- Colorectal cancer

Содержание
- 2. Epidemiology Colon and rectum cancer accounted for about 1 million new cases in 2002 (9,4% of
- 3. In Europe and North-America colorectal cancer is a rather common malignant disease and it ranks with
- 4. Epidemiology
- 5. Incidence of colorectal cancer (all countries, 2002)
- 6. RISK FACTORS, COLONIC CARCINOMA Familial adenomatous polyposis syndrome Hereditary factors Ulcerative colitis Crohn's colitis Schistosomal colitis
- 7. Familial adenomatous polyposis
- 8. Gardner syndrome
- 9. LARGE POLYP IN THE SIGMOID COLON
- 10. Macroscopic local growth Cancers of coecum and ascending colon are mainly papillomatous tumors. Because the coecum
- 11. Macroscopic local growth Cancers of the descending colon and sigmoid usually grow circumferential in the intestinal
- 12. Lymphogenic spread
- 13. Haematogenic spread of colorectal cancer
- 14. Metastases of colorectal cancer in lung
- 15. METASTASES COLORECTAL CANCER IN LIVER
- 16. METASTASES COLORECTAL CANCER IN LIVER
- 17. Presenting problems In general, complaints caused by a colorectal cancer occur late. The site of tumor
- 18. Successive complaints and symptoms due to cancer of the colon descendens or a sigmoid cancer are:
- 19. When there is suspicion of a sigmoid cancer it is important to ask if there has
- 20. DATA FORM FOR CANCER STAGING - COLORECTAL PRIMARY TUMOR (T) TX - Primary tumor cannot be
- 21. STAGE GROUPING
- 22. Colonoscopy
- 23. Polyp on stalk - polypectomy
- 24. Colonic adenocarcinoma at 20 cm, Grade II, arising in an adenomatous polyp
- 25. Rectal cancer
- 26. Treatment of colorectal cancer The treatment of choice is surgery for treatment with curative intent of
- 27. RIGHT HEMICOLECTOMY
- 28. In surgery for rectal cancer there is is always the question of whether the anus can
- 29. RESECTION OF COLORECTAL CANCER’S METASTASIS IN LIVER
- 31. Скачать презентацию
Epidemiology
Colon and rectum cancer accounted for about 1 million new cases
Epidemiology
Colon and rectum cancer accounted for about 1 million new cases
In Europe and North-America colorectal cancer is a rather common malignant
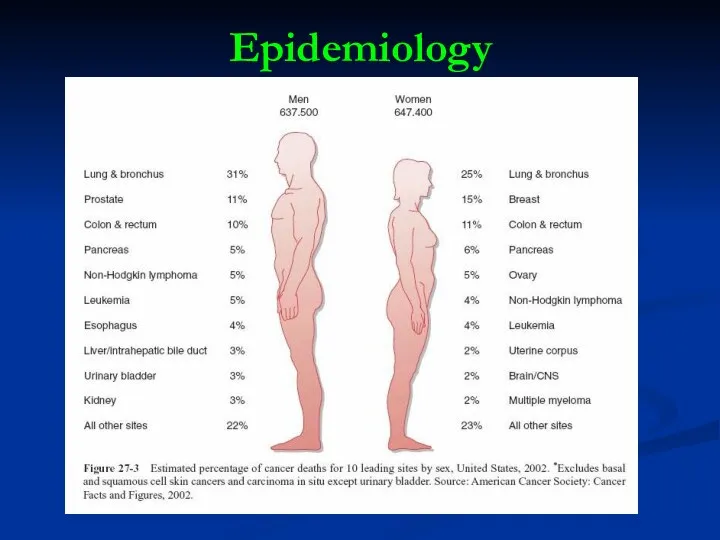
Epidemiology
Epidemiology
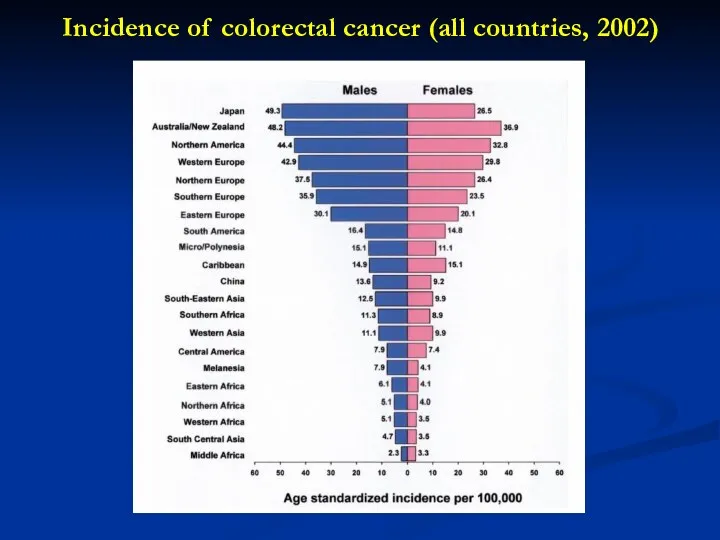
Incidence of colorectal cancer (all countries, 2002)
Incidence of colorectal cancer (all countries, 2002)
RISK FACTORS, COLONIC CARCINOMA
Familial adenomatous polyposis syndrome
Hereditary factors
RISK FACTORS, COLONIC CARCINOMA
Familial adenomatous polyposis syndrome
Hereditary factors
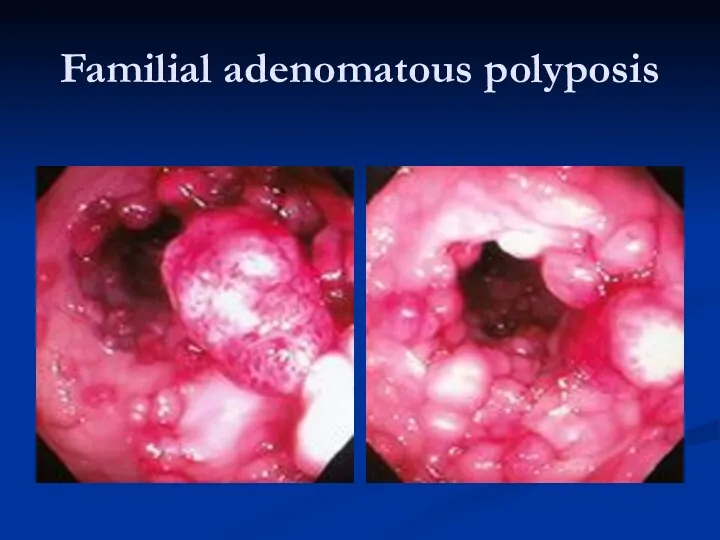
Familial adenomatous polyposis
Familial adenomatous polyposis

Gardner syndrome
Gardner syndrome
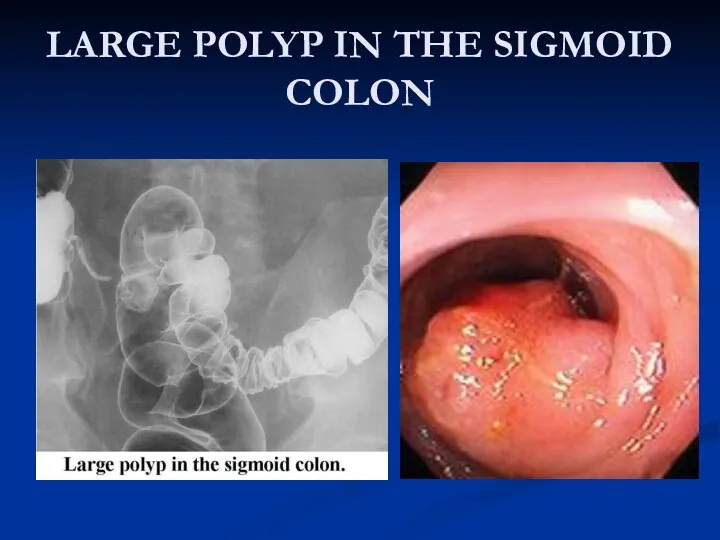
LARGE POLYP IN THE SIGMOID COLON
LARGE POLYP IN THE SIGMOID COLON
Macroscopic local growth
Cancers of coecum and ascending colon are mainly papillomatous
Macroscopic local growth
Cancers of coecum and ascending colon are mainly papillomatous
Macroscopic local growth
Cancers of the descending colon and sigmoid usually grow
Macroscopic local growth
Cancers of the descending colon and sigmoid usually grow
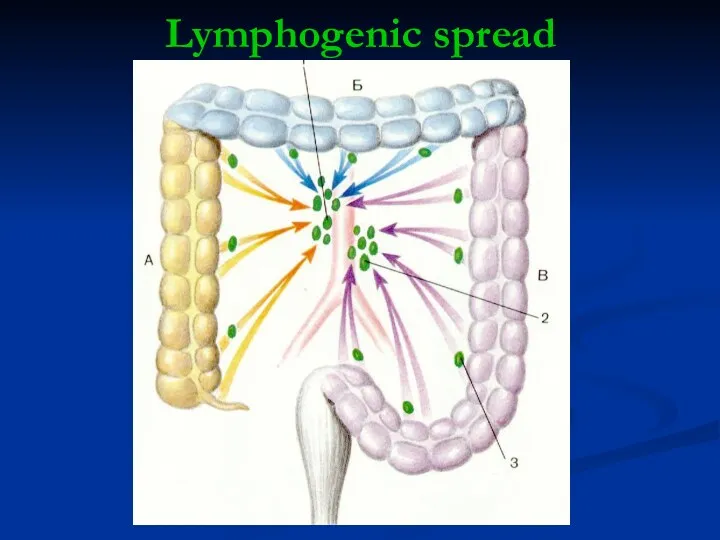
Lymphogenic spread
Lymphogenic spread
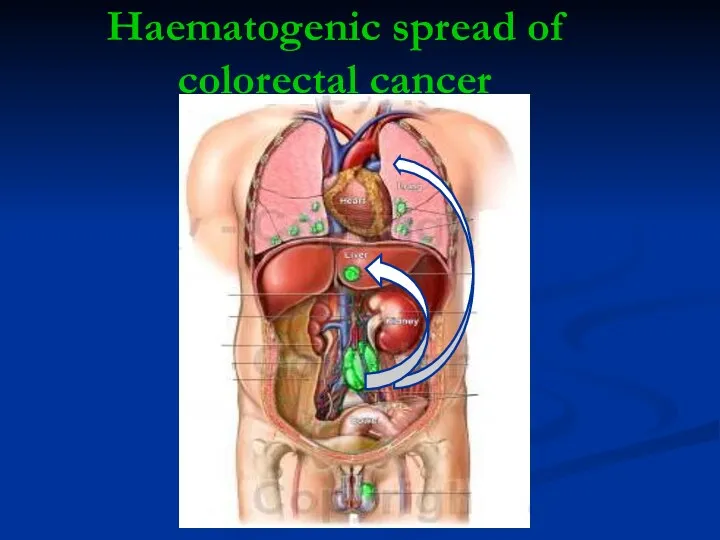
Haematogenic spread of
colorectal cancer
Haematogenic spread of
colorectal cancer
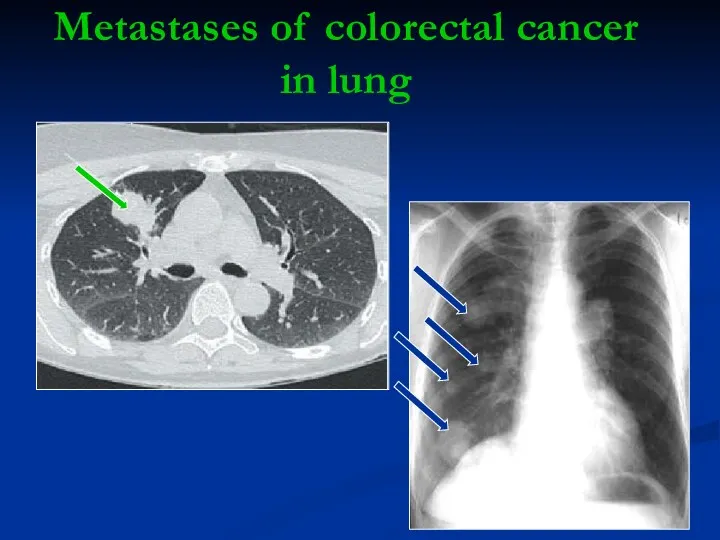
Metastases of colorectal cancer
in lung
Metastases of colorectal cancer
in lung
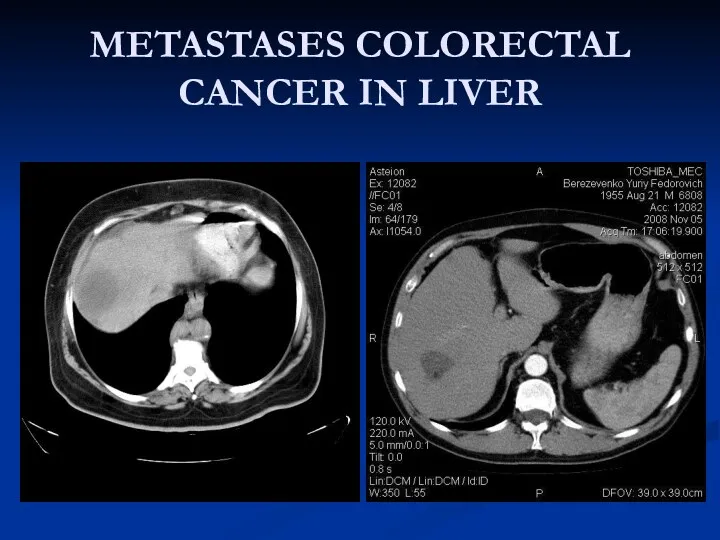
METASTASES COLORECTAL CANCER IN LIVER
METASTASES COLORECTAL CANCER IN LIVER
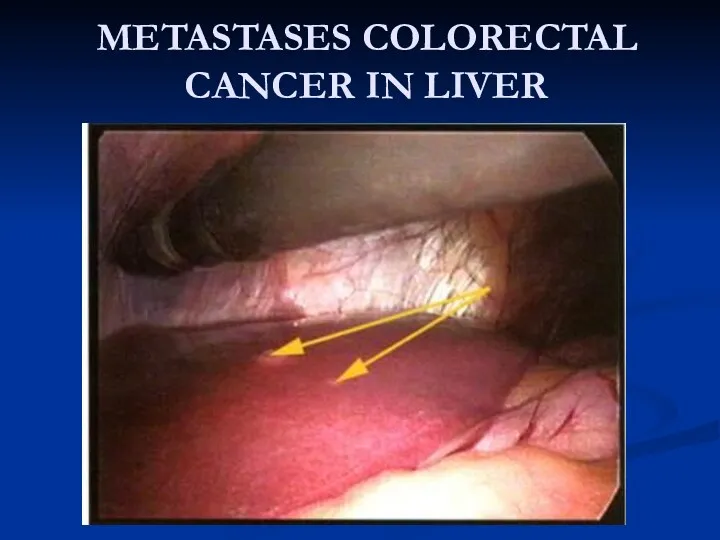
METASTASES COLORECTAL CANCER IN LIVER
METASTASES COLORECTAL CANCER IN LIVER
Presenting problems
In general, complaints caused by a colorectal cancer occur late.
Presenting problems
In general, complaints caused by a colorectal cancer occur late.
Successive complaints and symptoms due to cancer of the colon descendens
Successive complaints and symptoms due to cancer of the colon descendens
When there is suspicion of a sigmoid cancer it is important
When there is suspicion of a sigmoid cancer it is important
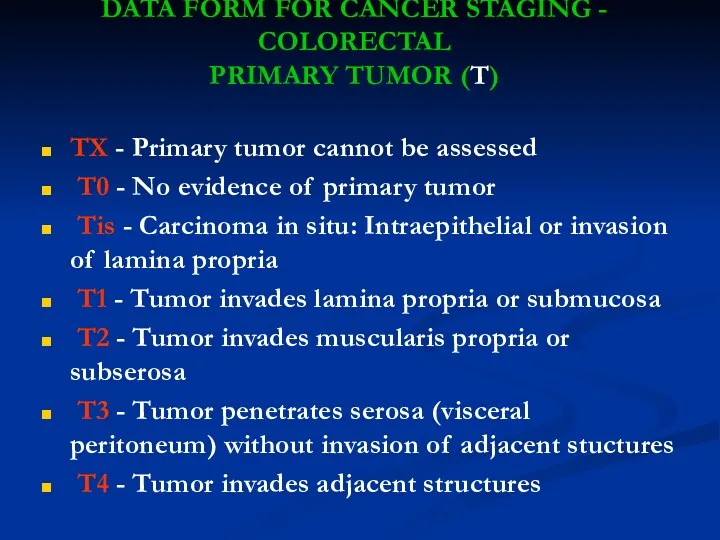
DATA FORM FOR CANCER STAGING - COLORECTAL
PRIMARY TUMOR (T)
TX -
DATA FORM FOR CANCER STAGING - COLORECTAL
PRIMARY TUMOR (T)
TX -

STAGE GROUPING
STAGE GROUPING
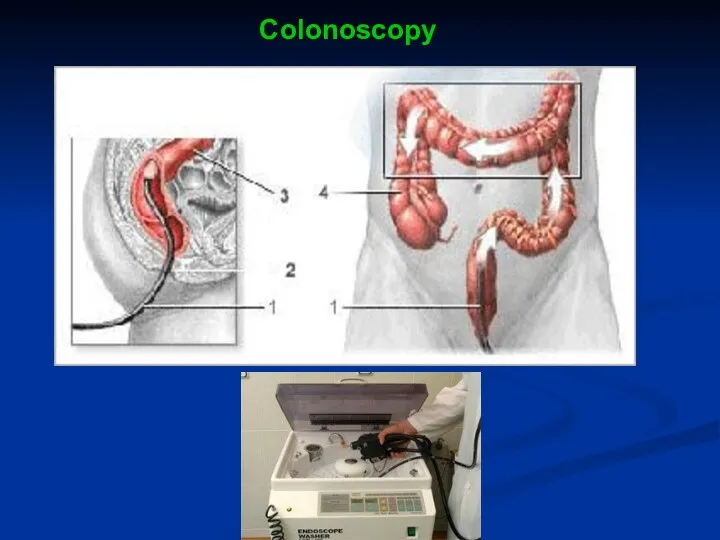
Colonoscopy
Colonoscopy
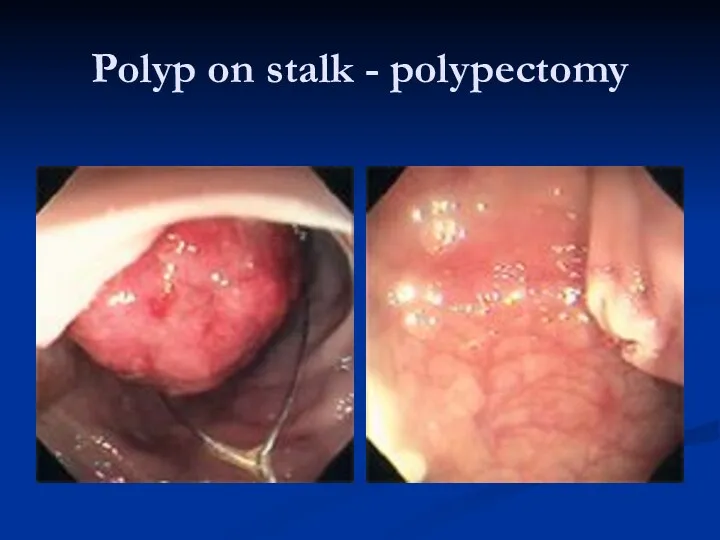
Polyp on stalk - polypectomy
Polyp on stalk - polypectomy
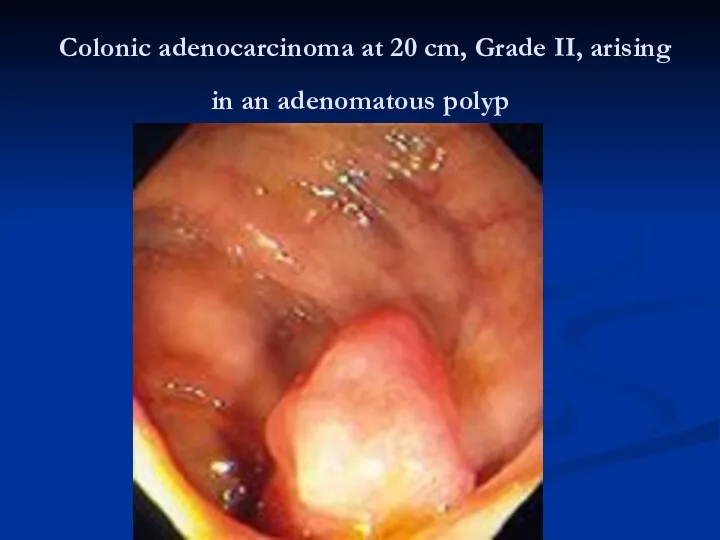
Colonic adenocarcinoma at 20 cm, Grade II, arising in an
Colonic adenocarcinoma at 20 cm, Grade II, arising in an

Rectal cancer
Rectal cancer
Treatment of colorectal cancer
The treatment of choice is surgery for treatment
Treatment of colorectal cancer
The treatment of choice is surgery for treatment
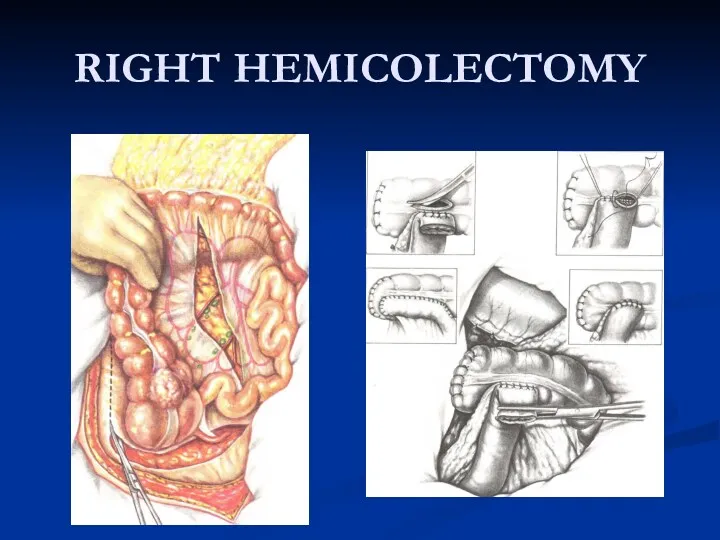
RIGHT HEMICOLECTOMY
RIGHT HEMICOLECTOMY
In surgery for rectal cancer there is is always the question
In surgery for rectal cancer there is is always the question
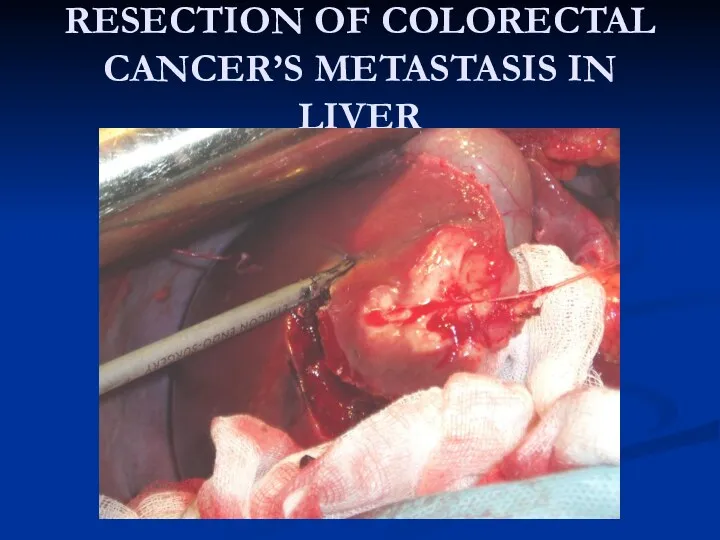
RESECTION OF COLORECTAL CANCER’S METASTASIS IN LIVER
RESECTION OF COLORECTAL CANCER’S METASTASIS IN LIVER
 Всероссийская служба медицины катастроф. Основы лечебно-эвакуационного обеспечения населения в ЧС мирного и военного времени
Всероссийская служба медицины катастроф. Основы лечебно-эвакуационного обеспечения населения в ЧС мирного и военного времени Основи мікробіології
Основи мікробіології Холера. Патогенез холеры
Холера. Патогенез холеры Мүмкіндіктері шектеулі науқастармен қарым-қатынас
Мүмкіндіктері шектеулі науқастармен қарым-қатынас Первичная хирургическая обработка ран ЧЛО
Первичная хирургическая обработка ран ЧЛО COVID-19
COVID-19 Іш сүзегі. Шигеллез
Іш сүзегі. Шигеллез Подготовка к инструмент методам исследования
Подготовка к инструмент методам исследования Панкреонекроз
Панкреонекроз Физиологическая классификация физических упражнений
Физиологическая классификация физических упражнений Эндокринная система
Эндокринная система Основы антисептики и асептики
Основы антисептики и асептики Лекция 22. Обмен веществ и энергии
Лекция 22. Обмен веществ и энергии Первичная профилактика сосудистой деменции
Первичная профилактика сосудистой деменции Общая гигиена. Климат. (Лекция 12-13)
Общая гигиена. Климат. (Лекция 12-13) Применение лекарственных средств, используемых при сердечно-сосудистых заболеваниях у беременных и родильниц
Применение лекарственных средств, используемых при сердечно-сосудистых заболеваниях у беременных и родильниц Люмбальная пункция. Показания и противопоказания к проведению люмбальной пункции
Люмбальная пункция. Показания и противопоказания к проведению люмбальной пункции Диабетическая нефропатия
Диабетическая нефропатия Gastrointestinal diseases : stomach cancer, colitis
Gastrointestinal diseases : stomach cancer, colitis Бронхиальная астма. ХОБЛ
Бронхиальная астма. ХОБЛ Зубные пасты и ополаскиватели, используемые при воспалительных заболеваниях пародонта
Зубные пасты и ополаскиватели, используемые при воспалительных заболеваниях пародонта Эндокринология. Гипогонадизм. (Лекция 8)
Эндокринология. Гипогонадизм. (Лекция 8) Симуляционный курс по неотложным состояниям
Симуляционный курс по неотложным состояниям Медицинская гельминтология. Возбудители гельминтозов
Медицинская гельминтология. Возбудители гельминтозов Arenaviruses: unique virology. Diseases of the Old World and New World
Arenaviruses: unique virology. Diseases of the Old World and New World Артериальная гипертония
Артериальная гипертония The Role of University Clinics in Treating for Teaching
The Role of University Clinics in Treating for Teaching Primary and secondary tuberculosis. (Lecture 5)
Primary and secondary tuberculosis. (Lecture 5)