- Gallstones (Cholelithiasis)

Содержание
- 2. Gallstone (Cholelithiasis) is a chronic recurrent hepatobiliary disease, the basis for which is the impaired metabolism
- 3. Epidemiology GD is a common disorder all over the world. The prevalence of GD varies widely
- 4. Prevalence rates of gallstones as determined by ultrasonography (Stinton L.M, Shaffer E.A, Gut and Liver 2016)
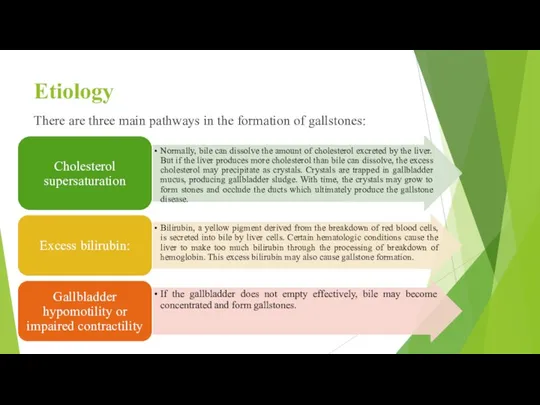
- 5. Etiology There are three main pathways in the formation of gallstones:
- 6. Etiology Depending on the etiology, gallstones have different compositions. The three most common types are cholesterol
- 7. Diagram of steroid hormones-induced inhibition of cholesterol catabolism. Drugs: estrogens, prednisolone, cyclosporine, azathioprine, sandostatin, clofibrate, nicotinic
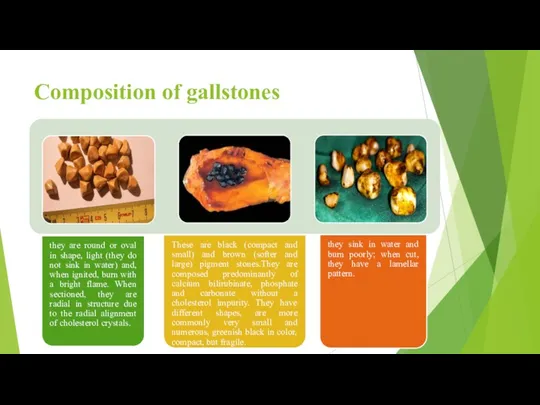
- 8. Composition of gallstones Stones in the gallbladder and/or bile ducts are a morphological substrate of GD.
- 9. Composition of gallstones
- 10. Pathogenesis The pathogenesis of GD is suggested to be multifactorial and probably develops from complex interactions
- 11. Cholesterol stones are formed in the gallbladder due to impaired relationships between the major bile components,
- 12. It shows a diagram of gallstone formation by taking into account the above impaired bile production
- 13. Symptoms and Signs About 80% of people with gallstones are asymptomatic. The remainder have symptoms ranging
- 14. Diagnosis Ultrasonography Gallstones are suspected in patients with biliary colic. Abdominal ultrasonography is the imaging test
- 17. Treatment For symptomatic stones: Laparoscopic cholecystectomy or sometimes stone dissolution using ursodeoxycholic acid. For asymptomatic stones:
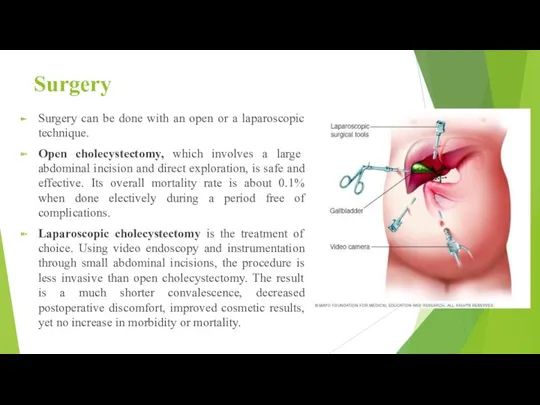
- 18. Surgery Surgery can be done with an open or a laparoscopic technique. Open cholecystectomy, which involves
- 19. Stone dissolution For patients who decline surgery or who are at high surgical risk, gallbladder stones
- 20. Prognosis The outlook for patients with symptomatic cholelithiasis managed by cholecystectomy is favourable. The same holds
- 22. Скачать презентацию
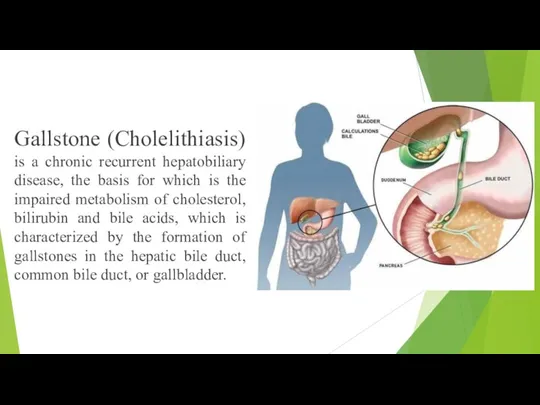
Gallstone (Cholelithiasis) is a chronic recurrent hepatobiliary disease, the basis for
Gallstone (Cholelithiasis) is a chronic recurrent hepatobiliary disease, the basis for
Epidemiology
GD is a common disorder all over the world. The prevalence
Epidemiology
GD is a common disorder all over the world. The prevalence

Prevalence rates of gallstones as determined by ultrasonography
(Stinton L.M, Shaffer E.A, Gut
Prevalence rates of gallstones as determined by ultrasonography
(Stinton L.M, Shaffer E.A, Gut
Etiology
There are three main pathways in the formation of gallstones:
Etiology
There are three main pathways in the formation of gallstones:
Etiology
Depending on the etiology, gallstones have different compositions. The three most
Etiology
Depending on the etiology, gallstones have different compositions. The three most
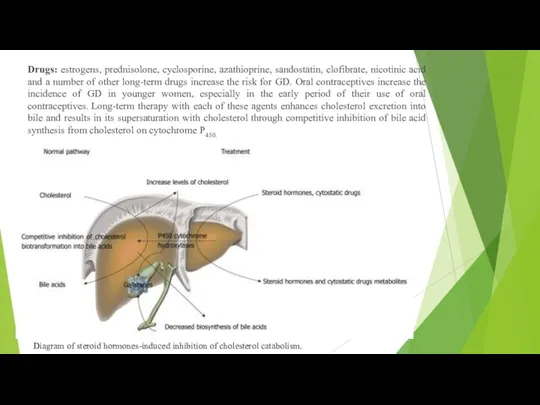
Diagram of steroid hormones-induced inhibition of cholesterol catabolism.
Drugs: estrogens, prednisolone, cyclosporine,
Diagram of steroid hormones-induced inhibition of cholesterol catabolism.
Drugs: estrogens, prednisolone, cyclosporine,

Composition of gallstones
Stones in the gallbladder and/or bile ducts are a
Composition of gallstones
Stones in the gallbladder and/or bile ducts are a
Composition of gallstones
Composition of gallstones
Pathogenesis
The pathogenesis of GD is suggested to be multifactorial and probably
Pathogenesis
The pathogenesis of GD is suggested to be multifactorial and probably
Cholesterol stones are formed in the gallbladder due to impaired relationships
Cholesterol stones are formed in the gallbladder due to impaired relationships
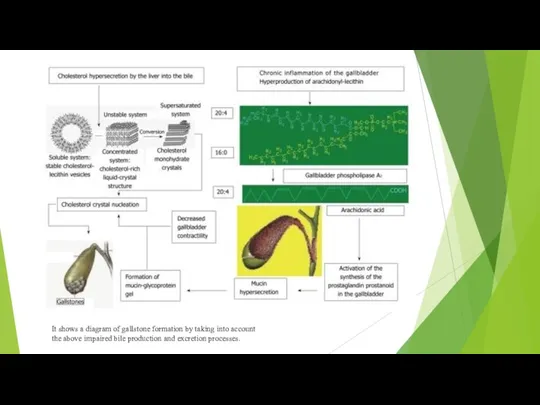
It shows a diagram of gallstone formation by taking into account
the
It shows a diagram of gallstone formation by taking into account
the
Symptoms and Signs
About 80% of people with gallstones are asymptomatic. The
Symptoms and Signs
About 80% of people with gallstones are asymptomatic. The
Diagnosis
Ultrasonography
Gallstones are suspected in patients with biliary colic. Abdominal ultrasonography is
Diagnosis
Ultrasonography
Gallstones are suspected in patients with biliary colic. Abdominal ultrasonography is


Treatment
For symptomatic stones: Laparoscopic cholecystectomy or sometimes stone dissolution using ursodeoxycholic
Treatment
For symptomatic stones: Laparoscopic cholecystectomy or sometimes stone dissolution using ursodeoxycholic
Surgery
Surgery can be done with an open or a laparoscopic technique.
Open
Surgery
Surgery can be done with an open or a laparoscopic technique.
Open
Stone dissolution
For patients who decline surgery or who are at high
Stone dissolution
For patients who decline surgery or who are at high
Prognosis
The outlook for patients with symptomatic cholelithiasis managed by cholecystectomy is
Prognosis
The outlook for patients with symptomatic cholelithiasis managed by cholecystectomy is
 ИВЛ-основы
ИВЛ-основы Контрацепция и планирование семьи
Контрацепция и планирование семьи Желчнокаменная болезнь и ее осложнения
Желчнокаменная болезнь и ее осложнения Диафрагмальные грыжи у детей
Диафрагмальные грыжи у детей Спадкові захворювання людини. Медико – генетичне консультування
Спадкові захворювання людини. Медико – генетичне консультування Segmental Stability of The Cervical Spine
Segmental Stability of The Cervical Spine Тері рагы
Тері рагы Прием пациента в стационар
Прием пациента в стационар Жедел кенелік энцефалит
Жедел кенелік энцефалит Гемолитико-уремический синдром
Гемолитико-уремический синдром Dermatomycosis. Pathogenesis
Dermatomycosis. Pathogenesis Острое повреждение легких (ALI) и острый респираторный дистресс-синдром (ARDS)
Острое повреждение легких (ALI) и острый респираторный дистресс-синдром (ARDS) Гемобластози у дітей
Гемобластози у дітей Актуальные вопросы кардиопрофилактики
Актуальные вопросы кардиопрофилактики Федеральный проект Демография
Федеральный проект Демография Синдромы помрачнения сознания: онейроид, сумеречное растройство сознания
Синдромы помрачнения сознания: онейроид, сумеречное растройство сознания Профилактика СПИДа. Классный час
Профилактика СПИДа. Классный час Ас қорыту жүйесі
Ас қорыту жүйесі Нейроинфекция у детей
Нейроинфекция у детей Первая доврачебная и врачебная помощь. Правовая основа
Первая доврачебная и врачебная помощь. Правовая основа Микропрепараты стоматологам на экзамен
Микропрепараты стоматологам на экзамен Кровезаменители. Кровезамещающие жидкости
Кровезаменители. Кровезамещающие жидкости Онкологиялық ауруларды ерте анықтау,скринингтік бағдарламалар ұйымдастыру және жүргізу
Онкологиялық ауруларды ерте анықтау,скринингтік бағдарламалар ұйымдастыру және жүргізу Рекомендованная вакцинация
Рекомендованная вакцинация Қабылдау бөлімі (сырқатты қабылдайтын жер)
Қабылдау бөлімі (сырқатты қабылдайтын жер) Продуктивное воспаление
Продуктивное воспаление Клиническая фармакокинетика
Клиническая фармакокинетика ВИЧ-инфекция и его профилактика
ВИЧ-инфекция и его профилактика