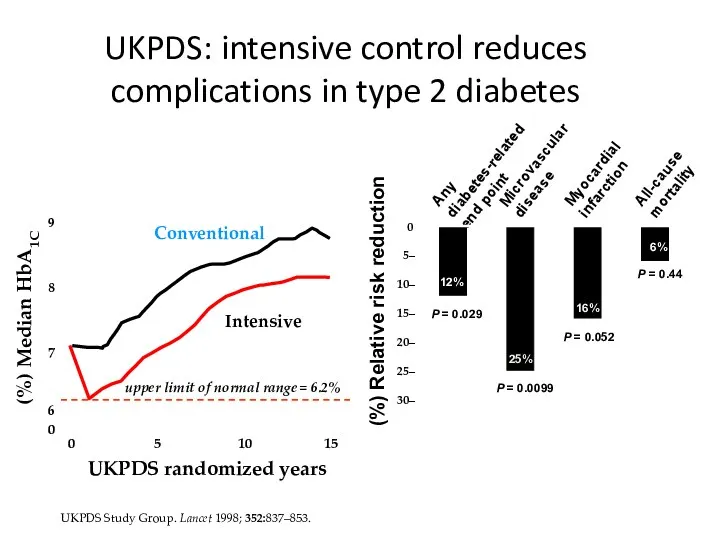
UKPDS Study Group. Lancet 1998; 352:837–853.
UKPDS: intensive control reduces complications
UKPDS Study Group. Lancet 1998; 352:837–853.
UKPDS: intensive control reduces complications
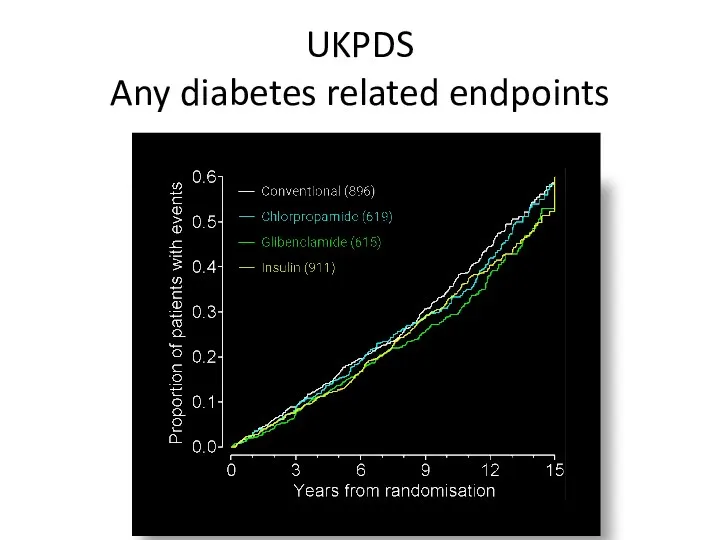
UKPDS
Any diabetes related endpoints
UKPDS
Any diabetes related endpoints
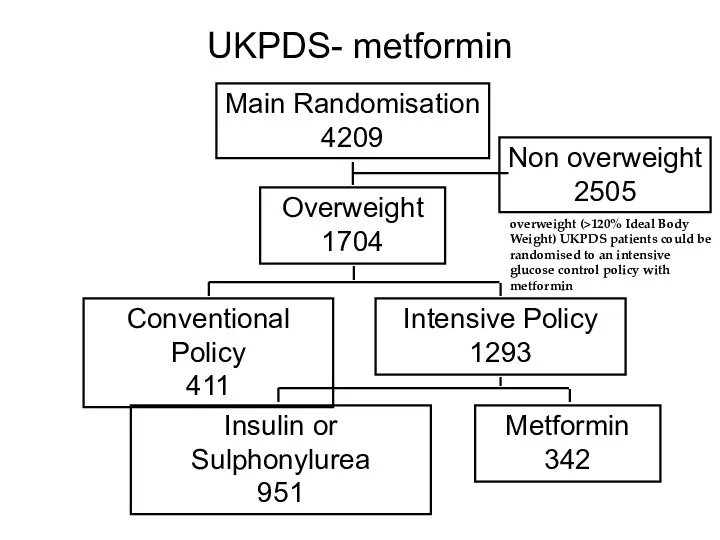
UKPDS- metformin
Main Randomisation
4209
Overweight
1704
Non overweight
2505
Conventional Policy
411
Intensive Policy
1293
Metformin
342
Insulin or Sulphonylurea
951
overweight (>120% Ideal
UKPDS- metformin
Main Randomisation
4209
Overweight
1704
Non overweight
2505
Conventional Policy
411
Intensive Policy
1293
Metformin
342
Insulin or Sulphonylurea
951
overweight (>120% Ideal
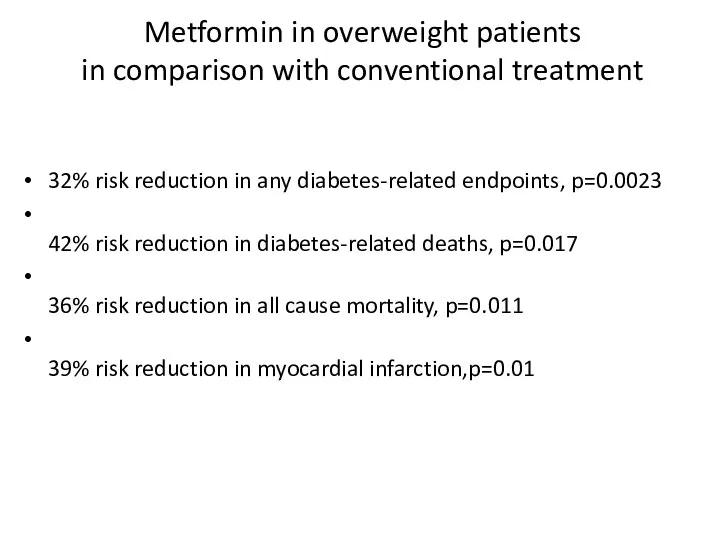
Metformin in overweight patients
in comparison with conventional treatment
32% risk reduction
Metformin in overweight patients
in comparison with conventional treatment
32% risk reduction
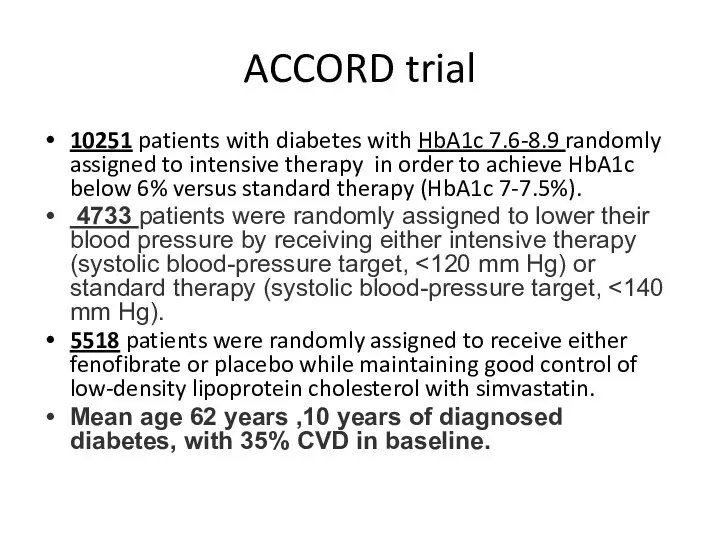
ACCORD trial
10251 patients with diabetes with HbA1c 7.6-8.9 randomly assigned
ACCORD trial
10251 patients with diabetes with HbA1c 7.6-8.9 randomly assigned
Treatment group
Treatment group
(ACCORD study (glycemic arm
(ACCORD study (glycemic arm
Gerstein HC et al. The ACCORD Study Group. N Engl J
Gerstein HC et al. The ACCORD Study Group. N Engl J
ACCORD study
glycemic group
ACCORD study
glycemic group
ADVANCE collaborative group
ADVANCE collaborative group
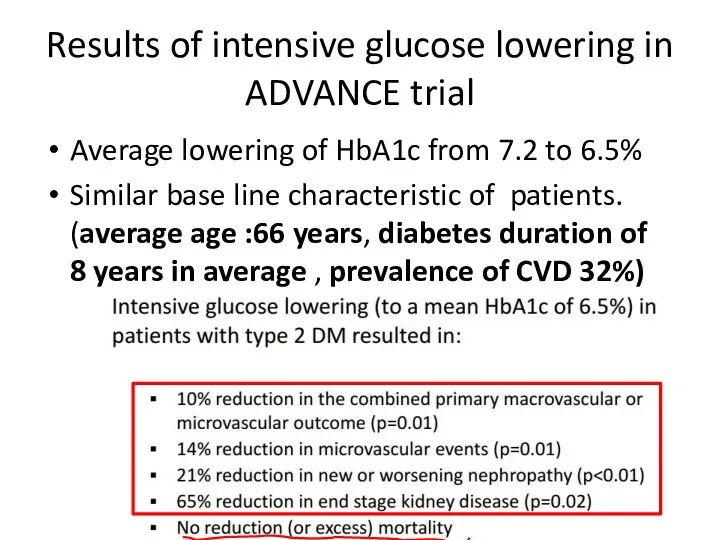
Results of intensive glucose lowering in ADVANCE trial
Average lowering of HbA1c
Results of intensive glucose lowering in ADVANCE trial
Average lowering of HbA1c
VA Diabetes Trial (VADT)
Similar study design: intensive therapy versus standard therapy.
Primary
VA Diabetes Trial (VADT)
Similar study design: intensive therapy versus standard therapy.
Primary
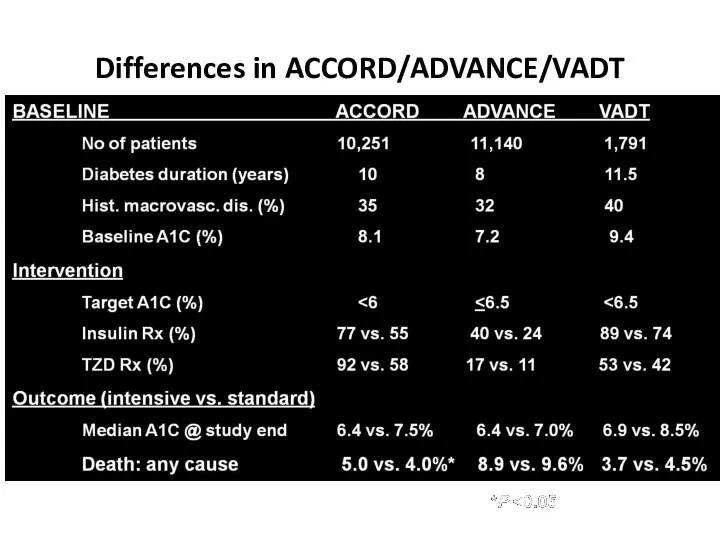
Differences in ACCORD/ADVANCE/VADT
Skyler JS, Bergenstal R, Bonow RO, et al.
Differences in ACCORD/ADVANCE/VADT
Skyler JS, Bergenstal R, Bonow RO, et al.
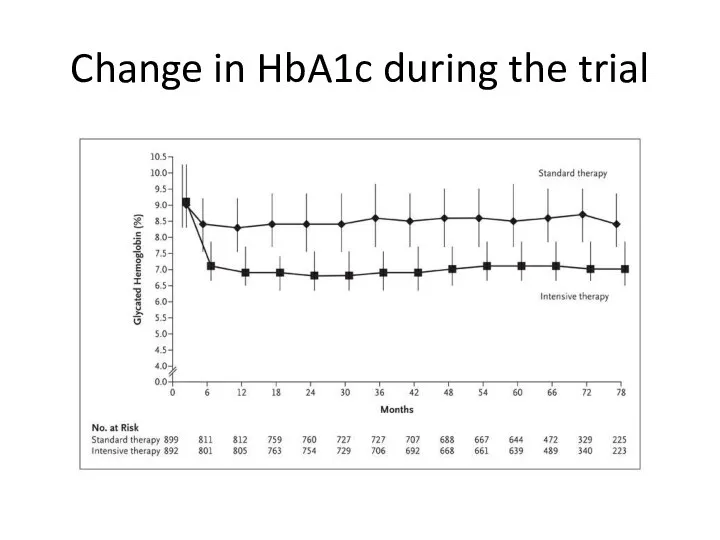
Change in HbA1c during the trial
Change in HbA1c during the trial
Initial results
No excess of cardiovascular mortality.
No improvement of cardiovascular morbidity.
No change
Initial results
No excess of cardiovascular mortality.
No improvement of cardiovascular morbidity.
No change
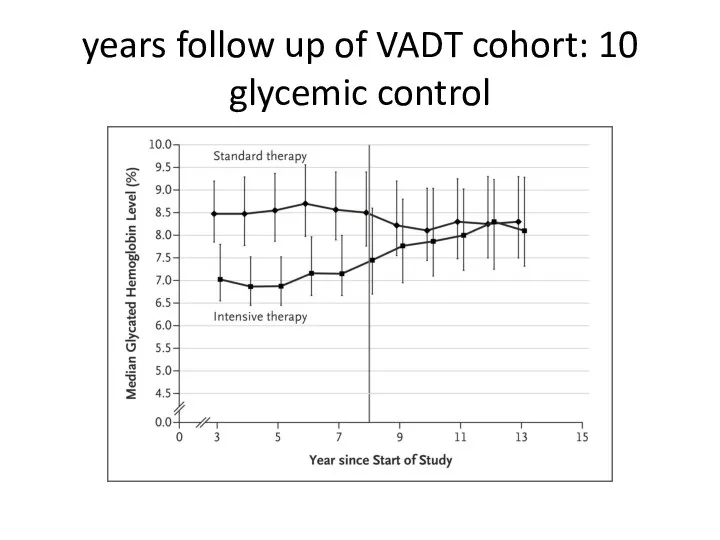
10 years follow up of VADT cohort: glycemic control
10 years follow up of VADT cohort: glycemic control
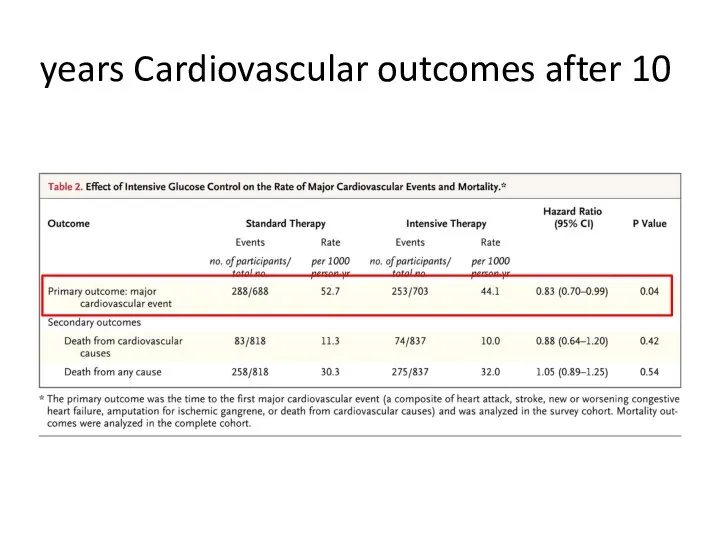
Cardiovascular outcomes after 10 years
Cardiovascular outcomes after 10 years
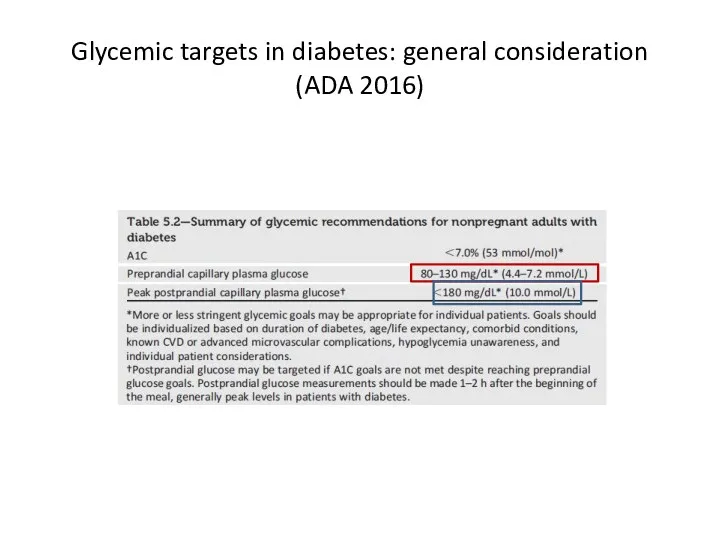
Glycemic targets in diabetes: general consideration
(ADA 2016)
Glycemic targets in diabetes: general consideration
(ADA 2016)
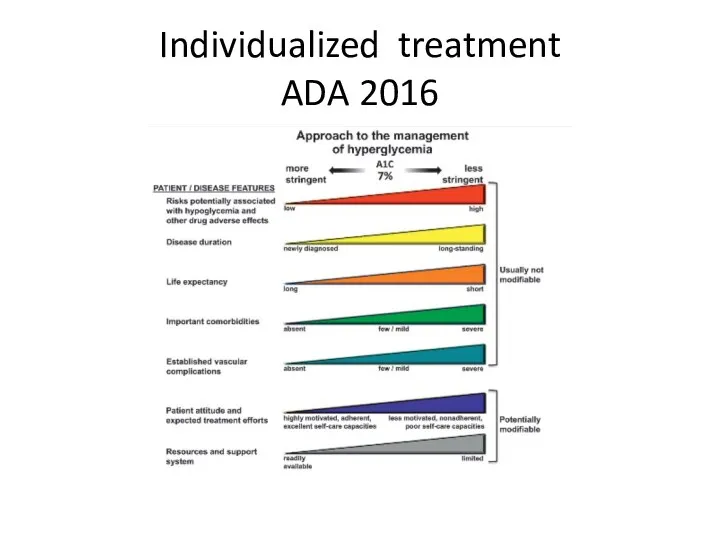
Individualized treatment
ADA 2016
Individualized treatment
ADA 2016
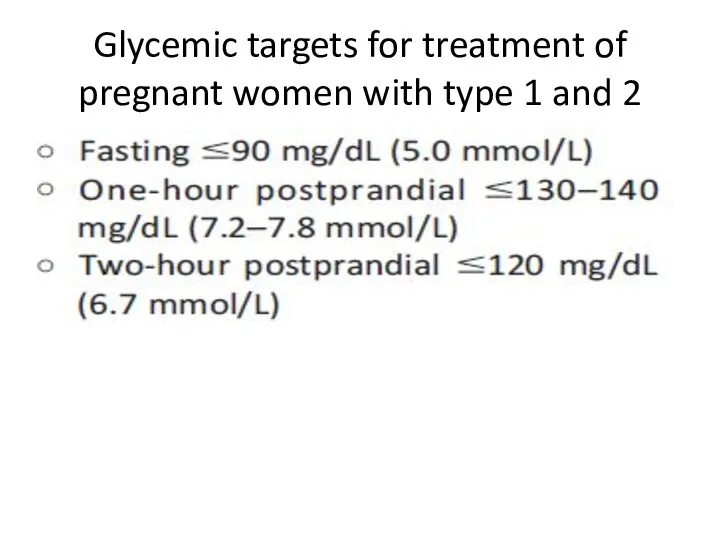
Glycemic targets for treatment of pregnant women with type 1 and
Glycemic targets for treatment of pregnant women with type 1 and
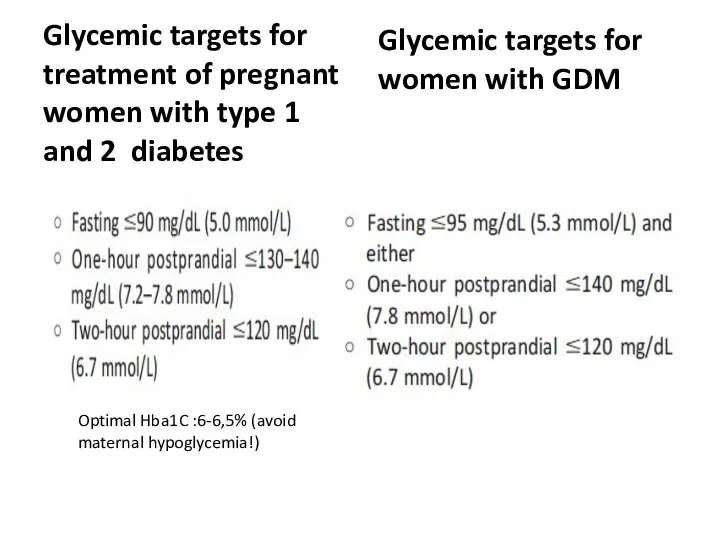
Glycemic targets for treatment of pregnant women with type 1 and
Glycemic targets for treatment of pregnant women with type 1 and
Type 1 insulin treatment
Concept of basal - bolus
Prescription of short
Type 1 insulin treatment
Concept of basal - bolus
Prescription of short
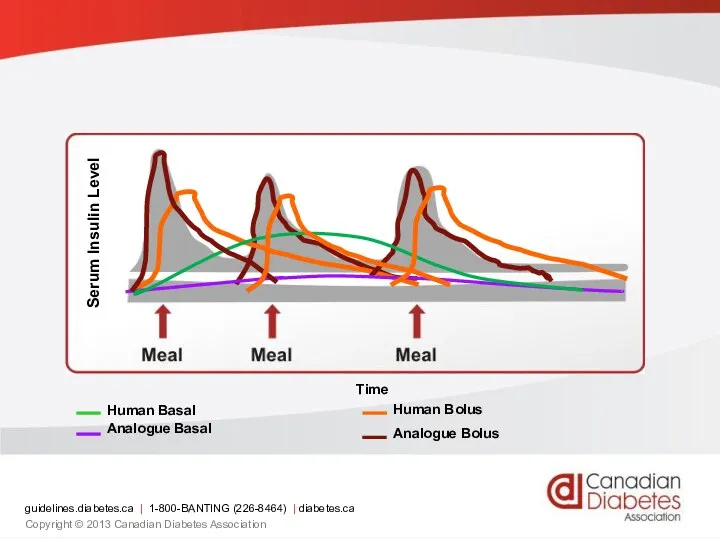
Serum Insulin Level
Time
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Copyright © 2013 Canadian
Serum Insulin Level
Time
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Copyright © 2013 Canadian
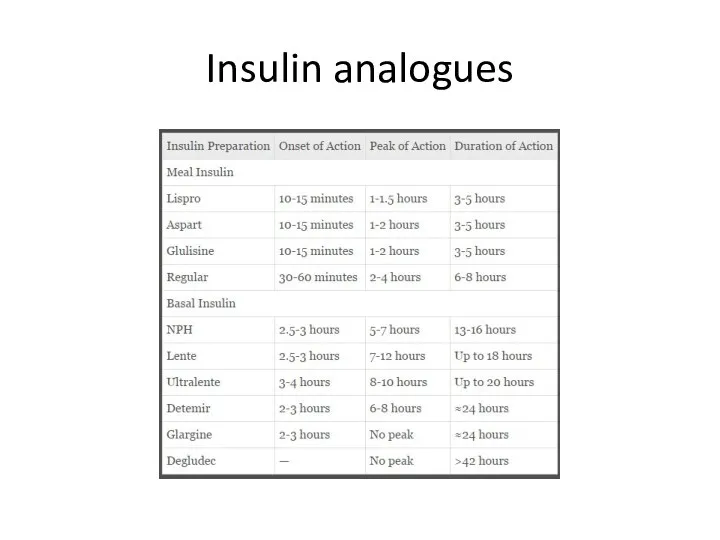
Insulin analogues
Insulin analogues
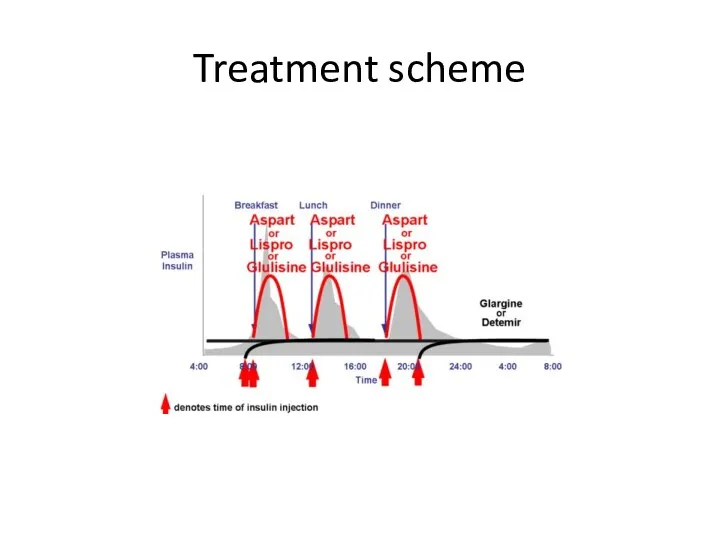
Treatment scheme
Treatment scheme
:Principles of type 2 treatment
(1)non –pharmacologic therapy
Physical activity.
1.1Minimum 150 minutes
:Principles of type 2 treatment
(1)non –pharmacologic therapy
Physical activity.
1.1Minimum 150 minutes
:Principles of type 2 treatment
(2)non –pharmacologic therapy
Diet and carbohydrates
500-750 kcal/d deficit:1200-1500
:Principles of type 2 treatment
(2)non –pharmacologic therapy
Diet and carbohydrates
500-750 kcal/d deficit:1200-1500
:Principles of type 2 treatment
(3)non –pharmacologic therapy
Diet and proteins
0.8 g/kg daily
:Principles of type 2 treatment
(3)non –pharmacologic therapy
Diet and proteins
0.8 g/kg daily
Pharmacological treatment of glycemia type 2:drug classification
Biguanides
Secretagogues
DPP4 inhibitors
α- glycosidase inhibitor
Thiazolidinedione
GLP1 agonists
SGLT2
Pharmacological treatment of glycemia type 2:drug classification
Biguanides
Secretagogues
DPP4 inhibitors
α- glycosidase inhibitor
Thiazolidinedione
GLP1 agonists
SGLT2
Biguanides
Metfomin(Glucomin,Glucophage)
Preferred initial pharmacologic agent because of long standing record of efficacy
Biguanides
Metfomin(Glucomin,Glucophage)
Preferred initial pharmacologic agent because of long standing record of efficacy
Metformin
Half-life up to 3 hour.
No metabolism ,excreted by kidney as active
Metformin
Half-life up to 3 hour.
No metabolism ,excreted by kidney as active
Metformin toxicity and side effects
Gastrointestinal (20-30%): start with lower dose with
Metformin toxicity and side effects
Gastrointestinal (20-30%): start with lower dose with
Secretagogues
Sulfonylureas: bind to SUR1 site of inward rectified KATP channel on
Secretagogues
Sulfonylureas: bind to SUR1 site of inward rectified KATP channel on
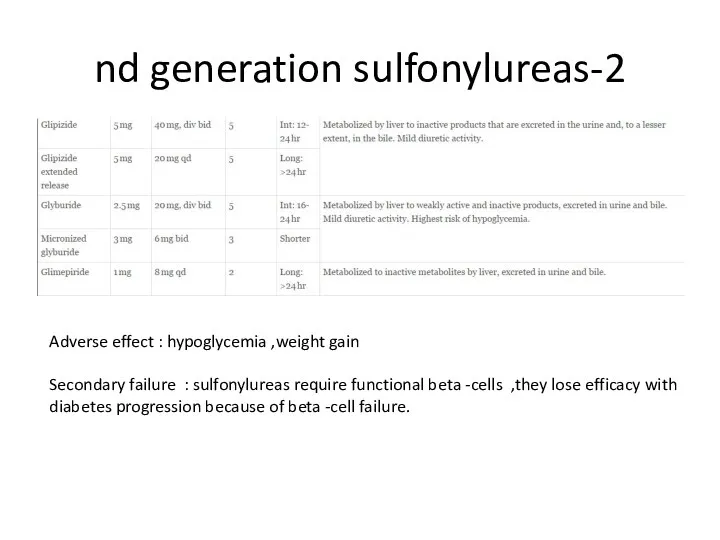
2-nd generation sulfonylureas
Adverse effect : hypoglycemia ,weight gain
Secondary failure : sulfonylureas
2-nd generation sulfonylureas
Adverse effect : hypoglycemia ,weight gain
Secondary failure : sulfonylureas
Glinides
Binding to distinct (from sulfonylurea) SUR 1 site
Burst phase-1 insulin
Glinides
Binding to distinct (from sulfonylurea) SUR 1 site
Burst phase-1 insulin
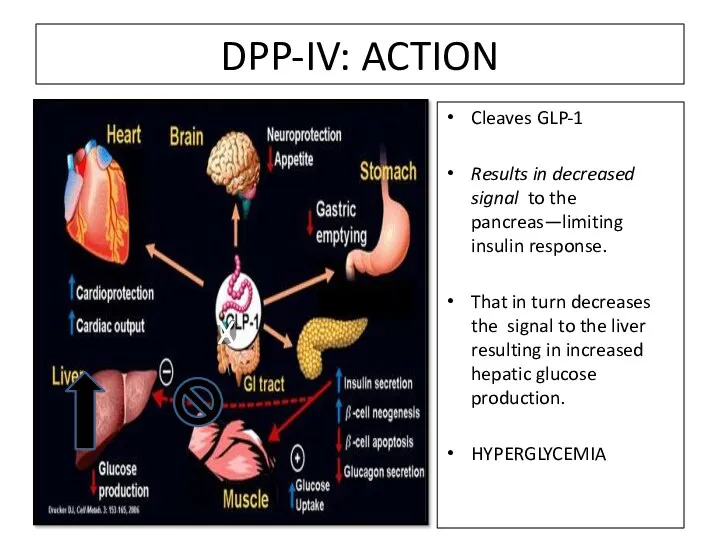
DPP-IV: ACTION
Cleaves GLP-1
Results in decreased signal to the pancreas—limiting insulin response.
That
DPP-IV: ACTION
Cleaves GLP-1
Results in decreased signal to the pancreas—limiting insulin response.
That
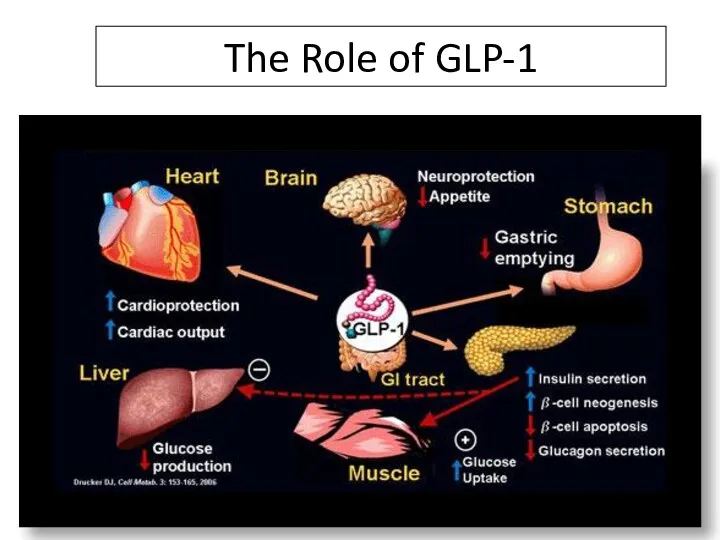
The Role of GLP-1
DPP-4 Inhibitors Increase ½ Life of GLP-1
The Role of GLP-1
DPP-4 Inhibitors Increase ½ Life of GLP-1
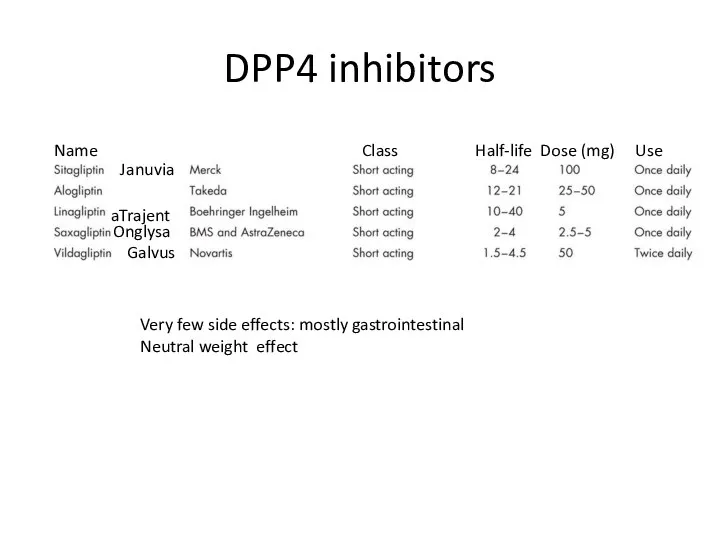
DPP4 inhibitors
Januvia
Trajenta
Onglysa
Galvus
Name Class Half-life Dose (mg) Use
Very few side effects: mostly
DPP4 inhibitors
Januvia
Trajenta
Onglysa
Galvus
Name Class Half-life Dose (mg) Use
Very few side effects: mostly
GLP1 agonists(injectable agents)
Breakthrough in DM 2 treatment
Glycemic ,cardiovascular (LEADER study)benefit ,
GLP1 agonists(injectable agents)
Breakthrough in DM 2 treatment
Glycemic ,cardiovascular (LEADER study)benefit ,
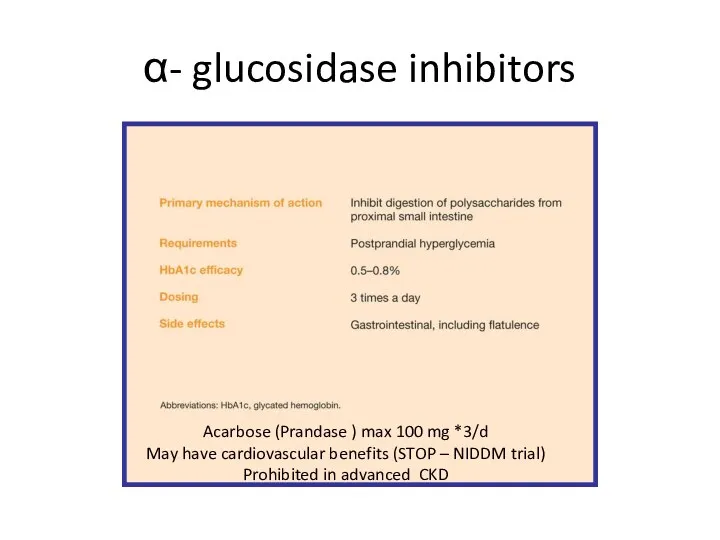
α- glucosidase inhibitors
Acarbose (Prandase ) max 100 mg *3/d
May have cardiovascular
α- glucosidase inhibitors
Acarbose (Prandase ) max 100 mg *3/d
May have cardiovascular
Thiazolidinediones
Gamma- PPAR agonists.
Increase of insulin sensitivity in adipose tissue skeletal muscle
Thiazolidinediones
Gamma- PPAR agonists.
Increase of insulin sensitivity in adipose tissue skeletal muscle
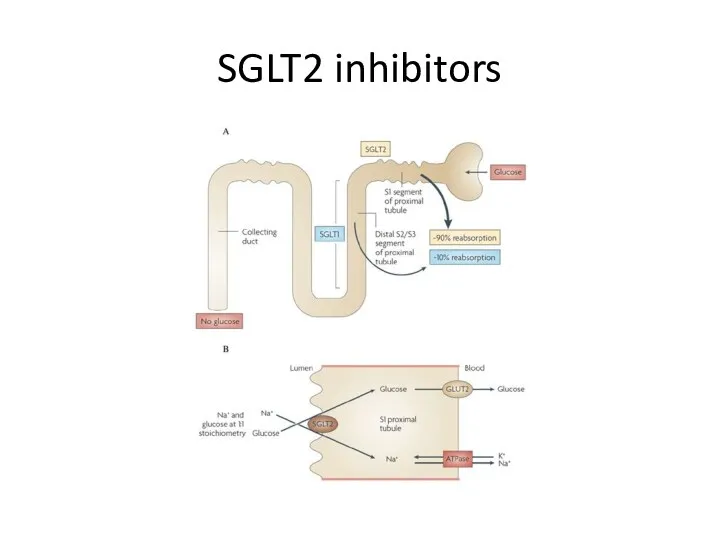
SGLT2 inhibitors
SGLT2 inhibitors
SGLT2 inhibitors medications
Empafliglozin (Jardiance)10 mg ,25 mg
Dapafliglozin(Forxiga) 10 mg
Positive
SGLT2 inhibitors medications
Empafliglozin (Jardiance)10 mg ,25 mg
Dapafliglozin(Forxiga) 10 mg
Positive
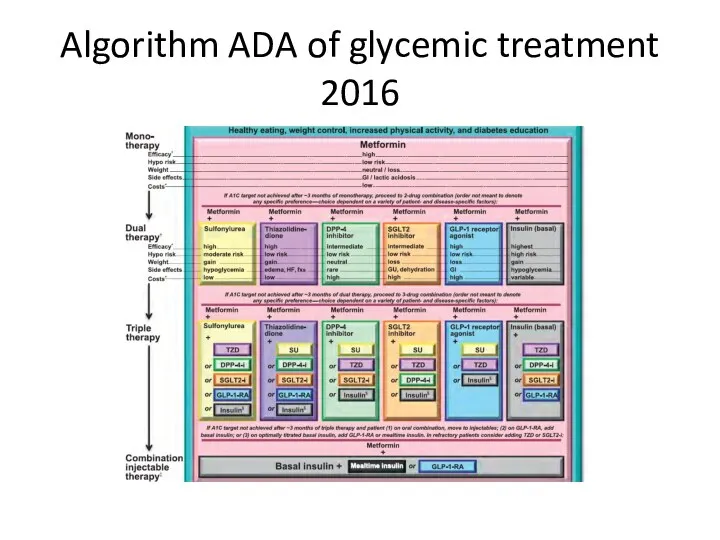
Algorithm ADA of glycemic treatment
2016
Algorithm ADA of glycemic treatment
2016
Comprehensive care of diabetes(ADA 2016)
Stop smoking.
Treat blood pressure to targets
Comprehensive care of diabetes(ADA 2016)
Stop smoking.
Treat blood pressure to targets
Statin treatment and diabetes
Patients 40-75 without additional atherosclerotic cardiovascular disease(ACVD)
Statin treatment and diabetes
Patients 40-75 without additional atherosclerotic cardiovascular disease(ACVD)
 Дифтерия: этиология, классификация, клиника, лечение
Дифтерия: этиология, классификация, клиника, лечение Оптическая когерентная томография
Оптическая когерентная томография Материаловедение. Лекция 9
Материаловедение. Лекция 9 Тактика лечение язвенной болезни (показания к оперативному лечению)
Тактика лечение язвенной болезни (показания к оперативному лечению) Патохимия, диагностика и коррекция нарушений обмена углеводов у детей (сахарный диабет, галактоземия, фруктоземия)
Патохимия, диагностика и коррекция нарушений обмена углеводов у детей (сахарный диабет, галактоземия, фруктоземия) Опухоли яичка
Опухоли яичка Клиника интеллектуальных нарушений
Клиника интеллектуальных нарушений Hemopoiesis. Immunology
Hemopoiesis. Immunology Методы исследования лимфаузлов и внутренних органов при заболеваниях крови
Методы исследования лимфаузлов и внутренних органов при заболеваниях крови Риск-менеджмент. Рисктердің медициналық көмек көрсету процессі мен байланысы
Риск-менеджмент. Рисктердің медициналық көмек көрсету процессі мен байланысы Тромбоэмболия ветвей легочной артерии: патофизиология, клиника, диагностика, лечение
Тромбоэмболия ветвей легочной артерии: патофизиология, клиника, диагностика, лечение Нейроинфекции. История изучения менингитов
Нейроинфекции. История изучения менингитов ЖАҚК (жалпы айналымдағы қан көлемі) және құрам бөліктерінің жеткіліксіздігін анықтау әдістері
ЖАҚК (жалпы айналымдағы қан көлемі) және құрам бөліктерінің жеткіліксіздігін анықтау әдістері Сосудистые заболевания нервной системы
Сосудистые заболевания нервной системы Эффективный контракт медицинской сестры
Эффективный контракт медицинской сестры Контроль качества клинических лабораторных исследований
Контроль качества клинических лабораторных исследований Генитальный герпес
Генитальный герпес Хронический лимфолейкоз
Хронический лимфолейкоз Вирусные кишечные инфекции
Вирусные кишечные инфекции Мәйітпен жұмыс жасау
Мәйітпен жұмыс жасау Расстройства ощущений и восприятия
Расстройства ощущений и восприятия Врождённые заболевания
Врождённые заболевания Острый живот
Острый живот Луи Пастер
Луи Пастер Сергиево-Посадский детский дом слепоглухих. Образовательные программы
Сергиево-Посадский детский дом слепоглухих. Образовательные программы Инфекции, передаваемые половым путём
Инфекции, передаваемые половым путём Спинальные амиотрофии
Спинальные амиотрофии Сибирская язва сельскохозяйственных животных
Сибирская язва сельскохозяйственных животных